
Abstract
Objectives:
Patients with peripheral artery disease have walking impairment, greater thrombotic risk, and are often treated with exercise training. We sought to determine the effect of a 3-month-long exercise program on clot strength among patients with peripheral artery disease and intermittent claudication.
Methods:
Twenty-three symptomatic peripheral artery disease patients were randomly assigned to a walking exercise program or to an attention control group who performed light resistance exercise. We investigated the effect of exercise training on clot strength and time to clot formation was assessed by thromboelastography.
Results:
After 3 months of exercise, clot strength (maximal amplitude) and time to clot formation (R) did not change significantly from baseline, even after improvements in claudication onset time (p < 0.01) and peak walking time (p < 0.05). Furthermore, changes in clot formation parameters were not significantly different between groups. Among the 10 individuals demonstrating a reduction in clot strength (reduced maximal amplitude), one was a smoker (10%) compared to 9 of 13 non-responders (69%) whose maximal amplitude was unchanged or increased (p = 0.0097).
Conclusion:
In this ancillary study, a 12-week walking program improved ambulatory function in peripheral artery disease patients with claudication, but does not modify clot strength or time to clot formation. Larger studies are needed to confirm these hypothesis generating findings and to determine whether a different amount or type of exercise may induce a change in clotting in this patient population.
Introduction
Peripheral artery disease (PAD) is associated with exercise impairment and greater cardiovascular morbidity and mortality.1,2 Supervised and home-based exercise programs are efficacious for the clinical management of claudication and improve objective ambulatory measures, such as claudication onset time (COT), peak walking time (PWT), and 6-min walk performance in PAD patients.3,4
Cardiovascular morbidity and mortality in symptomatic PAD patients is associated with higher thrombotic risk,5,6 and these patients may benefit from intensification of antithrombotic therapy. 7 The coagulation system may impact exercise performance since clot strength (maximal amplitude (MA)) is inversely correlated with objective and self-perceived ambulatory measures at baseline in patients with PAD and claudication. 8 Furthermore, acute exercise may have an impact on the coagulation system, but results have been controversial, as strenuous exercise induces clotting in some studies,9–11 but not in others.12–16 In contrast, it appears that chronic exercise training positively modifies exercise-induced blood coagulation;17–19 however, evidence is limited in patients with PAD and claudication.
In PAD patients with claudication, the impact of exercise training on clot strength, which reflects the end result of the coagulation cascade and the contribution of platelets to form the clot, is poorly understood. The primary objective of this ancillary study was to determine the effect of a 3-month-long exercise program on clot strength among patients with PAD and intermittent claudication. In addition, we evaluated whether exercise training induces any changes in time to clot formation in these patients.
Methods
Subjects
This was an ancillary study for a larger randomized, controlled clinical trial, and established laboratory methods were utilized (ClinicalTrials.gov Identifier: NCT00618670). This supplementary study aimed to generate preliminary estimates of the effect size and variability of clot strength. This analysis included 23 symptomatic patients with lower extremity PAD from a cohort of patients enrolled in a prospective, randomized, controlled clinical trial that compared a home-based exercise program with a supervised exercise program and its impact on exercise performance. 20 The study was performed at the General Clinical Research Center at the University of Oklahoma Health Sciences Center and was sanctioned by The Institutional Review Board at the University of Oklahoma Health Sciences Center. Patients who had intermittent claudication secondary to vascular insufficiency were included if they had (1) a history of any type of exertional leg pain, (2) ambulation during a graded treadmill test that was limited by leg pain consistent with intermittent claudication, and (3) an ankle brachial index (ABI) ⩽ 0.90 at rest or an ABI ⩽ 0.73 after exercise.
Patients were excluded for the following conditions: (1) absence of PAD (ABI > 0.90 at rest and ABI > 0.73 after exercise); (2) inability to obtain an ABI measure because of non-compressible vessels; (3) asymptomatic PAD determined from the medical history and verified during the graded treadmill test; (4) use of cilostazol and pentoxifylline initiated within 3 months before investigation, because these drugs may improve the patient’s ambulatory function; (5) exercise tolerance limited by factors other than leg pain; and (6) active cancer, renal disease, or liver disease. 4 This analysis did not include any patients that were using coumadin, because it affects clot formation. The local institutional review board approved this ancillary study and only those who signed a written informed consent and completed the study were included. Baseline demographic and clinical characteristics were collected on each patient in addition to a detailed physical examination.
