
Abstract
Background:
Incomplete or delayed access to discharge information by outpatient providers and patients contributes to discontinuity of care and poor outcomes.
Objective:
To evaluate the effect of a new electronic discharge summary tool on the timeliness of documentation and communication with outpatient providers.
Methods:
In June 2012, we implemented an electronic discharge summary tool at our 145-bed university-affiliated Veterans Affairs hospital. The tool facilitates completion of a comprehensive discharge summary note that is available for patients and outpatient medical providers at the time of hospital discharge. Discharge summary note availability, outpatient provider satisfaction, and time between the decision to discharge a patient and discharge note completion were all evaluated before and after implementation of the tool.
Results:
The percentage of discharge summary notes completed by the time of first post-discharge clinical contact improved from 43% in February 2012 to 100% in September 2012 and was maintained at 100% in 2014. A survey of 22 outpatient providers showed that 90% preferred the new summary and 86% found it comprehensive. Despite increasing required documentation, the time required to discharge a patient, from physician decision to discharge note completion, improved from 5.6 h in 2010 to 4.1 h in 2012 (p = 0.04), and to 2.8 h in 2015 (p < 0.001).
Conclusion:
The implementation of a novel discharge summary tool improved the timeliness and comprehensiveness of discharge information as needed for the delivery of appropriate, high-quality follow-up care, without adversely affecting the efficiency of the discharge process.
Introduction
Transitions of care between the hospital and outpatient setting are periods of vulnerability for patients. Incomplete or delayed access to information by patients and outpatient providers has been linked to preventable medical errors.1–3 Numerous studies demonstrate that adverse events such as medication errors and failure to follow-up pending tests may be prevented by improved inpatient–outpatient provider communication.2,4–7 The primary form of communication between these providers is the hospital discharge summary, but the availability of discharge summaries at the first post-discharge hospital visit is low, ranging from 12% to 34%. In addition, discharge summaries often lack important information such as updated discharge medications and follow-up plans.8,9
The Joint Commission has identified a standardized, written discharge summary completed within 30 days of hospital discharge as a key transition of care element to improve patient outcomes. The six primary content areas to be contained in a discharge summary, as mandated by The Joint Commission, are: reason for hospitalization, significant findings, procedures and treatment provided, patient discharge condition, patient and family instructions, and attending physician signature. 10 Other groups, including six major medical societies at the 2009 Transitions of Care Consensus Conference, 11 have proposed more detailed guidelines for discharge summary content.9,12–14 There is also developing consensus that electronically generated discharge summary notes, rather than paper notes or dictations, are more likely to be completed, are completed faster, and are preferred by inpatient and outpatient providers.15,16 Many hospitals have responded to these recommendations by monitoring discharge information sharing. For example, a 2010–2011 survey of hospitals participating in the Hospital to Home Quality Improvement Initiative found that 70.6% of hospitals track the timeliness of discharge summaries, and 72.9% track the accuracy of medication reconciliation in the discharge summary. 17 In all, 73% of hospitals also reported using an electronic form to complete medication reconciliation, and this number increased to 81% in 2012. 18
At our hospital, standard practice prior to June 2012 was to give patients a brief instruction document detailing their medication list, diagnosis, and follow-up appointments at the time of discharge. A complete discharge summary was dictated at a later date. Patients were called at home by a nurse 48 h after discharge, but a completed discharge summary was rarely available at that time, and was also rarely available at the time of outpatient follow-up appointments. To address these issues, we developed a tool for creating a combined electronic discharge note incorporating patient instructions and a comprehensive discharge summary for outpatient providers. The tool facilitates combined discharge note completion and delivery to the patient at the time of discharge and immediately becomes available to all providers in our healthcare system through the electronic medical record. The goal of this intervention was to improve communication between inpatient and outpatient providers in a manner that is transparent to the patient and puts information pertinent to medical care directly in the patient’s hands. In this study, we assess the comprehensiveness and availability of discharge information for post-discharge care, as well as the satisfaction of outpatient providers after implementation of the new tool. We also assess the effect of the tool on efficiency with respect to the discharge process.
