
Abstract
Objectives:
Biomarkers representing sympathetic tone and the surgical stress response are measured to objectively evaluate surgical techniques and anaesthetic protocols. If a part of the intraoperative procedure is repeated on the contralateral organ, one animal may potentially serve as its own control and, if so, may minimize the problem of individual differences of the stress response to anaesthesia and surgery. This study aimed to investigate the use of chromogranin A for measurement of the intraoperative sympathetic tone. Additional aims were to investigate chromogranin A and cortisol as indicators of the intraoperative surgical stress response caused by repeated noxious stimuli in dogs subjected to ovariohysterectomy and thereby to investigate the possibility of one dog serving as its own control.
Methods:
Experiments were carried out on 10 dogs subjected to ovariohysterectomy. Perioperative blood samples (0–6) were collected after premedication, immediately before induction of anaesthesia (0), after induction of anaesthesia and before incision (1), before (2) and after (3) removal of the first ovary, after a 15-min pause before removal of the second ovary (4), after removal of the second ovary (5) and after closing the abdomen (6). Plasma chromogranin A and cortisol were analysed.
Results:
Plasma chromogranin A did not change. Plasma cortisol concentration did not change between before anaesthesia and opening of the abdomen. Plasma cortisol increased at removal of the first ovary. Cortisol did not change at removal of the second ovary but remained increased compared to initial sample.
Conclusion:
The results suggest chromogranin A is a poor indicator of intraoperative sympathetic tone during elective surgery in dogs. Cortisol measurement was useful for assessment of intraoperative noxious stimuli. However, at these test conditions, neither plasma chromogranin A nor plasma cortisol was useful for assessment of repeated intraoperative noxious stimuli where one dog served as its own control.
Keywords
Introduction
The noxious stimuli caused by surgery triggers a stress response1–3 which can be used for assessment and evaluation of surgical methods and anaesthetic protocols in cats, 4 dogs5–9 and humans.10–13 The stress response can be evaluated by comparison of biomarkers in blood samples collected in the intra- or postoperative period. Exposure to a clinical setting causes a stress response which differs both among breeds and among individual dogs, 14 and the stress response to various anaesthetic agents vary in dogs 15 as well as in people. 16
If a part of the intraoperative procedure is repeated on the contralateral side, an animal may potentially serve as its own control for comparisons of different techniques in a cross-over design and thereby minimize the problem with individual and breed variation. The stress responses to a first and a second noxious stimulus in the same animal may be compared, whereby the problem of individual variation may be reduced. The removal of ovaries is considered to be the maximum noxious stimuli during ovariohysterectomy (OHE) of dogs5,17 and offers one such repetitive event. Moreover, if an animal can serve as its own control, the number of animals needed for research could potentially be reduced, which is important for ethical reasons.18–20
The increase of blood pressure during surgery correlates well to changes of concentrations of plasma vasopressin and catecholamines in both dogs 17 and humans. 21 In a previous study of canines subjected to OHE blood pressure, plasma vasopressin and urinary noradrenalin peaked at removal of ovaries, indicative of an increased sympathetic tone at removal of ovaries. 17 A sensory stimulus with a consequent sympathetic response and release of catecholamines affects the haemodynamics. 22 However, the release of noradrenalin, the neurotransmitter of sympathetic neurons, may be difficult to measure since its half-life in blood is short. 23 Therefore, a biomarker representing sympathetic tone may be valuable in measurements of surgical stress.