Intervention for exercise and control groups
At baseline, patients were randomly assigned to a supervised exercise program, a home-based exercise program, or an attention control program, and they were followed for the 3-month intervention period.
Exercise groups
Nine patients completed a supervised exercise rehabilitation program that was designed to elicit increases in COT and PWT, as previously described. 4 This standardized program consisted of 3 months of supervised treadmill walking sessions 3 days per week. Walking duration began at 15 min for the first 2 weeks of the program and progressively increased by 5 min biweekly until a total of 40 min of walking was accomplished during the final 2 weeks of the program. Patients walked at a grade equal to 40% of the final workload from the baseline maximal treadmill test to the point of near-maximal claudication pain, at which point they stopped to relieve their leg pain. Patients then repeated the alternating walking and rest periods until the prescribed total number of minutes of exercise was attained for the training session. During each exercise session, patients wore a step activity monitor on the right ankle to quantify the cadence and time of ambulation. Patients in the supervised program were not given advice or instructions to perform additional exercise away from our research center. 4 Although acute bouts of ischemia during walking increase reactive oxygen species at the end of exercise, 21 we have found that chronic levels of habitual ambulatory activity have no influence on oxidative stress and are associated with lower levels of inflammation. 22
Seven patients completed a home-based exercise rehabilitation program that was designed to be as similar to the supervised exercise program as possible and consisted of 12 weeks of intermittent walking to near-maximal claudication pain 3 days per week at a self-selected pace. Walking duration began at 20 min for the first 2 weeks and progressively increased 5 min biweekly until a total of 45 min of walking was accomplished during the final 2 weeks of the program. Exercise sessions were rigorously quantified with a step activity monitor (StepWatch3™; Orthoinnovations, Inc., Oklahoma City, OK, USA) to accurately record the duration and cadence of ambulation, and an exercise logbook was used to record the walking sessions. During follow-up meetings, patients discussed their progress with an exercise physiologist, were given feedback about the data from the step activity monitor, and were given new instructions on changes in exercise duration. These patients did not perform any exercise in our facility during the meetings with the research staff. 4
For this study, patients in both the home-based and the supervised exercise groups were merged into a single group (n = 16), as it has been previously shown that the home-based exercise program has high adherence and is efficacious in improving claudication measures to a similar extent as our standard supervised exercise program.4,20
Attention control group
Patients randomized to this group (n = 7) participated in supervised light resistance training over the 3-month study period. Light resistance training was performed three times per week, without any walking exercise, using a Pro-Form Fusion 6.0 LX weight system. On entry, the resistance that caused fatigue in various muscle groups after 15 repetitions (15-rep maximum) was established and was reassessed each month. The resistance training phase consisted of performing upper extremity exercises that included the bench press, military press, butterfly, biceps curl, triceps press down, and lat pull-down. Lower extremity exercises included the leg press, leg curl, and leg extension. One set of 15 repetitions was performed for each exercise. If the resistance from the exercise machine could not be lifted, resistance bands were used instead. During each exercise session, patients wore a step activity monitor to quantify the total time of their visit, which served as a measure of the amount of exposure they had with the research staff. Patients were encouraged to walk more on their own, but they did not receive specific recommendations about an exercise program during the study. This approach is similar to advice typically given by clinicians during routine follow-up vascular appointments. 4 No other risk factor management, lifestyle modification, or educational programming interventions were provided to any of the patients.
Primary outcomes: clot strength (MA) and time to clot formation (R)
Whole blood samples at rest were obtained at baseline and at the end of the study. Clot formation parameters were measured by thromboelastography (TEG). Within 2 h of drawing, citrated whole blood was activated with kaolin, and calcium citrate was added to obtain the thrombin-induced clot. The TEG Hemostasis System (Haemonetics Corporation, Braintree, MA, USA) provided quantitative measurements of the physical properties of the clot, which formed the primary outcome measure in the study consisting of the clot strength (MA) and the time to clot formation (R). In subsequent analyses, patients in either the exercise or the attention control group were considered responders to intervention if they had any reduction in MA at follow-up.
