
Abstract
Background:
Knowledge is scarce about the impact of stroke in Uganda, and culturally adapted, psychometrically tested patient-reported outcome measures are lacking. The Stroke Impact Scale 3.0 is recommended, but it has not been culturally adapted and validated in Uganda.
Objective:
To culturally adapt and determine the psychometric properties of the Stroke Impact Scale 3.0 in the Ugandan context on a small scale.
Method:
The Stroke Impact Scale 3.0 was culturally adapted to form Stroke Impact Scale 3.0 Uganda (in English) by involving 25 participants in three different expert committees. Subsequently, Stroke Impact Scale 3.0 Uganda from English to Luganda language was done in accordance with guidelines. The first language in Uganda is English and Luganda is the main spoken language in Kampala city and its surroundings. Translation of Stroke Impact Scale 3.0 Uganda (both in English and Luganda) was then tested psychometrically by applying a Rasch model on data collected from 95 participants with stroke.
Results:
Overall, 10 of 59 (17%) items in the eight domains of the Stroke Impact Scale 3.0 were culturally adapted. The majority were 6 of 10 items in the domain Activities of Daily Living, 2 of 9 items in the domain Mobility, and 2 of 5 items in the domain Hand function. Only in two domains, all items demonstrated acceptable goodness of fit to the Rasch model. There were also more than 5% person misfits in the domains Participation and Emotion, while the Communication, Mobility, and Hand function domains had the lowest proportions of person misfits. The reliability coefficient was equal or larger than 0.90 in all domains except the Emotion domain, which was below the set criterion of 0.80 (0.75).
Conclusion:
The cultural adaptation and translation of Stroke Impact Scale 3.0 Uganda provides initial evidence of validity of the Stroke Impact Scale 3.0 when used in this context. The results provide support for several aspects of validity and precision but also point out issues for further adaptation and improvement of the Stroke Impact Scale.
Introduction
Stroke is a noncommunicable disease that accounts for majority cause of long-term disability in adult and older people. 1 However, reliable data on stroke incidence and outcomes are sparsely described in Sub-Saharan Africa.2–4 Estimation from the Global Burden of Disease has indicated that over 80% of all stroke deaths occur in low- and middle-income regions of the world.4–7 The increase in stroke has been due to the rise in many modifiable vascular disease risk factors such as physical inactivity, smoking, harmful use of alcohol, and unhealthy diets.2,3
In Uganda’s Mulago National Referral Hospital in Kampala, a considerable number of patients with stroke receive their initial care in the neurology department, but how they live their lives with disabilities after discharge from the hospital is still unexplored. Uganda faces rehabilitation challenges due to inadequate number of professionals, poor infrastructure, and limited resources to adequately reduce the burden of stroke. To the best of our knowledge, there is no published data on patient-reported outcome measures of people with stroke in Uganda. Thus, there is lack of knowledge about the rehabilitation needs of persons with stroke or the caregiver burden. However, in order to explore, evaluate, and improve the situation for people with stroke in Uganda, a valid measure for the context is required.
The first language in Uganda is English, but in order to involve the non-English-speaking stroke population, it is also necessary to have valid measurements translated into the most widespread tribal language in Uganda, which is called Luganda. Presently, there is lack of culturally adapted, psychometrically tested patient-reported outcome measures for Uganda and other Sub-Saharan African countries. Even if there is no consensus on the exact processes to translate and adapt an instrument for use in an another cultural setting, there is agreement that it is incorrect to just solely translate the instrument for direct use. 8
The Stroke Impact Scale (SIS) is a comprehensive patient-reported outcome measure that incorporates meaningful dimensions of functioning and health-related quality of life into one self-report questionnaire. 9 The SIS measures the perceived impact of stroke and includes 59 items in eight different domains: Strength, Hand function, Activities of daily living (ADL)/Instrumental activities of daily living (IADL), Mobility, Communication, Emotion, Memory and thinking, and Participation. Each aggregated SIS domain score ranges from 0 to 100, with a higher score corresponding to lower perceived impact of stroke. The SIS has demonstrated evidence of validity and reliability, 10 has fewer ceiling and floor effects, is sensitive to change, and captures major dimensions of the health-related quality of life of persons with stroke compared to the commonly used measures such as the Barthel index and the Short Form-36. 9 Although SIS 2.0 has been translated into 14 cross-cultural and valid language versions, 11 just one study of SIS 3.0 has been found that investigated its use and validity in Sub-Saharan Africa specifically from Nigeria. 12 An evaluation of SIS 3.0 that has been culturally adapted to the Ugandan context and psychometrically tested would provide an important clinical tool for gaining information regarding people with stroke perceived impact of stroke in Uganda and Sub-Saharan Africa. The aims of this study were to culturally adapt the SIS 3.0, translate the SIS 3.0 Uganda version into Luganda, and determine the psychometric properties for each domain scale of the culturally adapted SIS 3.0 Uganda (in English and Luganda) on a small scale.
