
Abstract
Objective:
The primary objective was to assess the warming sensation caused by IFF Flavour 316282 in a syrup used for short-term treatment by patients suffering from nasal congestion and mild to moderate body pain, headache, fever or sore throat associated with an upper respiratory tract infection.
Methods:
A single cohort, single treatment arm, open-label study. Subjects received one 30 mL dose of syrup containing IFF Flavour 316282, paracetamol and pseudoephedrine and recorded onset and disappearance of any warming sensation in the mouth/throat. Subjects’ assessments of strength and appeal of the sensation, taste, texture and acceptability of the product was investigated using questionnaires.
Results:
A total of 56 subjects were included; 53 (94.6%) experienced a warming sensation. The median duration of the warming sensation was 114 s (95% confidence interval: 87–120 s). All subjects rated the syrup as excellent, good or fair for treating their symptoms; 100% and 94.6% of subjects respectively described texture and taste as excellent, good or fair. There were no safety concerns, and the syrup was well tolerated. Most subjects liked the warming sensation.
Conclusions:
IFF Flavour 316282 in a syrup for treatment of upper respiratory tract infection symptoms is associated with a warming sensation. The syrup is well tolerated, safe and palatable.
Keywords
Introduction
We recently published the results of a study evaluating the warming sensation caused by the excipient IFF Flavour 316282 (International Flavour and Fragrances, Shrewsbury, NJ, USA), 0.15% weight/volume, in a cough and cold syrup containing paracetamol, phenylephrine and guaifenesin. 1 In that study, 51 subjects with symptoms of upper respiratory tract infection (URTI) were treated with a single 30 mL dose of the syrup, and 47 (92.1%) reported experiencing a warming sensation in the throat and/or back of the mouth, which most found pleasant.
The acceptability of the warming sensation was not unanticipated, but needed to be documented. IFF Flavour 316282 is a flavouring agent, and earlier testing of the base formulation (containing the flavour but without the active cough and cold ingredients) revealed the warming sensation (data on file, Novartis Consumer Health, Inc., Parsippany, NJ, USA). The question arose then as to whether or not the warming sensation might be soothing to patients suffering from URTI symptoms. 1 While anecdotal evidence supports the soothing effects of warmth for some patients suffering from cough, chills, cold, sinus infection and influenza, the actual evidence is scarce. A few papers have referenced the comforting effects of warm liquids such as soups and teas and warming salves, particularly chest rubs,2–5 but until our study, the warming sensation associated with liquids, rubs or drug ingredients had never been formally studied or assessed in terms of patient acceptability. 1
Subsequently, the same excipient flavour has been incorporated in a new over-the-counter (OTC) syrup formulation for the short-term symptomatic treatment of nasal and sinus congestion associated with colds and influenza symptoms such as pain, headache and/or fever. The active ingredients of the syrup are paracetamol and pseudoephedrine, 500 mg and 30 mg, respectively, per 30 mL of syrup; both are well-established pharmaceutical agents commonly found in combination OTC products used to treat symptoms related to colds and influenza. 6 Given the positive outcomes for the warming sensation of the excipient flavour in our previous study, 1 we sought to evaluate its effects in this syrup formulation, targeting patients suffering from nasal congestion and mild to moderate body pain, headache, fever or sore throat associated with a URTI.
Methods and materials
Study population
Subjects (12 years of age and older) suffering from symptoms of a URTI were recruited. At dosing, eligible subjects had to have one or more symptoms in each of two categories: (1) nasal congestion (blocked nose) with or without rhinorrhea (runny nose) or sneezing and (2) mild-to-moderate body pain, headache, fever or sore throat. Exclusions included subjects with productive cough and those with dry cough and/or throat pain of severe intensity, in both cases defined as a rating of 3 on a 4-point ordinal scale where 0 = not present and 3 = severe.
Before any assessments were performed, subjects had to show an understanding of the study procedures, provide written informed consent and indicate their willingness to complete the required assessments. Informed consent was signed by one or both parents or legal guardian for adolescents, who also were asked to sign an informed assent.