Methods
Design, setting, and intervention
We conducted a pre–post quality improvement evaluation of the effect of a new electronic discharge summary tool on timeliness of discharge documentation and communication with outpatient providers at a 145-bed university-affiliated Department of Veterans Affairs (VA) medical center. The new tool was pilot tested by one academic inpatient medicine team between December 2011 and June 2012 prior to full deployment and use by all four of the medicine teams in July 2012. Implementation and evaluation of the new discharge summary tool was conducted as part of a quality improvement initiative and was therefore exempt from institutional review board (IRB) review.
Prior to July 2012, physicians completed a daily progress note and physician discharge instruction note on the day of discharge. A senior resident dictated or typed a formal discharge summary at a later date using a simple template in the VA computerized patient record system (CPRS). The business office then formatted the submitted document and after several days forwarded the discharge summary to the attending physician to sign. The attending could not edit the note, but could create an addendum to document any additional comments or discrepancies. Outpatient providers could then view the discharge summary in the electronic health record or by fax. This process usually took greater than a week and sometimes close to a month before the note was available for viewing by other providers.
The new electronic discharge summary tool was developed to facilitate the creation of a discharge note that could be given to patients at the time of discharge and also be immediately available to outpatient care providers. Its development was a collaborative effort between clinicians and electronic health record specialists within the VA. The tool combines free text, clinical reminders, and data objects into a template that is completed within the electronic health record. It also prompts the user to complete medication reconciliation and highlights medication changes. The new note combines the last day progress note, physician discharge instructions, and discharge summary into a single document that is given to the patient at the time of discharge. The content of the note was designed to adhere to both Joint Commission guidelines and recommendations from the Society of Hospital Medicine’s Project BOOST initiative. 19 The electronic discharge summary tool forces the completion of every item, represented by a separate text box or multiple-choice checkbox, before the note can be submitted.
Data collection and measures
Assessment of the timeliness of the discharge summary note for post-discharge care focused on the availability of the discharge summary information at the first follow-up contact with an outpatient provider. This contact included phone follow-up by a nurse (which is generally scheduled to occur within 48 h after discharge), or a visit with a primary care provider or a specialist, since complete discharge information is important to the quality of follow-up regardless of the type of contact. Data were collected through chart reviews of patients admitted roughly 5 months before implementation of the tool, 3 months after implementation of the tool, and 1.5 years after tool implementation. We randomly selected 30 patients admitted by one of the academic medicine services during the select study months and reviewed their electronic medical records to determine whether the discharge summary note was available at the time of the 48 h nurse phone call, the first post-discharge primary care provider outpatient visit, and the first post-discharge specialty provider outpatient visit. We also noted which of these contacts occurred first.
We assessed outpatient provider satisfaction with the new discharge summary note through a survey of providers conducted in October 2012, 3 months after the new combined discharge note was fully implemented. An eight-question written survey was placed in the mailboxes of 50 primary care providers at the VA medical center. The providers included physicians (attendings and residents), registered nurse care managers, and pharmacists. The questions used a 5-point scale to assess preferences between the old and new discharge summary, details of the discharge summary note, and timeliness of summary note completion. The survey also included an open-ended question that requested feedback on how the new discharge summary could be improved.
We evaluated the potential effect of the tool on the efficiency of the hospital discharge process by examining the time between the decision to discharge a patient and posting of either the patient discharge instructions note (pre-implementation of our tool) or the combined discharge summary note (post-implementation) in the electronic chart. In our workflow, posting one of these notes indicates that the physician has completed all of the work required for a patient to leave the hospital. Efficiency data were collected 2 years prior to tool implementation, 3 months after implementation, and again 2.5 years after tool implementation. These data were collected through observation and review of electronic medical records. An observer would follow the medical teams and record the time the physician determined that a patient would be discharged that day. This decision was usually made during morning rounds. This time was then compared to the time the patient discharge instructions note (pre-implementation) or combined discharge note (post-implementation) was entered and signed in CPRS. This information was collected, in part, to determine whether the increased requirements for documentation at the time of patient discharge might slow down the discharge process.