Specific research questions
What changes may be needed to culturally adapt items in the original SIS 3.0 to be used in the Ugandan context?
What are the rating scale properties in the SIS 3.0 Uganda version?
Do the item responses demonstrate evidence of internal scale validity and unidimensionality of the SIS 3.0 Uganda version?
Do the participants’ responses demonstrate evidence of person response validity in the SIS 3.0 Uganda version?
Do the items in the SIS 3.0 Uganda version demonstrate stability in relation to sociodemographic factors (differential item functioning (DIF))?
Do the items in the SIS 3.0 Uganda version in a reliable way separate participants into different levels of impact of stroke?
Methods
This study was a cross-cultural adaptation and validation of the SIS 3.0 to the Ugandan context after permission from the Mapi Research Trust. To meet the aims of the study, three logical phases were performed, each including several different steps. Phase 1 was the process of cultural adaptation of the original SIS 3.0 to the SIS 3.0 Uganda version (in English). In phase 2, the translation of the culturally adapted SIS 3.0 Uganda from English to Luganda was performed. Thereafter, the psychometric properties of the new SIS 3.0 instrument needed to be assessed. Thus, in phase 3, a psychometric evaluation was performed involving the SIS 3.0 Uganda (both in English and Luganda) using a Rasch model.13,14 The study was approved by the Uganda National Council for Science and Technology (UNCST) with the approval number of HS 703 and Mulago Hospital Research and Ethics Committee.
Study participants
In phase 1
In order to achieve cross-cultural equivalence, 25 participants in three different expert committees were involved, representing a variety of people who were likely to use the instrument. 15 A total of 15 occupational therapy students, 4 teachers from the Occupational Therapy School, at Institute of Allied Health and Management Sciences (UIAHMS)–Mulago in Uganda, and 6 senior occupational therapists (OTs) working at Mulago National Referral Hospital were involved. Among the 15 students, 3 were females, 12 were males, and their ages ranged from 22 to 24 years. The four OT teachers were all males with ages ranging from 39 to 43 years. Of the six senior OTs, one was female and five were males, with ages ranging from 35 to 42 years. All senior OTs had experience of working with patients with disabilities in both hospitals and community settings.
In phase 2
The translation process was performed by two authorized translators at Makerere University, Institute of Languages from English into Luganda, one had a background in medicine and the other with no medical background. Thereafter, two additional translators translated the SIS 3.0 in Luganda back to English. A review of the translation was completed by 19 Luganda-speaking OTs attending the first Uganda Association of Occupational Therapy (UAOT) National Conference. As the final step in this phase, five persons with stroke tested the instrument.
In phase 3
The psychometric testing of the culturally adapted SIS 3.0 Uganda (in English and Luganda) was performed in a cross-sectional study with 95 persons with stroke in Kampala city and its surroundings. We aimed to include 100 participants, as that sample size generates relatively stable item difficulty calibrations. 16 Eligible criteria for inclusion were people diagnosed with stroke attending rehabilitation services at various rehabilitation units in Kampala or receiving rehabilitation at home. Stroke was defined as “a focal neurologic deficit of sudden onset that lasted at least 24 hours, with no known alternative to a vascular cause.” 17 The diagnosis of stroke was confirmed either by radiologic findings on brain computerized tomography (CT) or by clinical examination. The Scandinavian Stroke Scale (SSS) was used to describe the severity of stroke in three categories: mild (45–58), moderate (30–44), and severe (0–29).18,19 The exclusion criteria were (1) presence of psychiatric diagnosis and symptoms identifiable in the medical notes, (2) inability to understand instructions in English or Luganda, (3) living outside Kampala and surrounding areas, and (4) >75 years of age.