The recruitment target was 56 subjects in order to obtain a minimum of 50 evaluable subjects from two centres. This sample size calculation was based on medical rather than statistical grounds, as is normally used for sensory panel tests and acceptability and local tolerability studies. In this case, the goal was to confirm results already seen with placebo syrups containing the excipient flavour in a consumer test using the final formulation.
Study design
The study used a single cohort, single treatment arm, open-label design carried out over 1 day at two centres. Screening occurred when the subjects were seen at the clinic for symptoms of a URTI, and eligible subjects received treatment between 30 min and 6 h after being screened.
The study was conducted according to the ethical principles of the Declaration of Helsinki. Study design and amendments were reviewed and approved by Central Research Ethics Board, Minister of Health and Social Services (Montreal, Quebec) for adolescent subjects or Institutional Review Board (IRB) Services (Aurora, Ontario) for adult subjects.
Study treatment
Each 30 mL dose of study medication contained the active ingredients: paracetamol, 500 mg, and pseudoephedrine, 30 mg. The syrup also contained 0.15% weight/volume of the warming IFF Flavour 316282. While being observed, each subject swallowed a single 30 mL dose of the study medication over a period of 1 min or less, immediately followed by a 1-h observation period.
Use of the following was prohibited from 6 h prior to dosing until the end of the assessment period: inhaler, medicated confectionary, throat lozenges or sprays, any products with demulcent properties (e.g. chewing gums, boiled sweets, mints), any medication for sore throat containing a local anaesthetic, paracetamol, any non-steroidal anti-inflammatory drug (NSAID) or any oral or topical nasal decongestant. Use of antihistamines was prohibited in the 24 h prior to dosing. Gargling, using breath fresheners or menthol or mint-containing products, eating and drinking (other than sipping up to 200 mL of room temperature water for cough or dryness) were disallowed from 1 h before dosing to the end of the assessment period.
Study assessments
Pre-dose
Eligible subjects had a short physical examination, which included evaluation of the oropharynx, vital signs (blood pressure, pulse and temperature) and height and weight measurements (to confirm minimum weight for adolescents). Baseline severity scores were recorded using a 4-point scale (0 = not present; 1 = mild; 2 = moderate; 3 = severe) for each of the following symptoms of a URTI: runny nose, sneezing, blocked nose, sore throat, dry cough, productive cough, headache, fever and body pain.
Subjective warming sensation was defined as a ‘feeling of warmth mainly in the throat and at the back of the mouth’. The baseline score for warming sensation intensity was determined by each subject following ingestion of 30 mL of water at room temperature. Subjects indicated the warming sensation intensity by making a vertical mark on a 100 mm visual analogue scale (VAS), which ranged from ‘no warming sensation’ (=0 mm) to ‘strongest possible warming sensation’ (=100 mm).
Post-dose
Two stopwatches (labelled ‘start of warming’ and ‘end of warming’) were started at the point when the study medication was swallowed (time zero). Subjects were asked to stop the ‘start of warming’ stopwatch as soon as they felt a warming sensation at the back of their throat and to stop the second stopwatch (‘end of warming’) as soon as that sensation disappeared. Subjects rated the warming sensation intensity at 60–75 s after dosing by making a vertical mark on the VAS.
At 10 ± 1 min post-dose subjects were asked to assess the strength of the warming sensation using a 5-point scale where 5 = much too strong and 1 = much too weak. They also rated their overall opinion of the warming sensation by answering the question ‘How do you like the warming sensation you experienced for this product?’ using a 9-point scale where 9 = liked extremely and 1 = disliked extremely.
One hour after dosing, a second physical examination, including assessments of the oropharynx and vital signs, was carried out, and adverse events were recorded. At this time, the subject’s overall opinion of the medication was evaluated using a 5-point scale from 4 = excellent to 0 = unacceptable, and based on the query ‘Taking into account all the benefits and any side effects which you attributed to your study medication, how would you rate the syrup you took for treating cold symptoms?’ the subject’s overall opinion of syrup taste and texture were recorded separately using a similar scale.