Secondary outcomes: ambulation and exercise performance
ABI test
ABI was determined by obtaining the ankle and brachial systolic blood pressures, as previously described. 4
Graded maximal treadmill test
Patients performed a progressive, graded treadmill protocol (2 mile/h, 0% grade with 2% increase every 2 min) until maximal claudication pain occurred. 23 The COT and the PWT were obtained. COT was defined as the walking time at which the patient first experienced pain, and PWT was defined as the time at which ambulation could not continue because of maximal pain. 4
6-min walk test
Patients performed an over-the-ground, 6-min walk test supervised by trained exercise technicians, as previously described. 24 The total distance walked during the test was recorded. The test–retest intra-class reliability coefficient is R = 0.94 for total 6-min walking distance. 24
Ambulatory activity monitoring and physical activity questionnaire
Daily Ambulatory Activity (presented as strides/day and minutes/day) was measured with a step activity monitor during seven consecutive days at baseline and at the end of the study. The monitor, attached to the right ankle above the lateral malleolus with elastic Velcro straps, continuously recorded the number of strides taken on a minute-to-minute basis. 4 Additionally, self-reported physical activity level was assessed with the Baltimore Activity Scale for Intermittent Claudication (BASIC) questionnaire. 25
Statistical analyses
A Spearman’s rank correlation coefficient was used to quantify the strength of the linear association between measures of changes in clot strength and changes in exercise performance. Partial correlation coefficients were estimated after adjustment for baseline ABI, smoking status, and the number of metabolic syndrome factors, where each covariate factor was considered separately. The distribution of continuous measures was compared between participants in the attention control and the exercise group using a non-parametric Wilcoxon rank-sum test, which was chosen given the skewed nature of the data distributions and the small sample size in each group. Analyses of within-group changes were performed using a non-parametric Wilcoxon signed-rank test, to account for the pairing between pre- and post-intervention observations. Proportions were compared between groups using a Chi-square test or Fisher’s exact test if at least 20% of the expected table frequencies were less than 5. Linear regression models were used to test the significance of the difference in means between exercise and control participants after adjusting for baseline ABI, smoking status, and the number of metabolic syndrome factors, where each covariate factor was considered separately. A two-sided 0.05 alpha level was used to define statistical significance. Data were analyzed using SAS (SAS System for Windows, ver. 9.2; SAS Institute Inc., Cary, NC, USA).
Results
Twenty-three symptomatic PAD patients were included in this ancillary study. Baseline demographic and clinical characteristics are summarized for the exercise and attention control groups in Table 1. All clinical characteristics are similar in both groups, except for ABI, which was lower in those patients included in the exercise group.
Clinical characteristics for symptomatic PAD subjects in the exercise and the attention control groups.

P25: 25th percentile; P75: 75th percentile; BMI: body mass index; PAD: peripheral artery disease.
Values are median (P25–P75) or count (percentages).
Patients in both the attention control and exercise groups completed a similar number of their interventional sessions (median (P25–P75) of 36 (35–36) and 36 (34–36), respectively). A detailed description of the intervention that summarizes the training parameters for the patients in the exercise group is shown in Table 2.
Exercise training parameters for each exercise group a .

P25: 25th percentile; P75: 75th percentile.
Values are median (P25–P75).
Median measures did not differ significantly between home-based and the supervised exercise groups (p > 0.20 for each, Wilcoxon rank-sum test).
Exercise performance parameters at baseline and after the intervention are shown in Table 3. All patients included in this analysis had considerable walking impairment typically seen in patients with claudication, as reflected by their COT, PWT, 6-min walk distance, daily ambulatory activity, and BASIC total score at baseline. Patients in the exercise group had lower 6-min walk distance and daily ambulatory activity before the intervention when compared to the control group. The exercise group demonstrated significant increases in COT, PWT, 6-min walk distance, and BASIC total score, while the control group only had a significant increase in 6-min walk distance (Table 3). There was a trend for the change score in PWT to be greater in the exercise group (p = 0.07) than in the control group, whereas the change scores for the remaining variables were not significantly different between groups.