Procedure
Phase 1
The first step in this phase was to explore if there were some relationships between the instrument and the underlying concepts in the original version of SIS and the target setting in Uganda. 20 This cultural adaptation process of the SIS 3.0 (in English) involved three expert committees who critically analyzed each domain in the instrument, item by item. Through the committees, the authors sought to capture the experiences of daily life (experiential equivalence). 15 J.T.K. and S.G. facilitated the committees’ item-by-item analyses by looking at the conceptual meaning, experiential equivalence, and semantic (do the words mean the same thing?) and idiomatic (word that are difficult to translate might need an item with a similar meaning) connotations. 15 The discussion in each committee was written down, and field notes were made by the researchers. A conceptual equivalence was sought in cases where a word was considered to have a different conceptual meaning in different cultures.
Phase 2
The adaptation and translation of the SIS 3.0 followed a forward–backward translation procedure.14,15 After translation of SIS 3.0 Uganda into Luganda, J.T.K. distributed the instrument to the 19 Luganda-speaking OTs where they critically reviewed the instrument in order to make comments on spelling and comprehension. J.T.K. facilitated the review, and comments were collected through field notes. J.T.K. interviewed five persons with stroke to evaluate whether the items had similar meaning for each person and whether the items were difficult, confusing, or unclear to understand.8,21 J.T.K. took field notes of the interviews and discussed the findings with S.G.
Phase 3
The culturally adapted SIS 3.0 Uganda (in English and Luganda) was administered during face-to-face interviews with persons with stroke by J.T.K. and three trained research assistants in two intervals of data collection between March 2011–December 2011 and August 2014–March 2015. Data were collected at four sites: Mulago National Referral Hospital neurology ward, Mulago Hospital physiotherapy department, Stroke Rehabilitation Centre in Kampala, and homes of people with stroke. J.T.K. made the appointment with the rehabilitation professionals using Facebook, email, or mobile phone. All persons with stroke who were approached agreed to participate in the study by signing the consent form themselves and, those who were not able, authorized the caregivers to sign on their behalf. However, most of the participants identified during their stay at the acute ward and had agreed to participate in the study could not be reached after 3 months since some of them had died and others went back to far home districts.
Data analysis
Phase 1
A descriptive summary of notes generated from each expert committee discussion about the original SIS 3.0 was analyzed by J.T.K. and S.G. Consistent and important comments, regarding conceptual, experiential, semantic, and idiomatic equivalence that appeared in at least two groups, were adopted in the SIS 3.0 Uganda.
Phase 2
The report produced by the translators was discussed by J.T.K., and S.G. Notes from both translators and the Luganda-speaking OTs were analyzed by J.T.K. The important components of the notes included, semantic, experiential, idiomatic, and grammatical use of words14,15 plus correction of spelling errors in the Luganda-translated SIS 3.0. The findings from the five persons with stroke who had tested the SIS 3.0 Uganda in Luganda were discussed by J.T.K. and S.G. in order to ensure the cultural relevance by making sure that the expressions were clear to the respondents and the researchers.
J.T.K. produced a report about the process of instrument adaptation and translation, and both the reports and the translated instrument were submitted to the original instrument developers Mapi Research Trust for approval. The Mapi Research Trust User Agreement (#15LI017M) was signed (26 March 2012).
Phase 3
Descriptive statistics were used to depict the study sample concerning stroke severity, age, and gender. A Rasch model was chosen to evaluate the psychometric characteristics of the adapted and translated SIS 3.0 Uganda by domain using the WINSTEPS software program (version 3.69.1.16). 22 Rasch models are currently preferred in the development and validation of clinical measurement scales in rehabilitation. 13 The Rasch analysis converts the raw item scores from a test or questionnaire into equal interval measures. Furthermore, the outputs from a Rasch analysis can be used to examine whether items from a scale measure a unidimensional construct, which is viewed as crucial in measurement statistics. 23 In this study, we followed an earlier described analytical process model, which has been described in more detail elsewhere.24,25 Initially, in order for the assessment to meet the essential criteria for a measurement scale, the average measures by each category must advance monotonically for each set of observations 26 and the outfit mean square (MnSq) values for each step category should also be less than 2.0. 26
Internal scale validity and person response validity in the dataset were then investigated using the item and person goodness-of-fit statistics and infit MnSq values >1.4 logits associated with standardized z ⩾ 2.0 values 27 as criteria for not demonstrating acceptable goodness of fit. It is generally acceptable if 5% of the items and persons by chance do not demonstrate acceptable goodness of fit. 28
The scale validity was further evaluated using a principal component analysis (PCA) of the residuals. 29 The criteria for variance explained in each of the domains were set to 60%.