Statistical analysis
The intensity of warming sensation at baseline and at 60–75 s post-dose and the onset and duration of warming sensation were summarized. For the intensity of warming sensation, the n, arithmetic mean, standard deviation (SD), median, minimum and maximum values were calculated for pre-dose, post-dose and for the difference (post-dose minus pre-dose). For the onset and duration of warming sensation, the n, minimum, 25th percentile, median and its 95% confidence interval (CI), 75th percentile and maximum values were calculated. The median, its 95% CI and the lower and upper quartiles were estimated using the Kaplan–Meier survival analysis method.
Results
Study population
A total of 56 subjects with a mean age of 33 years (range: 18–62 years) were recruited and all completed the study and were included in the analyses (Table 1). No subjects were discontinued from the study.
Study population demographics (N = 56).
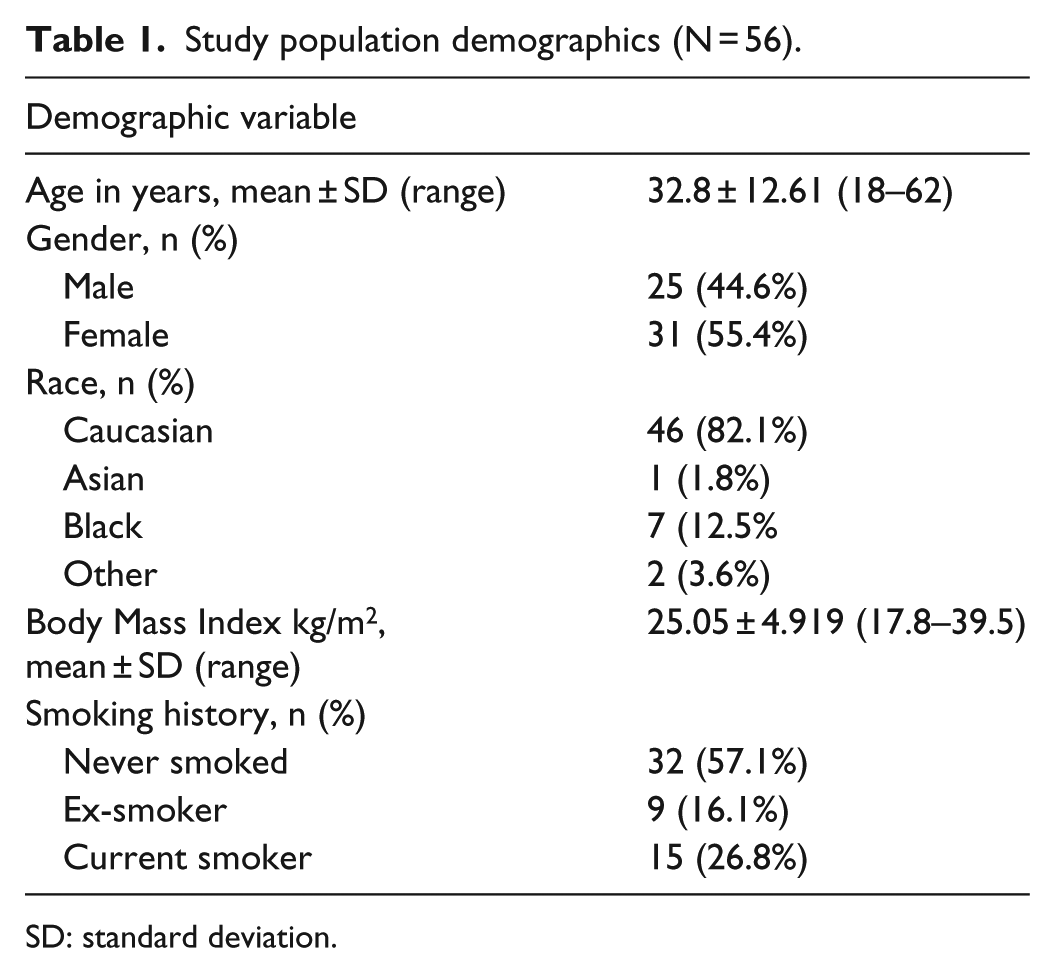
SD: standard deviation.
All subjects were over 18 years of age, and the majority were Caucasian (82.1%). More females (55.4%) than males (44.6%) were enrolled.
