
Abstract
Objectives:
Variation in plasma hormone levels influences the neurobiology of brain regions involved in cognition and emotion processing. Fluctuations in hormone levels across the menstrual cycle could therefore alter cognitive performance and wellbeing; reports have provided conflicting results, however. The aim of this study was to assess whether objective assessment of cognitive performance and self-reported wellbeing during the follicular and luteal phases of the menstrual cycle is feasible and investigate the possible reasons for variation in effects previously reported.
Methods:
The Cambridge Neuropsychological Test Automated Battery and Edinburgh Postnatal Depression Scale were used to assess the cognitive performance and wellbeing of 12 women. Data were analysed by self-reported and hormone-estimated phases of the menstrual cycle.
Results:
Recruitment to the study and assessment of cognition and wellbeing was without issue. Plasma hormone and peptide estimation showed substantial individual variation and suggests inaccuracy in self-reported menstrual phase estimation.
Conclusion:
Objective assessment of cognitive performance and self-assessed wellbeing across the menstrual cycle is feasible. Grouping data by hormonal profile rather by self-reported phase estimation may influence phase-mediated results. Future studies should use plasma hormone and peptide profiles to estimate cycle phase and group data for analyses.
Keywords
Introduction
The ‘normal’ menstrual cycle is initiated and progresses over 28–31 days. Plasma steroid hormone and peptide level fluctuation across phases is necessary to support the regulatory feedback mechanisms needed for normal reproductive functioning. For example, oestradiol and progesterone levels are at their lowest during menses (days 1–8), oestradiol increases over the follicular phase to peak just before ovulation. Following ovulation, oestradiol and progesterone levels both increase, peaking during the mid-luteal phase then declining towards onset of menses at Day 1. 1
Sex steroids influence neuronal plasticity, though most estimates of direct effect are derived from animal studies.2–4 Depending on concentration, oestradiol and progesterone can either protect or damage neurones.5–7 Steroid metabolism can lead to redox cycling and the formation of free radicals, leading to cell death or ischaemia. 8 The formation of the progesterone metabolite allopregnanolone modulates gamma-aminobutyric acid (GABA) and can produce a sedative effect which may slow information processing and adversely affect cognition9,10 and may also lower mood. 11
Menstrual phase–related changes in sex steroid levels can influence region-specific glucose metabolism 12 and brain activation. 13 It is therefore possible that these differences may result in altered cognitive performance similarly to effects seen in pregnancy.14,15 However, assessment of cognitive performance across the menstrual cycle has produced conflicting results.16–26 This may be due to methodological differences, but inaccuracy of self-reported menstrual cycle phase day may also influence results.
As well as affecting cognitive performance, any alteration in activation of the amygdala, a brain region involved in emotional processing, may lead to alterations in wellbeing. Premenstrual syndrome (PMS) is relatively common affecting between 40% and 90% of women. PMS occurs typically in the late luteal period when oestradiol and progesterone levels are declining prior to the onset of menses.27–30 Symptoms include mild adverse somatic and cognitive effects, mood lability, anxiety and feelings of loss of control.26,29,31 In studies investigating the association between hormone fluctuation and cognition, it is therefore important to assess emotional wellbeing as variation may adversely affect cognitive performance.31–33
It remains unclear what the effects of fluctuations in hormone and peptide levels across the menstrual cycle have on cognitive function and wellbeing, if any. The accuracy of self-reported stage of the menstrual cycle is also unclear. This investigation aims to assess study feasibility and the accuracy of self-reported menstrual cycle phase.
Materials and methods
A total of 12 women were recruited from the staff of a hospital in the north of England. Women over the age of 18, who reported they had a ‘normal’ menstrual cycle were included, that is, they had a regular monthly 28–31 day cycle. The women included were not planning a pregnancy and were not using any form of hormonal contraception. Those taking any prescription or regular non-prescription medication were excluded as were those with psychiatric or medical conditions. Study information was provided and written consent obtained.