Data analysis
Our data analysis is primarily descriptive. We compare the time for completing the discharge note and availability of the summary note information for post-discharge care at various time points before and after implementation of the new discharge summary note tool. If a patient’s discharge was delayed due to external circumstances (e.g. a nursing home bed was not available for transfer), the data for time to discharge note completion is removed as an outlier. Student’s T-tests are used to determine if there are differences in the time to note completion between time points. Outpatient provider use of and satisfaction with the new discharge summary information is determined by the responses to specific survey questions, noting in particular the percentage who responded positively to the different items.
Results
Comprehensiveness of discharge summaries
Table 1 summarizes the content areas of the notes that were available in the electronic chart at the time of patient discharge, before and after implementation of the discharge summary note tool. Prior to June 2012, the only note that appeared in the electronic chart at the time of discharge was the patient discharge instructions note, which contained a limited set of information pertinent to patients and their caregivers. After June 2012, the combined discharge summary note appeared in the electronic chart at the time of discharge and contained more comprehensive information pertinent to both patients and physicians. The completion rate of required content was 100% in the new process.
Comparison of the content of the electronic notes available at the time of discharge (pre-June 2012 patient discharge instructions note vs post-June 2012 combined discharge summary note).
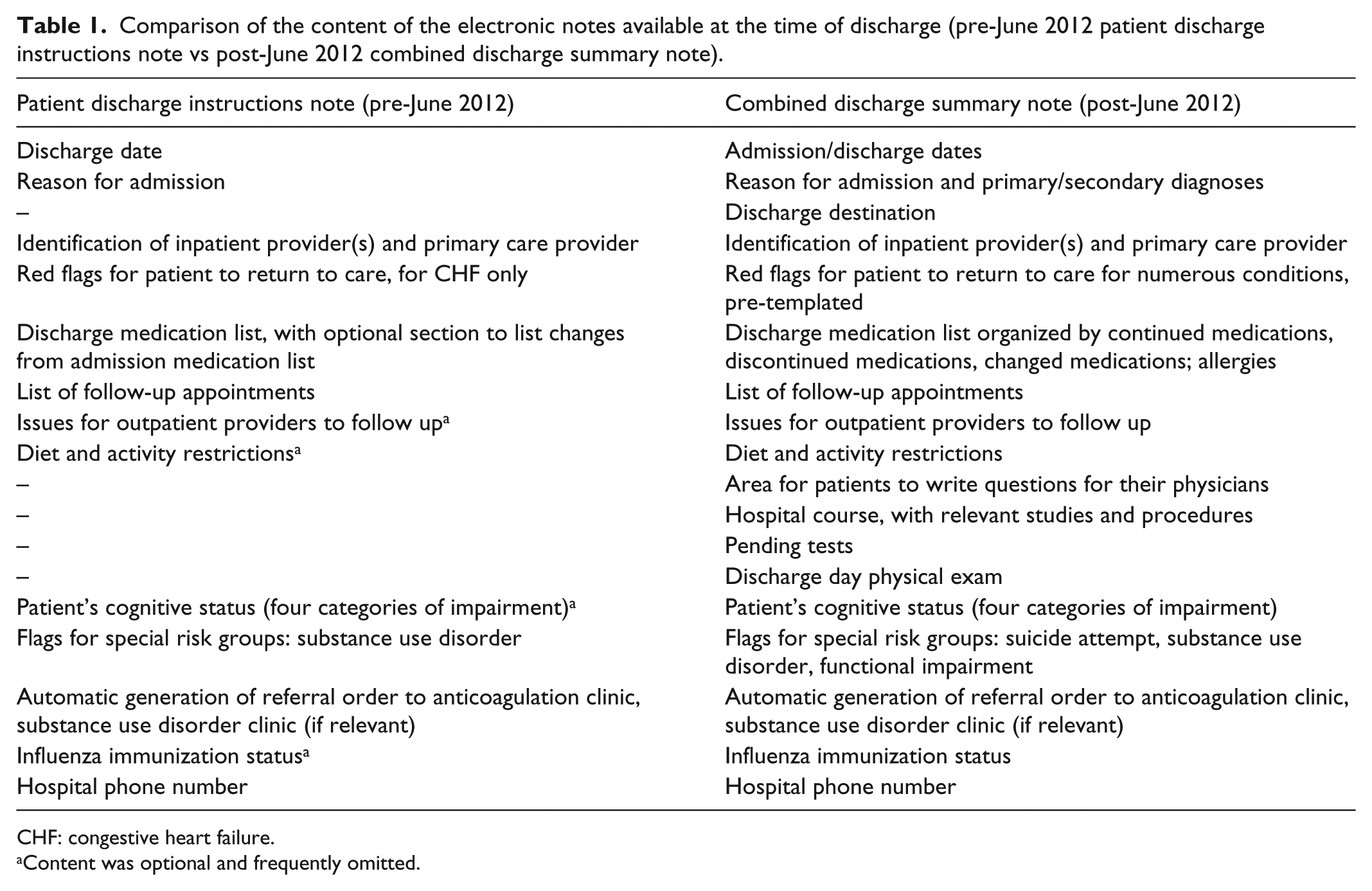
CHF: congestive heart failure.
Content was optional and frequently omitted.
Timeliness of discharge summary completion
The percentage of discharge summaries available at the time of first post-hospital patient follow-up increased from 43% in February 2012 (5 months prior to implementation of the tool) to 100% in September 2012 (3 months after implementation). The level of discharge summary note availability remained at 100% as of February 2014, which is 1.5 years after implementation (Figure 1).

Percentage of discharged patients with a discharge summary note available in the electronic chart by the time of first follow-up contact (phone call or clinic visit), before and after combined discharge summary note implementation.
Outpatient provider satisfaction with new discharge note