Stability of the item response patterns in relation to SIS 3.0 Uganda language version, age, gender, level of education, civil status, side of the affected body, and previous work status (e.g. if an item is relatively similar in challenge for male and female participants) were also evaluated. As items that are functioning differently (being more/less challenging) for certain subgroups can be a threat to validity, a series of differential item function (DIF) analyses were performed using Mantel–Haenszel for polytomous measure in the WINSTEPS program at a level of significance (p < 0.01). 29
Finally, the separation indices are estimates to evaluate whether a test in a reliable manner generates precise individual measures that can be differentiated from one another. 30 A criterion for the person-separation reliability index was set to being equal to or greater than 1.5. The domain could then clinically separate the sample into at least two different strata (higher and lower levels of perceived impact of stroke). 30 The WINSTEPS program also computes an equivalent measure of Cronbach’s alpha, which indicates the reliability of the scale. We set a criterion that the reliability coefficient should exceed 0.80.
Results
Cultural adaptation of the SIS 3.0
The various expert committees, comprising people with different levels of professional experience, were organized separately, but they all pointed out similar items that required adaptation, and this strengthened the content validity and reliability of the adapted instrument.
The domains of Strength, Memory and thinking, Emotion, and Communication all had word expressions that were conceptually, semantically, idiomatically, and experientially relevant in the Ugandan context. However, some items in the SIS domains of Participation, Mobility, Hand function, and ADL/IADL had to be altered in order to have relevant meanings in the Ugandan context. Items in the ADL/IADL domain were altered, “clip your toe nails” to “cut your toe nails.” The item “cut your food with a knife and fork” was altered to “feed yourself with a hand fork/spoon.” In the item “get to the toilet on time,” the word latrine was added because some people use latrines. The item “Go shopping” was altered to “buy items from the shop” because people go to small shops to buy one specific item at a time in a day. The examples given for “heavy household chores” were changed from vacuum cleaning, laundry, and yard work to sweeping, washing, and cleaning the compound. In Uganda, a negligible number of people use vacuum cleaners and washing machines, and people refer to a yard as a compound. In the domain Mobility, the item “walk a block” was changed to “walk 100 meters” because there are no standard blocks in Uganda. “Climb one flight of stairs” was changed to “climb a staircase once.” In the domain Hand function, an example of carrying heavy objects such as “bag of groceries” was altered to a “5 litre Jerry can of water” because people commonly carry water containers in their daily activities. The item “turn door knob“ was altered to “turn door handle“ and the item “pick up a dime” was changed to “pick up a coin.” The statement “door handle” and the word “coin” are just semantics commonly used in daily life. Overall, 10 of 59 (17%) items in the eight domains needed to be culturally adapted in the original SIS 3.0 to be used in the Ugandan context. The majority were 6 of 10 items in the domain ADL/IADL, 2 of 9 items in the domain Mobility, and 2 of 5 items in the domain Hand function.
The translation process
The translators indicated that not all words in English had directly translatable equivalent words in Luganda, and occasionally, expressions in English were used to translate to Luganda. Such words/terms as emotion, feeling nervous, and concentration did not have translatable equivalences. Instead, expressions in Luganda were used as a substitute for one specific word. The report of the 19 OTs attending the UAOT conference indicated that the translation was done properly and they had nothing to add, substitute, or remove. The data collected from the five persons with stroke who tested the SIS 3.0 Uganda in Luganda found that the instrument was culturally relevant to them, and no additional modification of the instrument was needed to fit the target sample.
Psychometric evaluation
A total of 95 participants completed the SIS questionnaire (in English, n = 41, and in Luganda, n = 54), and the data were subsequently included in the Rasch analysis. Table 1 summarizes the baseline characteristics of the sample including gender, level of education, marital status, side of the body affected, and work status. The mean age of the persons with stroke was 52 years, and the majority of them (75%) had had an ischemic type of stroke, and 41% had moderate stroke according to SSS. Table 2 shows the aggregated domain scores of the SIS 3.0 for the sample. Table 3 summarizes the results of the rating scale properties, item and person validity, PCA, DIF and reliability, and person separation.
Demographics of the participants from Uganda with stroke (n = 95).

SSS: Scandinavian Stroke Scale; SD: standard deviation.
The SIS 3.0, aggregated domain scores and self-rated recovery.