Exercise performance measures at baseline (pre-intervention), after 3 months of follow-up (post-intervention), and the change score for each group of participants.

P25: 25th percentile; P75: 75th percentile; BASIC: Baltimore Activity Scale for Intermittent Claudication.
Values are median (P25–P75).
Significantly different than the pre-intervention value: *p < 0.05; **p < 0.01.
The clot formation measures at baseline and at the end of the intervention period are shown in Table 4. Clot strength (MA) and time to clot formation (R) did not differ significantly between the control and exercise groups at baseline or after the intervention. Furthermore, within-group changes in MA and R were not significant in either group, and there was no significant difference in the change scores between groups. After separate adjustments for ABI, the number of metabolic syndrome factors, and smoking status, the clot formation measures did not differ significantly between the control and exercise groups except for the post-intervention measurement of R (Table 5). In the unadjusted model, R was significantly shorter in the exercise group compared to the control group (mean difference = 1.1 min shorter, 95% confidence interval (CI): 0.06–2.1 min shorter, p = 0.039). Additionally, in the model adjusted for baseline smoking status, R was significantly shorter in the exercise group at the post-intervention time point (mean difference = 1.2 min shorter, 95% CI: 0.1–2.2 min shorter, p = 0.033). No significant correlations between change in exercise parameters and changes in clot strength (MA) were found, even after separate adjustments for baseline ABI, the number of metabolic syndrome factors, and smoking status (data not shown).
Clot formation measures at baseline (pre-intervention), after 3 months of follow-up (post-intervention), and the change score for each group of participants.

MA: maximal amplitude.
Values are median (P25–P75).
Overall hypothesis test, Kruskal–Wallis test.
Comparisons of clot formation measures between the exercise and attention control groups after adjustment for potential baseline confounding factors (ABI, the number of metabolic syndrome factors, or smoking).
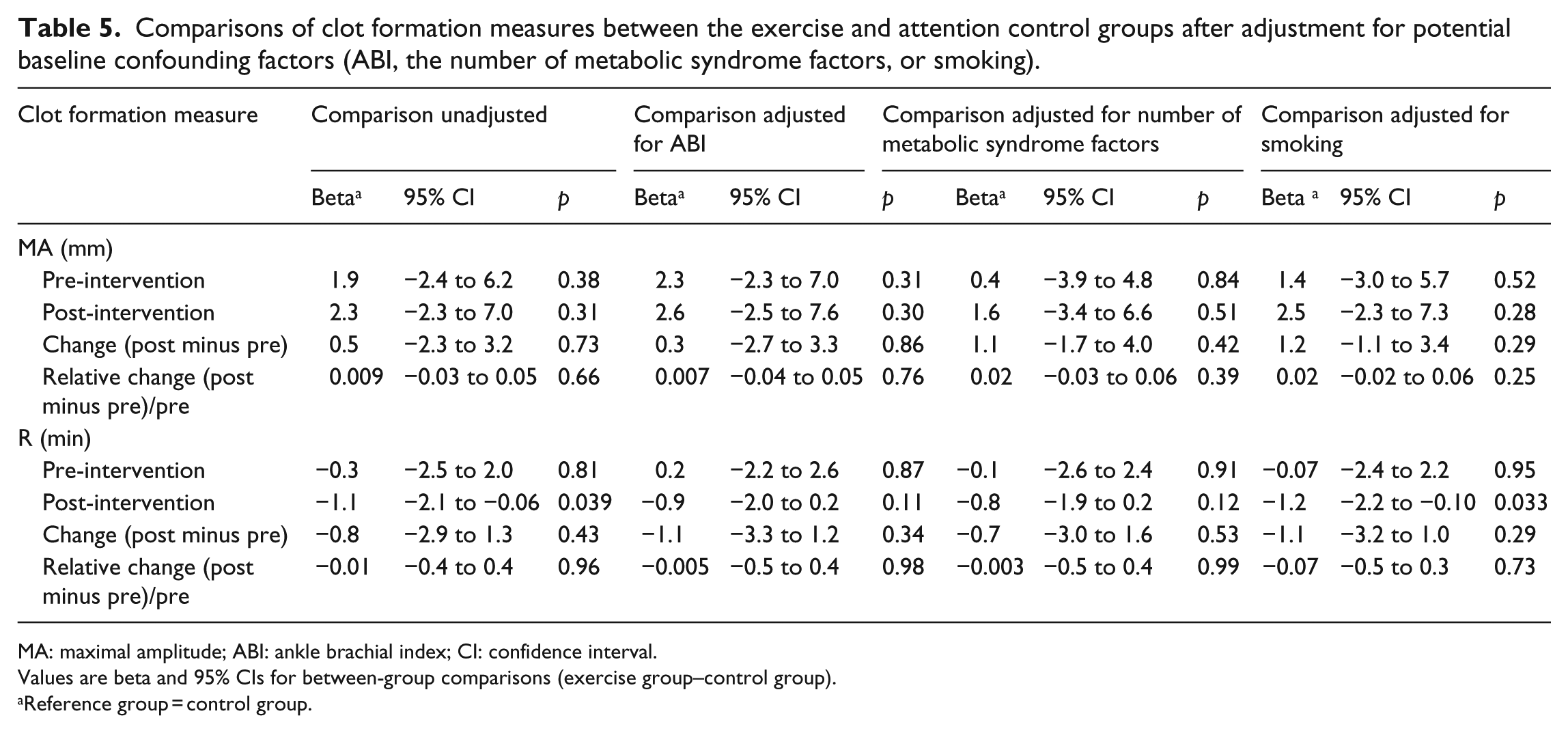
MA: maximal amplitude; ABI: ankle brachial index; CI: confidence interval.