Assessments were undertaken in the woman’s self-reported follicular and luteal phases. Self-reported stage was assessed by each woman based on the date of the start of their current menstrual period, that is, counting forwards; this was then confirmed by counting backwards from the start of their subsequent menstrual period. If there was a discrepancy (2 or more days) between phase estimation using these two methods, data were not included. Half the participants were assessed first during their self-reported follicular phase, ideally during menstruation, then 3 months later during the mid-luteal phase (group 1). The remaining participants undertook assessments first during their self-reported luteal phase and then 3 months later during the follicular phase (group 2). Figure 1 shows participant flow through the study. This cross-over design was used with the aim of precluding order and learning effects that may occur when repeated assessments are undertaken in this way. Phase of cycle was estimated first by self-report, then by plasma hormone and peptide assay. Venous blood samples were drawn at the time of each cognitive and wellbeing assessment. Approvals were obtained from the Bradford Research Ethics Committee (05/Q1202/123) and Bradford Teaching Hospitals National Health Service (NHS) Foundation Trust research department and the study was carried out according to research governance guidance. 34

Participant flow through the study.
Data collection tools
The Cambridge Neuropsychological Test Automated Battery
The Cambridge Neuropsychological Test Automated Battery (CANTAB) is a computer-based psychometric test battery, 35 providing a fast, precise, language-independent accurate and objective assessment of ability, relative to more traditional pen and paper tools.36,37 CANTAB® is designed in a game-like format, providing feedback which helps maintain motivation. 36 Four tests were chosen from the battery that assess aspects of executive function: (a) the ability to plan or strategize and (b) shift attention (stockings of Cambridge (SOC) and intra/extra dimensional (IED) shift tests) and two that assess aspects of working memory, which is a component of executive function 38 (c) immediate and delayed perceptual matching (delayed matching to sample (DMS) test) and (d) spatial memory (spatial recognition memory (SRM) test).
SRM test
The SRM test is a two-choice forced discrimination task, assessing spatial memory, completed in approximately 5 min depending on level of ability. The participant is presented with a white square, which appears in sequence at five different locations on the screen. In the recognition phase, the participant sees a series of five pairs of squares, one of which is in a place previously seen in the presentation phase. The other square is in a location not previously seen. Locations are tested in the reverse of the presentation order. This task is repeated three more times, each time with five new locations.
DMS test
The DMS test assesses forced choice recognition memory for novel non-verbalisable patterns. DMS is a test of simultaneous and DMS, assessing short-term working memory and is completed in approximately 10 min. The participant is shown a complex visual pattern (the sample) and then, following a brief delay, four similar patterns are presented. Task difficulty is manipulated by varying the delay before the 4 response stimuli are presented (0–1200 ms).
SOC test
The SOC test assesses spatial planning ability and is completed in approximately 10 min depending on level of ability. The participant is shown two displays containing three coloured balls. The displays are presented in a way where they can be perceived as stacks of coloured balls held in stockings suspended from a beam. The participant must use the balls in the lower display to copy the pattern shown in the upper display. The balls may be moved one at a time by touching the required ball, then touching the position to which it should be moved.
IED shift test
The IED shift test assesses rule acquisition and attentional set shifting ability to discriminate between patterns, to reverse a correct and reinforced response and to shift attention from one perceptual aspect of a pattern to another. The test is completed in approximately 7 min and consists of a series of two alternative forced choice patterns presented in nine fixed order stages. Two artificial dimensions are used in the test, colour-filled shapes and white lines.
Edinburgh Postnatal Depression Scale
The Edinburgh Postnatal Depression Scale (EPDS) is a valid and reliable screening tool for use in the general population. The EPDS is a 10-item self-administered questionnaire. 39 The EPDS has been used frequently as a screening tool in non-postnatal populations.40–42 Cut-off scores range from 9–13, a score equal to or greater than 11 was the cut-off indicator for increased risk of depression in this study.
National Adult Reading Test
The National Adult Reading Test (NART) can be used to assess pre-morbid IQ in those with neurodegenerative conditions such as Alzheimer’s disease, but may also be used as a quick and accurate tool to assess IQ in a healthy population. 43 The NART is relatively short and unaffected by poor concentration and motivation. Nelson 43 suggests that the NART is particularly useful in matching research participants when intelligence level may affect outcome measures.