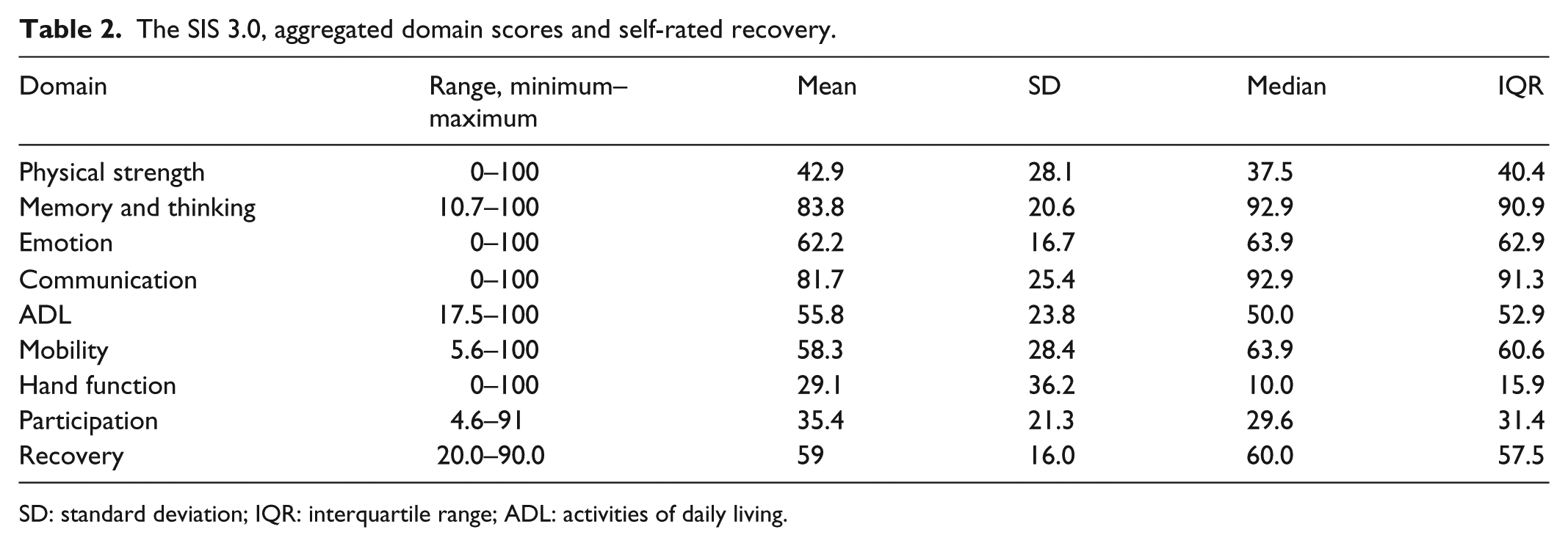
SD: standard deviation; IQR: interquartile range; ADL: activities of daily living.
Psychometric properties of the domains of Uganda SIS 3.0 version among persons with stroke (n = 95).

ADL: activities of daily living; SIS: Stroke Impact Scale.
Category 3 higher than expected outfit: 2.70.
SIS3h and SIS3i demonstrated misfit.
SIS4g demonstrated misfit.
SIS5a and SIS5f demonstrated misfit.
SIS6a demonstrated misfit.
SIS7a demonstrated misfit.
SIS8a demonstrated misfit.
Mantel–Haenszel statistics p < 0.01, measure used to determine DIF.
Item SIS5b demonstrates DIF by body side affected: left hemisphere: 44.25, right hemisphere: 51.39.
Item SIS8b demonstrates DIF by marriage variable: single: 51.18, married: 47.11.
Rating scale properties
The average measures of the SIS 3.0 Uganda version demonstrated monotonicity advancement up the rating scale, and only one of the scale categories demonstrated outfit MnSq values exceeding 2.0.
Internal scale validity and unidimensionality
Only in the domains of Strength and Memory and thinking, all items demonstrated acceptable goodness of fit. The remaining six domains had at least one item that did not show acceptable goodness-of-fit statistics. So, the range of item misfit was from 77.8% to 100% across domains. In total, 8 items out of all 59 items (13.6%) in the SIS 3.0 demonstrated misfit to the Rasch model. After deletion of the misfitting items from the domains, the results of PCA were acceptable for the domains Strength, Memory and thinking, Communication, Participation, Mobility, Hand function, and ADL/IADL, further supporting unidimensionality within these domains. However, for the domain Emotion, only 51.5% of the total variance within the sample was explained by the first dimension; thus, the unidimensionality of this domain was questionable.
Person response validity
There were more than 5% person misfit in the domain Participation and Emotion while Communication, Mobility, and Hand function domain had the lowest proportions of person misfits.