Cold and flu symptoms
The presence of URTI symptoms in the study population pre-dose is summarized in Table 2. All symptoms were mild or moderate. Aside from blocked nose, which was required for entry into the study, the three most common symptoms were sore throat pain (92.9%), dry cough (91.0%) and runny nose (85.7%). No subjects had productive cough, and none had fever. One patient did not present with blocked nose, but was included in the analyses.
Presence of mild or moderate upper respiratory tract infection symptoms pre-dose (N = 56).

Warming sensation
A total of 53 subjects (94.6%) experienced a warming sensation. In all, 47 (83.9%) experienced the sensation within 60 s of ingesting the syrup; the other 6 subjects (10.7%) experienced the warming sensation almost immediately, such that their experience of warming had subsided by the time of the 60-s assessment. Three subjects (5.4%) experienced no warming sensation at all.
The median time to onset of warming was 9.5 s (95% CI: 8, 12 s), with times for individual subjects ranging from 2 to 49 s. The interquartile range (Q25 to Q75) was 7–15.5 s. The median duration of warming sensation was 114 s (95% CI: 87–120 s), with durations for individual subjects ranging from 27 to 615 s (10.3 min). The interquartile range was 73–140 s. At 60 s after syrup ingestion, the mean ± SD intensity was 37.7 ± 26.67 mm (range: 0–86 mm) compared to a pre-dose mean intensity of 3.5 ± 7.85 mm (range: 0–39 mm).
The majority of subjects (38, 67.9%) described the warming sensation as ‘pleasantly warming or just about right’ (Table 3), and overall, 39 subjects (69.6%) liked the warming sensation (Table 4). Six subjects (10.7%) disliked the sensation, while 11 (19.6%) neither liked nor disliked the experience.
Subjects’ assessments of strength of warming sensation at 10 min post-dose.
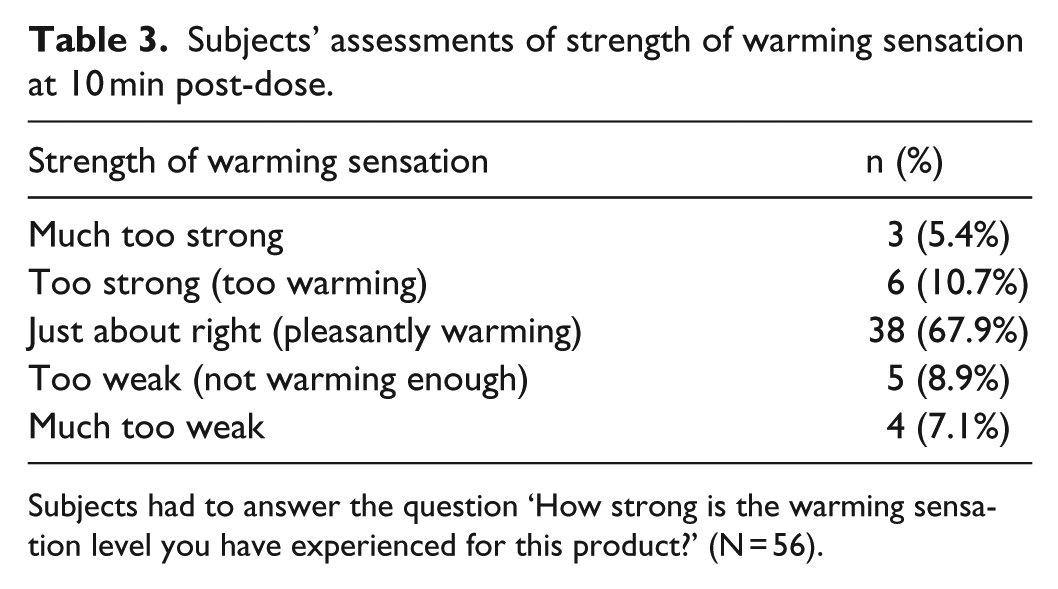
Subjects had to answer the question ‘How strong is the warming sensation level you have experienced for this product?’ (N = 56).
Subjects’ overall opinions of warming sensation at 10 min post-dose.

Subjects had to answer the question ‘How do you like the warming sensation you have experienced for this product?’ (N = 56).