Values are beta and 95% CIs for between-group comparisons (exercise group–control group).
Reference group = control group.
A secondary analysis was performed to determine whether a change in MA during the study, defined as a response irrespective of the intervention, was associated with baseline and intervention measures. Overall, at the end of the study, 10 patients demonstrated a decrease in MA (and were considered responders), and 13 patients demonstrated no change or had an increase in MA (and were considered non-responders). There were no differences in the number and percentage of responders in the control and the exercise groups (3 (43%) and 7 (44%), respectively; p > 0.95). Overall, responders and non-responders did not differ significantly in terms of their changes in exercise parameters (data not shown). However, non-responders were more likely to report active smoking at baseline (69%) as compared to responders whose MA value decreased (10%) (p = 0.0097).
Discussion
Our primary finding was that a 3-month-long exercise program does not have a significant impact on clot strength and time to clot formation when compared to an attention control group of PAD patients with intermittent claudication. Therefore, our results suggest that a low-intensity walking program during 12 weeks does not modify overall clot formation, but larger studies are needed to confirm our findings and determine whether a different amount or type of exercise may induce a change in clotting in this patient population.
Activation of the coagulation system depends on both accelerated clot formation (shorter R) and increased clot strength (higher MA), so we evaluated both parameters. Neither clot strength nor time to clot formation changed after the patients completed a well-characterized and effective exercise program that improved their overall ambulatory function, as expressed by the favorable changes in COT, PWT, 6-min walk total distance, and BASIC total score. Based on the negative results, we may infer that the walking programs performed by patients with PAD improve their walking, but do not affect clot formation per se. Therefore, to change these parameters, a different exercise program or other types of treatment (e.g. medication) may be required.