DIF
There were no items demonstrating DIF between SIS Uganda version using the English or Luganda languages across the domains. There were also no significant uniform DIF in six of eight domains in relation to the six person demographic factors: age, gender, level of education, civil status, side of the affected body, and previous work status. The domains that demonstrated significant DIF were the ADL/IADL domain where one item “dress the top part of your body” demonstrated a significant uniform DIF in relation to the body side affected, and another item “limited in social activities” in the domain Participation demonstrated uniform DIF with marital status.
Separation and reliability
The person-separation index in the SIS 3.0 Uganda five domains of Strength, ADL/IADL, Mobility, Hand function, and Participation were all above 1.5 indicating that they could separate the sample into two or more groups. The domain Emotion had the lowest person-separation index of 1.43; therefore, it was not able to separate the sample into more than one group, thus indicating that it is not functioning as a measurement scale in this sample. The reliability coefficient was equal or larger than 0.90 in all domains except the Emotion domain, which was below the set criterion of 0.80 (0.75).
Table 4 provides the details of the individual item difficulty calibrations (ranged from easier to more challenging items) in Strength (1a–d), Memory and thinking (2a–g), Emotion (3a–i), Communication (4a–g), ADL/IADL (5a–j), Mobility (6a–j), Hand function (7a–e), and Participation (8a–h). The item difficulty calibrations, item standard error (SE), infit MnSq, and Z statistics per SIS domain are presented from the Ugandan sample with stroke (n = 95).
Item difficulty calibrations, item standard error (SE), and infit MnSq statistics per SIS domain from the Ugandan sample with stroke (n = 95).
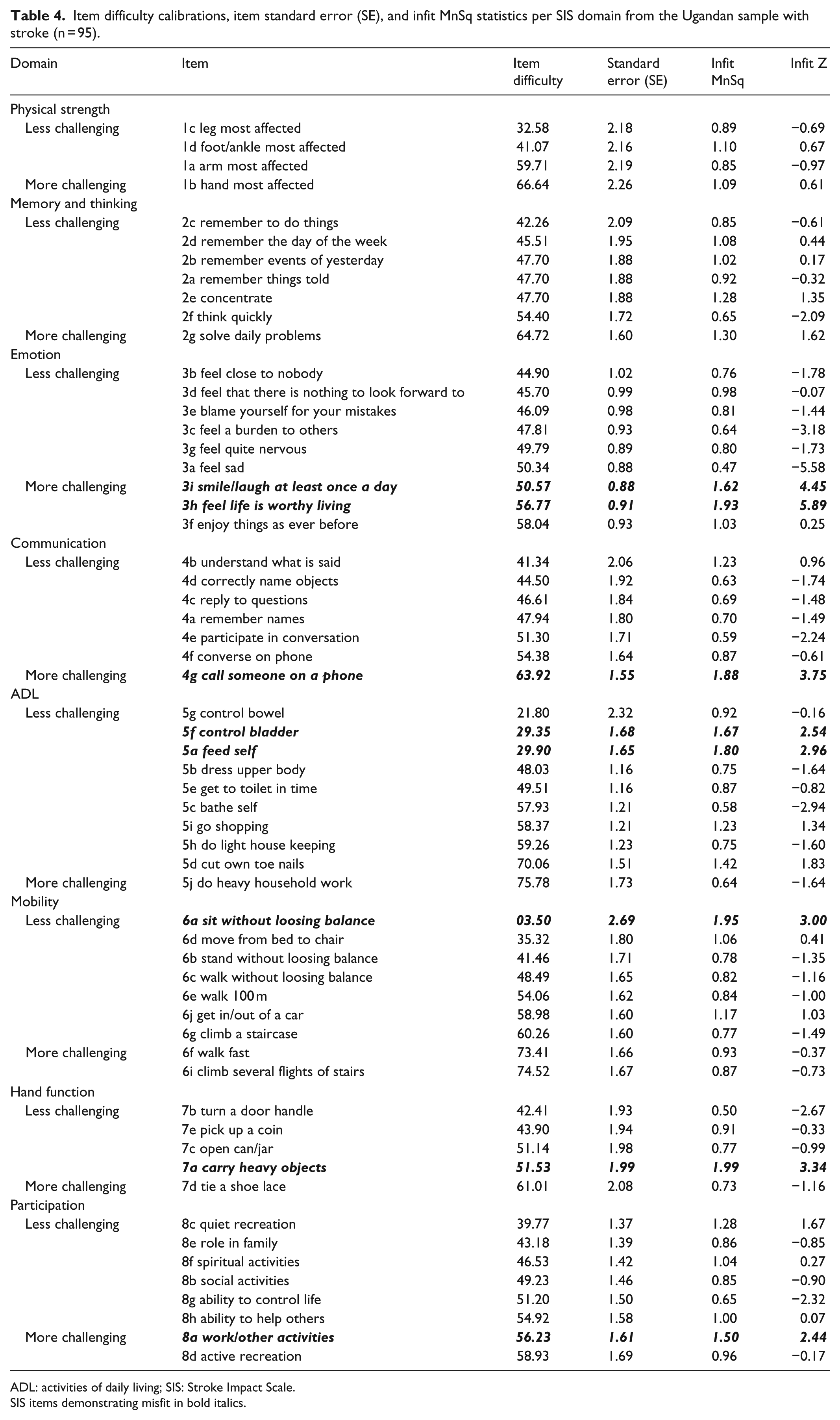
ADL: activities of daily living; SIS: Stroke Impact Scale.