An alternative method to study the intraoperative sympathetic activity may be to investigate chromogranin A (CgA) which is stored in secretory granules of neuroendocrine tissues and is released together with noradrenalin and adrenalin. Within chromaffin cells, there are numerous granules that contain catecholamines, chromogranin and neuropeptides. A sympathetic stimuli causes aggregation and exocytosis of granules, and the content is released. 24 In man, the biomarker CgA is considered a reliable indicator of marked increase of sympathetic tone as it correlates with norepinephrine release rate.25–27 CgA is relatively stable in plasma compared to the neurotransmitters and is used as a parameter to measure stress in conscious dogs. 28 The structure and homology of the molecule, the specific epitopes of the molecule that can be used to analyse CgA in both dogs and cats, are described, 29 but the tests had not been validated when the previous study 17 of surgical stress was performed. The CgA17-38 assay has been used earlier to measure CgA in other species. 30
Cortisol is used as a biomarker of stress. Findings on cortisol in the intraoperative period in dogs subjected to OHE are partly in conflict. One reason may be that the anaesthetic protocol affects the stress response. Therefore, studies with differences in anaesthesia may therefore yield different results. An increased plasma cortisol was reported before skin incision compared to before induction of anaesthesia with one anaesthetic protocol but no increase was reported at removal of ovaries. 31 In comparisons of different anaesthetic protocols, cortisol increased during surgery at or after removal of the second ovary.32,33 Fox et al. 34 reported a doubled plasma cortisol concentration between skin incision and manipulation of ovaries. On the other hand, no intraoperative increase of cortisol was found in dogs subjected to OHE when epidural and systemic tramadol were compared. 35
This study aimed to investigate the use of CgA for measurement of the intraoperative sympathetic tone. An additional aim was to investigate the use of CgA and cortisol as indicators of the intraoperative surgical stress response caused by repeated noxious stimuli in dogs subjected to OHE, and thereby investigate the possibility of one dog serving as its own control. Perioperative plasma samples from a previously reported study were used for the analysis. 17
Methods
Animals
In total, 10 privately owned, intact female dogs destined for elective neutering at the University Animal Hospital, Swedish University of Agricultural Sciences (SLU), were used in the study. Detailed information on the animals is previously reported. 17 The mean (±standard deviation (SD)) age and weight of the dogs was 44 (±31) months and 23 (±7) kg, respectively. Written consent was obtained from the owners of the dogs. The study was approved by the Uppsala Animal Ethics Committee, Sweden and Swedish Board of Agriculture (C 127/10). The animals were treated according to national law and institutional guidelines, in order to ensure animal welfare.
Design of study
A prospective experimental study was designed to investigate biomarkers of perioperative stress. Plasma CgA and cortisol were analysed in blood samples collected in the previously reported study where healthy dogs were subjected to elective OHE. 17 In short, the dogs were admitted to the University Animal Hospital for routine neutering, and blood samples were collected in the perioperative period for later analysis of biomarkers of the surgical stress response.
Premedication and surgery
The dogs were pre-medicated with a combination of sedative and analgesic drugs, acepromazine (Plegicil vet; Vericore Ltd) at 0.03 mg/kg intramuscular (i.m.), carprofen (Rimadyl vet; Pfizer ApS) at 4 mg/kg subcutaneous (s.c.) and methadone hydrochloride (Metadon Recip; Recip AB) at 0.2 mg/kg s.c. Anaesthesia was induced with propofol (Rapinovet vet; Schering-Plough A/S), the dogs were intubated and anaesthesia was maintained with isoflurane (Isoba vet; Schering-Plough A/S) in a mixture of oxygen and air. The surgical procedure for OHE was previously reported. 17 In short, the dogs were placed in dorsoventral recumbency and prepared for surgery. The abdomen was opened, the ovarian pedicle was double ligated and the first ovary was removed. After a 15-min pause, the procedure was repeated for the second ovary, after which the uterus was removed, and the abdomen and skin incision was closed.
Collection of pre- and intraoperative samples
A blood sample was collected prior to surgery, and six samples were collected intraoperatively. Each step of the procedure was followed by a pause to decrease carry-over effects. Blood samples 0–6 were collected after premedication, immediately before induction of anaesthesia (0), after induction of anaesthesia and before incision (1), before (2) and after (3) removal of the first ovary, after a 15-min pause before removal of the second ovary (4), after removal of the second ovary (5) and after closing the abdomen (6). Time of events is given in Table 1.
Plasma chromogranin A (CgA) and cortisol concentrations measured at each event during ovariohysterectomy in 10 dogs.
