
Abstract
Alkaptonuria is a rare autosomal-recessive metabolic disorder of tyrosine degradation which results in elevated levels of circulating homogentisic acid. Ochronosis occurs when homogentisic acid polymerizes and deposits in connective tissue. Ochronotic lesions in the carotid arteries have not been described. In this report, we describe a 65-year-old man with alkaptonuria, with hypertension and hyperlipidemia, who underwent an uneventful carotid endarterectomy for an asymptomatic high-grade internal carotid artery stenosis. Histology revealed homogentisic acid deposits as black-brownish areas in the intima. He was noted to have an impressive heavily brown-black pigmented discoloration of the carotid plaque. Cardiovascular involvement is a rare consequence of alkaptonuria and is manifested by pigment deposition at the areas influenced by shear stress and turbulence.
Introduction
Alkaptonuria is a rare autosomal-recessive metabolic disorder of tyrosine degradation which results in elevated levels of circulating homogentisic acid (HGA). Increased circulating HGA is the root cause of the triad associated with the condition: homogentisic aciduria, arthritis, and ochronosis. Ochronosis occurs when HGA polymerizes and deposits in connective tissue throughout the body. Ochronotic deposits are commonly reported in the skin, sclera, cartilage, joint spaces, and tendon sheaths. Other manifestations include stone formation, tendon rupture, pathologic fractures, and severe arthropathies. Cardiovascular manifestations have previously been localized to valves, coronary arteries, and the aorta. Ochronotic lesions in the carotid arteries have not been described. In this report, we describe a 65-year-old man with alkaptonuria, with no other major cardiovascular risk factors, who underwent an uneventful carotid endarterectomy for an asymptomatic high-grade internal carotid artery stenosis.
Case description
The patient was a 65-year-old man with a history of alkaptonuria, hypertension, hyperlipidemia, staghorn calculi, and bilateral knee and shoulder replacements. He has had lithotripsy several times for his symptomatic kidney stones. He also has had spine surgeries in the past and he still suffers from significant back pain at times. He has had no history of transient ischemic attack, stroke, or amaurosis fugax. He has never smoked. His review of system and physical examination did not reveal any significant finding. He was undergoing surveillance for valvular disease by his cardiologist who detected a carotid bruit on physical examination. After carotid duplex showed high-grade (more than 80%) stenosis of right internal carotid artery (Figure 1), the patient was referred to vascular surgery for carotid endarterectomy. The patient underwent uneventful standard carotid endarterectomy with bovine pericardial patch angioplasty under general anesthesia with cerebral oximetry as neurologic monitoring. A shunt was not used.

Ochronotic deposits within the carotid plaque and intima.
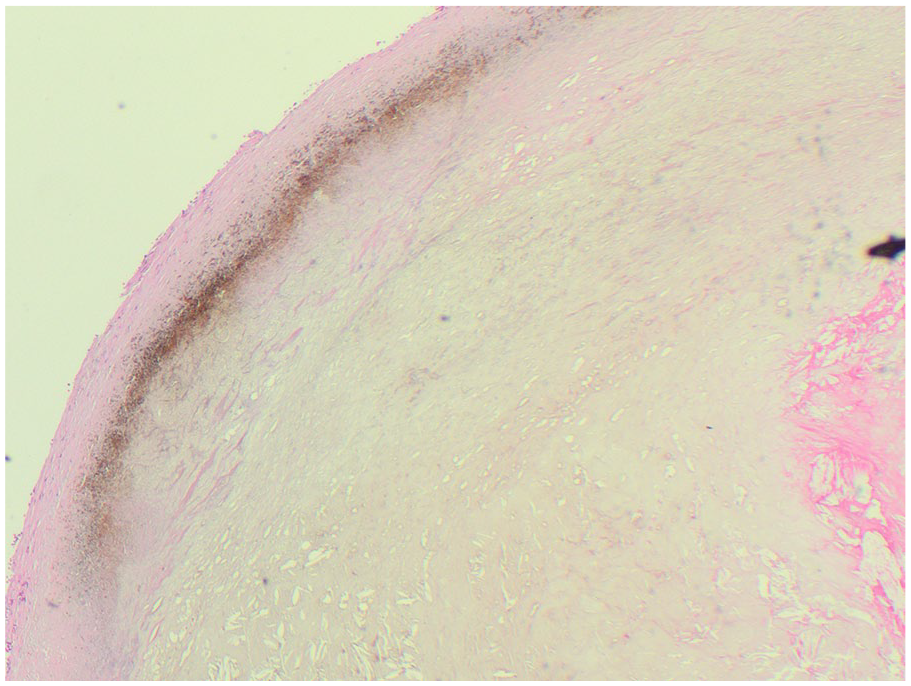
Upon dissection into the carotid sheath, a black-pigmented carotid artery was identified. Entry into the carotid revealed plaque with multiple dense black deposits. He was noted to have an impressive heavily brown-black pigmented discoloration of the carotid plaque as depicted in Figure 2. Histology revealed HGA deposits as black-brownish areas in the intima (Figure 3). He was discharged on the first postoperative day on 81 mg aspirin and a statin medication. He has been seen in follow-up a year later and he is in his usual state of health.