Biochemical analysis
Selected steroid and peptide levels were used to help provide an objective measure of cycle phase day; a 9-mL venous blood sample was drawn at each test session. Following centrifugation, the sample was separated and the plasma was frozen to −80°C. Plasma hormone and peptide levels were assayed by the hospital laboratory and determined by Siemens Medical Solutions ADVIA Centaur XP® (prolactin, cortisol, oestradiol, progesterone, follicle stimulating hormone (FSH), luteinising hormone (LH) and testosterone), IMMULITE 2000 analyser (sex hormone binding globulin (SHBG)) and in-house radioimmunoassay (dehydroepiandrosterone sulphate (DHEA-S)). Coefficients of variation were provided by the laboratory: (a) prolactin 5.2% at 630 mu/L, (b) 17β-oestradiol 3.0% at 3780 pmol/L, (c) progesterone 6.4% at 50 nmol/L, (d) cortisol 7.3% at 950 nmol/L, (e) DHEA-S 11.1% at 4.8 nmol/L, (f) SHBG 5.8% at 20.1 nmol/L, (g) FSH 8.9% at 1.9 iU/L, (h) LH 7.6% at 6.7 iU/L and (i) testosterone 6.9% at 3.3 nmol/L.
Statistical analysis
Stata version 13 44 was used for all analyses. A repeated measures regression model (xtreg command) was used to analyse CANTAB and EPDS test scores (SRM – percent correct, DMS – percent correct all delays, SOC – number of problems solved in the minimum number of moves, IED shift – number of stages completed, total number of errors, number of errors adjusted by number of completed stages and EPDS – total score and number of assessments with score equal to or greater than 11). Phase of cycle and order of assessment were examined to investigate their potential influence on results. Follicular and luteal phase median and interquartile hormone and peptide level ranges were calculated and levels compared using Wilcoxon signed-rank test for matched pairs. Potential correlations between hormone and peptide levels and cognitive test scores and EPDS were explored.
Results
All women initially recruited returned for their second assessment and completed all cognitive tests, completed an EPDS and provided blood samples at each assessment. Examination of group characteristics revealed no significant differences in age, body mass index (BMI) or NART score (Table 1). The second assessment was arranged to coincide with each woman’s self-reported contrasting (relative to the first phase at testing) menstrual phase (Figure 1). Self-reported and hormone-estimated phase group cognitive test scores are shown in Table 2 and EPDS results are shown in Table 3. There were no significant differences in any test score or measure of wellbeing when results were analysed by self-reported phase, however, when results were analysed by hormone profile–estimated phase, significant phase differences were demonstrated for SRM percent correct and DMS probability error. Mean luteal phase EPDS score was significantly greater compared to the follicular phase score when results were analysed by hormone-estimated phase compared to self-reported phase (Table 3).
Participant characteristics (mean with SD in parentheses).

SD: standard deviation; BMI: body mass index (kg/m2); NART: National Adult Reading Test.
Mean (standard error) Group CANTAB Test scores by self-reported menstrual phase and hormone profile–estimated menstrual phase.

CANTAB: Cambridge Neuropsychological Test Automated Battery; SRM: spatial recognition memory; DMS: delayed matching to sample; SOC: stockings of Cambridge; IED: intra/extra dimensional.
All participants completed the maximum nine stages for each test phase.
Mean (standard error) EPDS and number classified as distressed (EPDS >11) by self-reported menstrual phase and hormone profile–estimated menstrual phase.

EPDS: Edinburgh Postnatal Depression Scale.
Phase of cycle and order of assessment effects were investigated, and no significant differences were observed for the majority of tests. For the DMS simultaneous and all delays tests, however, the group assessed first in the follicular then luteal phase (group 1) had significantly lower scores on both tests compared to the group tested first in the luteal then follicular phase (group 2) (p = 0.03 and p = 0.03). Further analysis suggests, however, that there was no carry-over/interaction effect between phase of cycle and order of assessment.