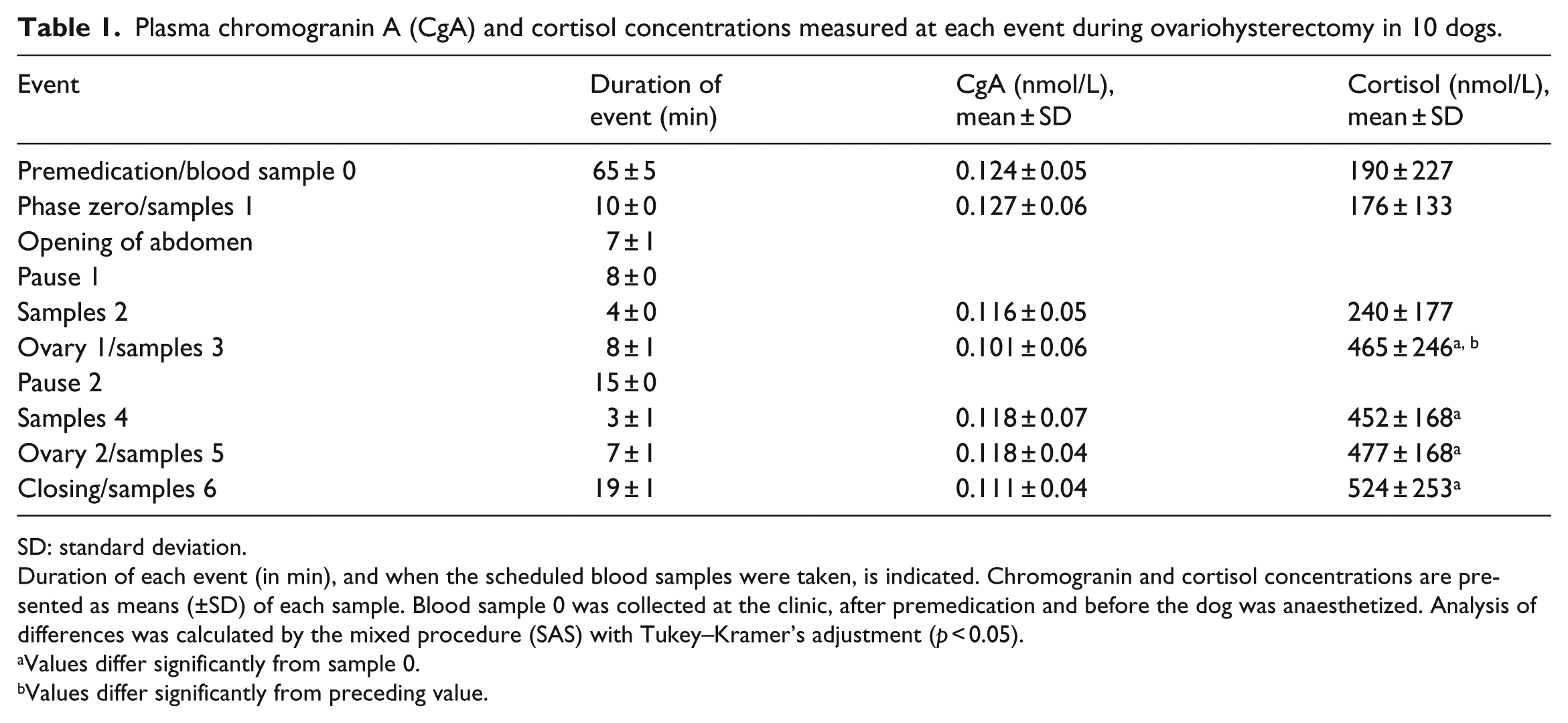
SD: standard deviation.
Duration of each event (in min), and when the scheduled blood samples were taken, is indicated. Chromogranin and cortisol concentrations are presented as means (±SD) of each sample. Blood sample 0 was collected at the clinic, after premedication and before the dog was anaesthetized. Analysis of differences was calculated by the mixed procedure (SAS) with Tukey–Kramer’s adjustment (p < 0.05).
Values differ significantly from sample 0.