SIS items demonstrating misfit in bold italics.
Discussion
This study is the first to present a culturally adapted, translated, and psychometrically tested version of the SIS 3.0 for use in Uganda. Context relevant adaptations to some SIS items were incorporated in the SIS 3.0 Uganda versions, and translation that aimed at conceptual, experiential, semantic, and idiomatic equivalence seemed to have been achieved. The results provide support for several aspects of validity and precision but also point out issues for further adaptation and improvement of the SIS. The study may also provide important information about various consequences of stroke for the Ugandan population, as described in Tables 2 and 4.
Taken together, the study indicates that the SIS 3.0 Uganda is overall a suitable instrument to evaluate the impact of stroke in an urban and semi-urban stroke population in Uganda, given that actions are undertaken to minimize the impact of the items demonstrating misfit and DIF. Furthermore, the Emotion domain aggregated measures should be treated with caution, as they may not be precise enough to detect differences in subgroups. The largest impacts of stroke in this sample were found in the domains Hand function and Participation, whereas the domains Memory and Communication were least impacted (shown in Table 2). This probably meant that participants in this sample perceived more physical impairments as compared to cognitive and language impairments.
The cultural adaptation
When culturally adapting the SIS 3.0, the domains ADL/IADL and Mobility were more sensitive to the culture than the domains that are more related to the bodily functions, and this is termed as experiential equivalence. Items in these two domains seek to capture the experience of daily life; however, in Uganda the given tasks simply might not be experienced, even if they were translated in the same way as in the original version of SIS 3.0. The items in the questionnaire were replaced by similar words describing the same items that are actually experienced in the target culture. 15 One explanation for why the item “feed yourself with a hand or fork/spoon” demonstrated a misfit could probably be that some people who were using cutlery for eating before their stroke found it difficult to use cutlery after the stroke, and those who used their hand to eat still found it easy to use after the stroke. It is notable that it was the same culturally adapted items that showed misfit in both the Uganda and Luganda versions of the SIS 3.0. This may raise a question about the adaptation process of the instrument, which may require further investigation. However, the adapted items were more contextually biased and that could reflect unexpected responses, hence item misfit. It is important to recognize variations in everyday performances of the activities within a culture as well as between cultures. These variations also need to be taken into consideration when adapting an outcome measure such as SIS 3.0 for a new context. Attention to this level of detail seems to allow increased confidence that the impact of a condition such as stroke is described in a similar manner in trials or outcome evaluations. Therefore, the findings of this study raise an important question about the validity of adapted items, and a future study may be required to find out whether the adapted items affected the validity of the instrument.
The translation process
The translation process involved professional translators who were not familiar with the research topic. The translation process was performed by two authorized translators from English into Luganda, and thereafter, two additional translators translated the SIS 3.0 in Luganda back to English. Thus, the translation was not likely to be affected by translators’ bias but might have been affected by semantic misinterpretation. However, such misinterpretations were discovered and corrected by the advisory committees. Furthermore, there were many phases and processes that included different groups of people with different backgrounds and that improved both the cultural adaptation and translation processes. The latter process was aimed at maintaining the relevance and meaning of items in all domains of the instrument. The instrument was checked to ascertain that words had similar meanings. Words or expressions that had no direct translation were discussed and equivalent expressions in the Luganda language were found and equivalent contextual expressions were included.