Acceptability of the syrup
Subject acceptability and overall opinion of the syrup are summarized in Tables 5 and 6. The majority of patients (44, 78.6%) rated the syrup as good or excellent for treating their URTI symptoms after 1 h. Twelve (21.4%) rated the syrup as fair; no subjects considered the treatment poor or unacceptable. Taste and texture of the syrup were also rated as good or excellent by the majority of subjects: 33 (58.9%) and 50 (89.3%), respectively. Twenty subjects (35.7%) rated taste as fair (or ‘as expected’); 6 (10.7%) gave a similar rating for texture. No subjects considered taste to be unacceptable, although 3 (5.4%) reported the taste to be poor or ‘worse than expected’. No subjects felt that the texture of the syrup was either poor or unacceptable.
Subjects’ opinions of effectiveness of syrup for treating symptoms of upper respiratory tract infection after 1 h (N = 56).

Subjects’ assessments of acceptability of syrup taste and texture (N = 56).

Safety
Eight subjects (14.3%) experienced treatment-emergent adverse effects (TEAEs), all of which were considered to be study drug related. In order of highest occurrence, the reported adverse effects (AEs) were somnolence (4 subjects, 7.1%), dizziness (2 subjects, 3.6%) and palpitations, dry mouth, muscular weakness, tremor and cold sweat (1 subject each, 1.8%). The AEs were all mild and transient; there were no severe or serious AEs, and no subjects discontinued the study due to an AE. Mean changes in systolic and diastolic blood pressure and body temperature were small. Mean pulse rate fell by 3.4 bpm at 1 h post-dose.
Discussion
The purpose of this study was to evaluate the perception of the warming sensation associated with a flavouring agent when combined with 500 mg paracetamol and 30 mg pseudoephedrine, per 30 mL of a syrup formulation, and its impact on the acceptability of the product for the short-term treatment of symptoms associated with URTI. This is the second documented study of perception of warming sensation associated with an OTC product used to treat symptoms of upper respiratory infections.
As in the first study, 1 the majority of the study population experienced a warming sensation after swallowing the syrup, and most described the sensation strength as ‘pleasantly warming’. In the earlier study, about 18% of subjects described the sensation as ‘not warm enough’, suggesting perhaps that warmth in an OTC medication is soothing and desirable for some patients. In this study, about 9% of subjects similarly reported the sensation as not being warm enough, with the lower number probably reflecting a greater percentage of subjects experiencing the warming sensation. The data strengthen the idea that soothing qualities of an OTC cold remedy might enhance compliance with symptomatic therapy and, specifically, support existing anecdotal evidence that for some patients suffering from URTI symptoms, warming is a positive attribute.2–5
The majority of subjects were satisfied with the syrup as a treatment for their cold symptoms at 1-h post-dosing, and most found the taste and texture to be acceptable. There were no safety concerns resulting from this study.
Like the earlier study, 1 this was done using an open-label design, and the lack of a control group – that is, the unflavoured syrup – limits interpretation of the findings. Nonetheless, it remains difficult to provide appropriate controls for these types of studies – specifically, the lack of an added flavour would likely make the syrup unpalatable for most subjects. More detailed discussion of this issue is provided in our earlier article. 1
Conclusion
This study confirms that most people perceive IFF Flavour 316282 as producing a pleasant warming sensation in an OTC cold formulation containing 500 mg paracetamol and 30 mg pseudoephedrine per 30 mL dose. There were no safety concerns, and the syrup itself was well tolerated. Overall, subjects liked the warming sensation. Data from this study and a similar earlier study suggest that the localized warming effect demonstrated by IFF Flavour 316282 may increase the acceptability of OTC products containing the flavour which may in turn improve patient compliance for those seeking relief from cold and flu symptoms.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr Judith Rosen Farrar for editorial support and technical review during manuscript preparation. Both authors participated in conducting the study, including development, data collection and analysis, writing the Clinical Study Report, and drafting the manuscript. Both authors met the International Committee of Medical Journal Editors (ICMJE) definition of authorship.
Declaration of conflicting interests
The authors are both employees of Novartis Consumer Health SA, Nyon, Switzerland.
Funding
This study was funded by Novartis Consumer Health S.A., Nyon, Switzerland.