H&E stain of carotid plaque—showing ochronotic (brownish) deposit near the intimal wall with stripped layers of tunica media to the far left. Atherosclerotic cholesterol plaque is depicted to the right of the ochronotic deposits. A dense cholesterol-rich core is in the center with right-sided pink-appearing thrombus.
Preoperative ultrasound imaging. Left panel shows internal carotid artery high-grade stenosis with significant luminal stenosis. Right panel shows velocities in proximal internal carotid artery.
Discussion
Alkaptonuria is a rare autosomal-recessive deficiency of HGA dioxygenase, an enzyme required for the degradation of tyrosine. This leads to elevated circulating levels of the substrate, HGA. When HGA is excreted, it darkens urine; when circulating it can polymerize forming a melanin-like substance and ultimately deposit in connective tissues.
The prevalence of alkaptonuria is around 1:100,000–250,000, and thus, literature regarding the condition is mostly observational. Interestingly, manifestations of the disease such as ochronosis in cartilage were described by Dr Virchow 1 as early as 1865. It is one of the earliest known metabolic diseases. It was understood to be a result of a metabolic deficiency by Garrod2,3 in 1902 and presented to the Royal College of Physicians as such in 1908. The genetic basis of the disease had not been fully understood until nearly a century later in 1996. 4 The characteristic ochronotic plaques are named after the discolored (clay-colored) tissue found on microscopic evaluation.
Alkaptonuria may be clinically relevant at birth, with affected babies having darkened diapers from homogentisic aciduria. As these patients age to the third decade of life, darkened deposits in the sclera or ear cartilage may develop. Ochronosis can cause the formation of various stones, connective tissue ruptures, pathologic fractures, valvular disease, coronary-artery disease, and aortic root disease. The most clinically impactful manifestation is arthropathy secondary to ochronotic deposits, resulting in the need for early arthroplasty. In one of the largest natural history series, life-table analyses showed that joint replacement was performed at a mean age of 55 years, renal stones at 64 years, cardiac-valve involvement at 54 years, and coronary-artery calcification at 59 years. 5
Cardiovascular involvement is a rare consequence of alkaptonuria and is manifested by pigment deposition at the areas influenced by shear stress and turbulence. Multiple studies have described the cardiovascular manifestations of alkaptonuria. In the largest reported series of patients with alkaptonuria, the most common cardiovascular manifestation of alkaptonuria was stenosis of the aortic valve. 6 In two studies identifying cardiovascular manifestations, the prevalence of aortic stenosis was 17%–25%.6,7 When compared the general population, the prevalence was higher, with general population incidence which leads previous authors to posit that turbulent flow and increased pressure lead to microvascular damage that was an ideal focus for HGA deposition. 6
In another article outlining cardiovascular ochronsis in a single patient, Vavuranakis et al. describe severe aortic stenosis and coronary disease with HGA deposits at autopsy. They posited that the patient’s peripheral vascular disease and coronary disease may have been partly due to pigment deposition in the arterial intima. However, no pathologic specimens were analyzed. 8
Unfortunately, in a previous analysis of patients with alkaptonuria, carotid imaging had not been reviewed; therefore, there is no data on the prevalence of carotid stenosis in these patients. In the future, retrospective analysis may consider evaluating concomitant carotid stenosis. Ours is the first case report identifying ochronotic plaque in the carotid artery. With such a low prevalence of alkaptonuria, it is unclear whether this was an incidentally found carotid plaque from usual etiologies or if the carotid bifurcation is a newly identified location of accelerated plaque deposition in alkaptonurics.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.