Among the 22 outpatient providers who responded to the survey (response rate 44%), 55% were attending physicians, 23% primary care registered nurses, 14% pharmacists, 5% resident physicians, and 5% did not indicate their position (Table 2). In all, 86% of the respondents indicated they always or most of the time review the discharge summary of recently discharged patients prior to their primary care appointment. In total, 90% were mostly or completely satisfied with the new discharge note, and 86% preferred it to the old note. All respondents found it helpful that the discharge note is completed at the time of discharge. When queried about areas for improvement to the new discharge summary, respondents most often replied that the discharge medication list required further work to highlight changes made during the hospitalization. The second most common response was that hospital courses were too long, too short, or disorganized.
Outpatient provider use of and satisfaction with the new discharge note and procedure.

Efficiency of discharge process
In 2010, prior to implementation of the new discharge summary note tool, the time between the decision to discharge a patient and posting of the patient discharge instructions note was on average 5.6 h (Figure 2). In 2012, immediately following tool implementation, the time between the decision to discharge and posting of the combined discharge summary note decreased to 4.1 h, a difference of 27% (p = 0.04). In 2015, 2.5 years after the discharge summary tool had been implemented, the time required for the discharge process decreased even further to 2.8 h (p < 0.001).

Average hours from decision to discharge patient to discharge note entry in medical record system.
Discussion
This study finds that an electronic discharge summary tool, which facilitates completion of a comprehensive discharge summary at the time of patient discharge, increased the availability of discharge information at the time of outpatient follow-up and improved outpatient providers’ satisfaction with documentation. Importantly, implementation of this tool did not increase the time from decision to discharge a patient to posting of the discharge note. Prior studies have shown that standardizing the content of discharge summaries improves quality, 20 particularly when using an electronic medical record to generate the content.15,16 Other studies have shown that timely sharing of discharge documentation improves outpatient providers’ satisfaction and decreases the likelihood of readmission on subsequent emergency room visits.21–23 Our study further demonstrates that use of an electronic tool coupled with redesign of the discharge summary documentation can improve the timeliness of documentation and outpatient provider satisfaction. Moreover, despite increasing the amount of content in the discharge document, there was no delay in the discharge process, but rather improvement in time to discharge. This improvement is likely related to multiple factors, including changes in workflow (for instance, resident physicians may be more likely to prepare discharge summaries prior to the day of discharge) and other initiatives taking place in the hospital (for instance, care managers may have an increased role in preparing for discharges).