Values differ significantly from preceding value.
CgA measurements
Competitive radioimmunoassays (RIAs) were used to measure defined parts of the CgA molecules. The assays are previously described and have been validated by our research group for use in dogs.29,36
Cortisol measurement
The plasma cortisol concentration was analysed in duplicates using an enzyme-linked immunosorbent assay (ELISA) kit for human use (IBL International Gmbh) and validated for canine plasma. Intra-assay coefficient of variation (CV) was calculated as the difference between duplicates using a precision profile, that is, the smoothed relationship of concentration error expressed as %CV value versus concentration. 37 The recovery of cortisol in spiked plasma samples was on average 99.2%. Intra-assay CV for cortisol was <10% (between 31.7 and 2208 nmol/L). Intra-assay CV for cortisol was 3.4% at 178.5 nmol/L and 4.0% at 552.7 nmol/L. The minimum detectable value was 8.2 nmol/L.
Statistical analysis
The effects of various perioperative events on plasma cortisol and CgA concentrations were analysed using mixed linear models for repeated-measures data.38,39 Analysis of differences was calculated by the mixed procedure (SAS) with Tukey–Kramer’s adjustment (p < 0.05). 40 No power calculation or sample size calculation was done. All the available samples from the previous study were used for analysis.
Results
CgA
The mean (±SD) plasma concentration of CgA (Table 1) in samples 0–6 was between 0.101 (±0.06) and 0.127 (±0.06) nmol/L (minimum ± SD and maximum ± SD). Plasma CgA concentration did not change during surgery (n.s., p > 0.05).
Cortisol
The mean (±SD) plasma concentration of cortisol (Table 1, Figure 1) was 190 (±227) nmol/L before surgery (sample 0). After induction of anaesthesia and opening of the abdomen, the plasma cortisol concentration did not change, 176 (±133) nmol/L and 240 (±177) nmol/L, respectively. After removal of the first ovary, the plasma cortisol concentration increased to 465 (±246) nmol/L. Plasma cortisol concentration did not change at removal of the second ovary compared to first ovary, but remained increased compared to sample 0 throughout the surgical procedure.

Plasma cortisol concentrations in samples collected perioperatively in 10 dogs subjected to ovariohysterectomy. The mean (±SD) concentration of cortisol was 190 (±227) nmol/L before surgery (sample 0). After induction of anaesthesia (1) and opening of the abdomen (2), the plasma cortisol concentration did not change, 176 (±133) nmol/L and 240 (±177) nmol/L, respectively. After removal of the first ovary (3), plasma cortisol concentration increased to 465 (±246) nmol/L. Plasma cortisol concentration did not change after a 15-min pause before removal of the second ovary (4) or at removal of the second ovary (5) or at end of surgery (6) compared to first ovary but remained increased compared to sample 0. When symbols are filled, values differ from sample 0 (p < 0.05).
The possible use of the studied biomarkers for analysis of repeated noxious stimuli where one dog was suggested to serve as its own control was not investigated further as cortisol did not increase at removal of second ovary and intraoperative CgA did not change.
Discussion
The results showed that the CgA concentration did not change during surgery, which suggested that CgA is a poor indicator of intraoperative sympathetic tone. Cortisol concentration increased at removal of the first ovary but did not increase further at removal of the second ovary. Therefore, analysis of cortisol seems to be valuable for measurement of intraoperative surgical stress with the used anaesthetic protocol in dogs. Neither CgA nor cortisol seems to be suitable for measurement of surgical stress caused by repeated noxious stimuli at these test conditions. Therefore, one dog could not serve as its own control with the used anaesthetic protocol and the studied biomarkers.
In human subjects, a proportional stress response to the degree of surgical trauma is described.41,42 The noxious stimuli and release of cortisol caused by incision and opening of the abdomen in this study were less compared to removal of ovaries. This was in line with our previous studies where no increase of either blood pressure or the vasopressin concentration was registered at opening of the abdomen during OHE in dogs.5,17 These results are also in agreement with other studies in dogs where no beneficial effect on postoperative pain was found by infiltration of local anaesthesia at the incision,43,44 by a shorter versus longer abdominal incision 45 or by reduction of the number of portals used in laparoscopic procedures. 46 Our interpretation is that minimized surgical stress and noxious stimuli at removal of ovaries are important to consider in development of new techniques for reduced postoperative pain.