The psychometric evaluation
In the last phase of evaluating the instrument, the overall validation of the SIS 3.0 Uganda adhered to the Rasch model assumptions. The findings showed high values of scale fit for all domains of SIS 3.0 Uganda in agreement with the previous study conducted in Brazil and Germany.15,31 When deleting these misfitting items, the remaining items worked well together to form a unidimensional scale. Of the three reversed items in the Emotion domain, two did not demonstrate acceptable goodness of fit. Other items that misfitted were one item in the domain Communication, two items in ADL/IADL domain, one item in the Mobility domain, one item in Hand function domain, and one item in the Participation domain. In the Brazilian SIS 3.0 version, 31 four items including the two mentioned above in the Emotion domain also demonstrated misfit to the Rasch model and the related item on incontinence in the ADL domain. In line with these findings, additional Rasch studies using the Functional Independence Measure (FIM) has also shown that continence does not match the underlying construct. 32 In addition, reversed items demonstrated problems with item fit in empirical studies with other diagnostic tools. 33
The results do, however, indicate evidence of fairness in testing in the SIS 3.0 Uganda within this Ugandan sample, as the domains did not demonstrate item DIF in relation to English or Luganda. The uniform DIF between the item “dress the top part of the body” and the body side affected could probably be due to the paralysis which systematically could impact the scores on this item. In the domain Participation, uniform DIF was also found in the item “limited in social activities” and whether one was single or married, which is also logical in relation to the direction of DIF (see Table 3). In summary, based on these findings, further larger clinical studies using SIS 3.0 Uganda in the Ugandan context need to be cautious in summarizing scale scores including items demonstrating misfit and DIF, as they may compromise the validity of the individual measures. On the basis of how SIS 3.0 is currently reported (using percentage on an aggregated 100-level scale), such comparable measures could still be calculated and reported from the Ugandan context without compromising the validity of such measures. It is also crucial to highlight that the items in SIS demonstrating misfit or DIF may still be highly clinically relevant and should, therefore, still be included in the SIS evaluation but should be treated with caution when generating the aggregated scores, as they may compromise the validity of such scores.
In this study, the domain Emotion lacked acceptable ability to separate the sample into at least two distinct strata. These findings are in line with other studies conducted in more western societies which have indicated that items in the Emotion domain were less sensitive to change and were associated with random variability across time.11,25 Based on the findings, we would argue that the domain Emotion also should be used with caution in intervention studies in Uganda, as it does not demonstrate unidimensionality nor is it sensitive enough to distinguish specific groups.
Recruiting participants into the project became a long process and took a long time. It would have been easier if there were organized stroke rehabilitation services in Uganda. This also affected the number of included participants; however, as this is a small-scale study, a sample size of approximately n = 100 has been suggested to provide relatively stable pattern of responses and detection of misfitting items. 34 The study findings can, therefore, still be viewed as providing pilot validity evidence of SIS 3.0 Uganda in this context. Larger and more representative samples are desirable for any type of definitive statistical analyses and thus would be preferable to draw definite conclusions regarding the validity of the SIS 3.0 Uganda among the population with stroke in Uganda. Although this study used a smaller sample that was not population based, it was drawn from multi-cultural Kampala, the capital city of Uganda and thus should reflect to a greater extent the urban population’s characteristics. However, more investigations may be required to explore the psychometric properties of SIS 3.0 Uganda using more rural samples of the stroke population, and thus, future studies with larger and more heterogeneous samples are required in order to verify or refute those hypotheses. It is also important to compare item hierarchies of the domains in SIS 3.0 across contexts and cultures, in order to make valid comparisons between international samples with stroke.
In conclusion, the cultural adaptation of SIS 3.0, the translation, and the subsequent validation were overall successful. Most domains of the SIS 3.0 Uganda version satisfy essential criteria for rating scale functioning and have satisfactory internal consistency and discrimination validity among people with stroke in Uganda. Future studies with larger samples are, however, required for more in-depth analysis of item and person fit. Such studies should also focus on comparisons of measures across contexts in order to understand more generic consequences of stroke in a global context.
Footnotes
Acknowledgements
We thank the participants with stroke and their family members for participating in this study. We would like to extend our sincere gratitude to the participants for their active participation and Professor Elly Katabira for his contribution to the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Uganda National Council for Science and Technology (UNCST) HS 703.
Funding
The financial support for this study was provided by the Swedish Research Council, Developmental Research (grant number 2014-28-63), the Swedish Association of Occupational Therapists, the HELD research group at Karolinska Institutet (![]() ). The authors alone are responsible for the content and writing of this article.
). The authors alone are responsible for the content and writing of this article.
Informed consent
Written informed consent was obtained from all participants before the study.