Timeliness and availability of key information post-discharge is a critical issue. At our institution, the majority of patients discharged from an acute care setting are called by a nurse within 48 h of discharge and seen by an outpatient provider within 1–2 weeks. The Joint Commission initiative advocating for a written discharge summary completed within 30 days of discharge falls well short of what is likely needed in current clinical practice to prevent adverse events after discharge. In the era of the electronic medical record, more timely dissemination of discharge information would improve patient care and is not onerous to providers, as demonstrated here. We propose that completion of discharge summaries on the day of discharge should be a goal for all hospitals.
Our combined discharge summary note is unique in that it provides a comprehensive summary of the events of a patient’s hospitalization, outlines changes to the patient’s treatment plan, and highlights items for follow-up. The information provided is more comprehensive than the minimum Joint Commission requirements for discharge summaries. 10 Furthermore, this information is available to all providers who are credentialed to access the VA electronic medical record system at the time the patient physically leaves the hospital. Another unique feature of our intervention is that the printed combined discharge summary, which includes a section written in patient-friendly language, is handed to the patient at the time of discharge. This provision is intended to improve patients’ as well as their caregivers’ understanding of hospital events and encourage patient ownership of their medical problems and follow-up plan.
This study has several limitations. First, as a pre–post evaluation at a single medical center, we are unable to control for all confounders, including temporal trends and other types of activities that might have influenced our results. For example, at the time the discharge summary tool was implemented, a broader inpatient redesign initiative was also underway. 24 Other discharge focused interventions that were part of this initiative included increasing nurse care coordinator and pharmacy involvement during team rounds, holding interdisciplinary meetings to discuss patient discharges, implementing 48 h post-discharge nursing phone calls, and developing an online medication reconciliation tool that helps to populate the medication section of the discharge note. Second, the sample size for observations of the time from physician’s decision to discharge to discharge note completion was smaller in the pre-implementation time period (n = 13), as compared to 2012 (n = 34) and 2015 (n = 64). These peculiar sample sizes resulted from different study goals at the time the various observations took place, as well as resource constraints. Third, because we conducted this study at a teaching hospital, the inpatient resident physician teams change every month and inexperienced interns join the workforce every July. Consequently, there may be changes in the quality and timeliness of discharge documentation on a month-to-month basis that we did not capture. Fourth, the sample size for our provider survey was relatively small. Nonetheless, the consistency in responses across a relatively heterogeneous group of outpatient providers gives us some confidence in our findings. Finally, the timeliness and comprehensiveness of discharge summaries are important to, but do not guarantee, adequate communication between inpatient and outpatient providers. Other important factors that we did not assess include the accuracy of information contained within notes, rates of readership of notes by outpatient providers, and the volume of information within notes, which may distract from the most clinically relevant content.
In conclusion, despite these limitations, this study adds to the literature suggesting that established healthcare systems can learn new tricks that improve the timeliness, comprehensiveness, and outpatient provider satisfaction with communication at the time of patient discharge. To date, our tool has been applied to approximately 3000 hospital discharges per year for more than 3 years and influenced the practice of nearly 150 resident physicians during that time period. Our experience supports the idea that completion of a comprehensive discharge summary document at the time of patient discharge is feasible and useful.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All authors of this article attest that the activities that resulted in producing this article were not conducted as part of a research study, but as part of a non-research evaluation under the authority of VA operations. Thus, ethical approval was not required.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This quality improvement project was supported by the Department of Veterans affairs, Veterans Integrated Service Network (VISN) 11.