Removal of the first ovary increased plasma cortisol concentration. This demonstrates that stretching of the mesovarium, its ligation and transection caused an intense noxious stimulus. These results are in agreement with previous studies on plasma cortisol in dogs32–34 and intraoperative blood pressure measurements in dogs subjected to OHE.5,17,33 After removal of the second ovary, following a 15-min pause, the cortisol concentration remained constant but was continuously increased compared to initial concentration throughout the procedure. A further increase of cortisol at removal of second ovary was possibly blocked by negative feedback. However, it is suggested that during stress of laparotomy in humans, the behaviour of the human pituitary–adrenal system does not conform to the specifications of a negative feedback mechanism. 47 The increase in adrenocorticotropic hormone (ACTH) secretion during surgery in humans is often considerably more than that required to produce a maximum adrenocortical response. 48 In Engquist and coworkers’ study 48 of human subjects, exogenous ACTH was used, which makes comparisons difficult. Furthermore, opioid may affect ACTH release in animals and humans.49,50 The plasma clearance of cortisol is related to plasma binding, with a half-life of 66–80 min at normal hormone levels in humans.51–53 The authors’ opinion is that plasma clearance of cortisol only slightly affected the results as the pause between ovary removals was 15 min.
In this study, CgA was measured in order to assess sympathetic tone as a measure of surgical stress. The results were in agreement with other studies where no increase of noradrenalin concentrations during OHE was found in blood samples obtained before and after removal of ovaries in dogs.31,33,35 In our previous study, 17 the first urinary sample was collected by the owner at home, whereas the first plasma sample, used as baseline in this study, was collected after arrival and premedication at the animal hospital. Animal hospital visits with associated veterinary care are stressful events.14,54,55 Furthermore, Catestatin, a cleavage product of CgA, can modulate the release of catecholamines.56,57 The different baselines make comparisons between (previous study) urinary noradrenalin and (this study) plasma CgA difficult and comparisons should be done cautiously. In the previous study, 17 if the urinary sample collected after induction of anaesthesia was used as baseline, urinary noradrenalin did not change at ovary removal (data on file), which is in agreement with the plasma CgA results of this study.
An alternative explanation of the CgA results may be there is a difference both in CgA content between adrenal medulla and sympathetic nerve endings and in response at sympathetic stimuli. In humans, only high-intensity exercise elevated CgA which peaked 2 min after exercise. 58 Short-term, high-intensity exercise predominantly stimulated noradrenalin release from synaptic nerve endings. In humans, adrenal medulla contained far more CgA than synaptic nerve. 58 A possible interpretation of our results is that intraoperative noxious stimuli stimulated release of noradrenalin from nerve endings, but not from adrenal medulla. However, further studies are needed.
There were study limitations. The number of animals included in the trial was low, and the results should therefore be interpreted cautiously. A possible confounder is that the plasma samples had been thawed earlier for analysis in the previous study, but it is unlikely that this thawing affected the analysis because CgA is considered a stable molecule.
Conclusion
The results suggest CgA is a poor indicator of sympathetic tone during elective surgery in dogs. To evaluate intraoperative noxious stimuli, cortisol measurement is valuable in dogs. However, to assess repeated intraoperative noxious stimuli where one dog serves as its own control, measurements of neither plasma CgA nor plasma cortisol are useful with the present anaesthetic protocol and sampling interval.
Footnotes
Acknowledgements
The authors thank Kerstin Olsson, Åsa Eriksson and Gunilla Drugge at Department of Anatomy, Physiology and Biochemistry, SLU, for their invaluable assistance and technical advice.
Declaration of conflicting interests
The authors declare that they have no conflicting interests.
Funding
This project was financially supported by Amanda Personnes’ Research Fund, Sweden.