Even though other studies have evaluated the impact of exercise on the coagulation cascade,26,27 this is the first to evaluate changes in quantitative clot formation parameters, in particular clot strength, in PAD patients treated with a closely monitored specific exercise program and evaluated with objective measures of ambulatory function. A previous study in PAD showed that treatment of patients with claudication by supervised exercise did not result in significant improvements on the thrombin–antithrombin complex and prothrombin fragments 1 and 2 (both markers of thrombin generation). 26 Thrombin generation is a measure of pro-thrombotic activity, but it does not evaluate other factors that contribute to the formation of the clot, such as platelets. In this study, we measured clot strength, which is a measure of the end result obtained when the coagulation cascade is activated and induces clot formation with the contribution of platelets. In concordance with the previous study, we did not find any effect of exercise training on clot strength. However, further investigations and larger studies may be needed to determine the impact of exercise training in PAD patients on the different levels of the coagulation system.
Other factors that affect the coagulation system, such as smoking, may have contributed to our negative results. Smokers are more susceptible to thrombosis due to decreased fibrinolytic activity, 28 and they have greater clot strength. 29 In our study, responders were less likely to report current smoking; among the 10 individuals demonstrating a reduction in clot strength (responder), 1 was a smoker (10%) compared to 9 of 13 non-responders whose MA was unchanged or increased after the intervention (69%). Even though responders and non-responders did not differ significantly in terms of their changes in exercise parameters, current smoking was significantly associated with MA response. This suggests that the effect of smoking on clot formation could have minimized any positive exercise-mediated changes in clot strength. This possibility should be considered and further investigated.
Our study has inherent limitations. Since it was an ancillary study to explore the effect of a structured exercise program on clot strength in PAD patients, we had a small sample size. Therefore, our results need to be confirmed in larger studies. Our estimated change scores and their variability may be valuable in future studies to help determine required sample sizes to ensure sufficient statistical power. Despite the small sample size, we demonstrated efficacy for improving ambulation times within the exercise group. There is certainty that the patients in our study followed the exercise program correctly, because patients were closely monitored. Thus, the absence of change in clot formation parameters was not associated with deficiencies in the exercise program or problems with exercise compliance. By design, the attention control group performed light resistance training exercise. This may be considered a study limitation because it may have minimized the chance of detecting differences in changes in clot formation with the exercise group. Another study limitation is that the patients in the exercise group had more severe PAD, as reflected by a worse ABI at baseline. This may be due to more patients in the attention control group having a history of lower extremity revascularization when compared to the exercise group, even though this trend was not statistically significant. Additionally, this study is limited to PAD patients who have intermittent claudication, and may not be generalized to patients with less or more severe disease.
Conclusion
A well-structured, low-intensity walking program during 12 weeks improves ambulatory function in PAD patients with intermittent claudication, but does not modify clot strength or time to clot formation. Larger studies are needed to confirm these hypothesis generating findings.
Footnotes
Acknowledgements
J.E.E.: (1) Contributions to conception and design, acquisition of data, analysis, and interpretation of data; (2) drafting the article and revising it critically for important intellectual content; (3) final approval of the version to be published. K.M.: (1) Contributions to conception and design, acquisition of data, analysis, and interpretation of data; (2) drafting the article and revising it critically for important intellectual content; (3) final approval of the version to be published. J.A.S.: (1) Analysis and interpretation of data; (2) revising the article critically for important intellectual content; (3) final approval of the version to be published. J.F.S.: (1) Contributions to conception and design; (2) revising the article critically for important intellectual content; (3) final approval of the version to be published. P.S.M.: (1) Acquisition of data; (2) revising the article critically for important intellectual content; (3) final approval of the version to be published. A.W.G.: (1) Contributions to conception and design, acquisition of data, analysis, and interpretation of data; (2) revising the article critically for important intellectual content; (3) final approval of the version to be published.
Declaration of conflicting interests
The authors declare no conflict of interest in preparing this article.
Funding
This research was supported by the American Heart Association (award number 09BGIA2251080; J.E.E.); the National Institute on Aging (NIA) (grant number R01-AG-24296; A.W.G.); the Oklahoma Center for the Advancement of Science and Technology (grant number HR09-035; A.W.G.); the University of Oklahoma Health Sciences Center General Clinical Research Center sponsored by the National Center for Research Resources from the National Institutes of Health (grant number M01-RR-14467); and partial funding provided by National Institutes of Health, National Institute of General Medical Sciences (grant 1 U54GM104938; J.A.S.).