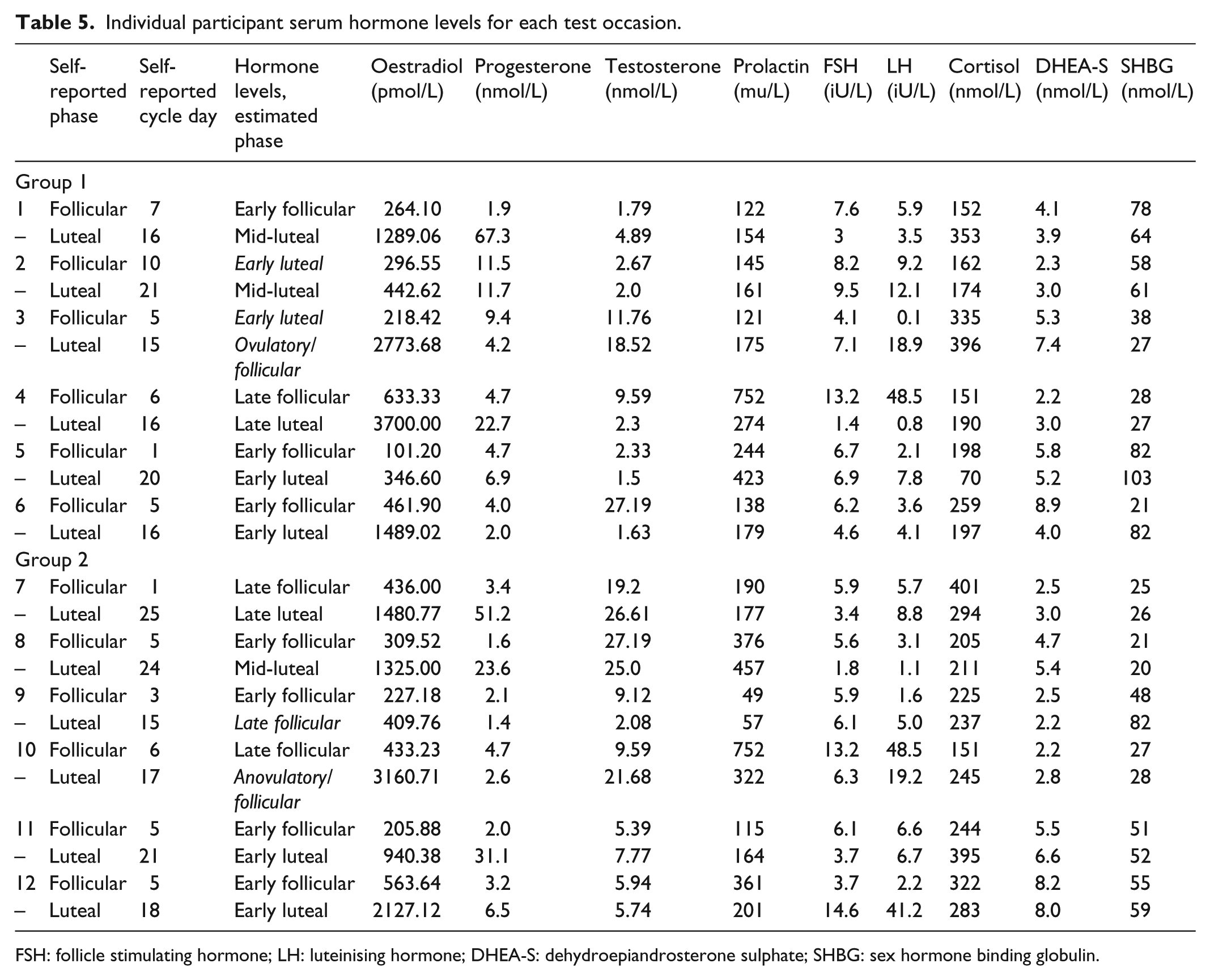
Table 4 illustrates median and interquartile range (IQR) hormone and peptide levels for the follicular and luteal phases by self-reported phase, and Table 5 illustrates individual steroid/peptide levels and self-reported cycle day and hormone-estimated phase for each participant at each assessment.
Serum hormone levels by menstrual phase.

IQR: interquartile range; DHEA-S: dehydroepiandrosterone sulphate; SHBG: sex hormone binding globulin; FSH: follicle stimulating hormone; LH: luteinising hormone.
Individual participant serum hormone levels for each test occasion.
FSH: follicle stimulating hormone; LH: luteinising hormone; DHEA-S: dehydroepiandrosterone sulphate; SHBG: sex hormone binding globulin.
Discussion
Our study demonstrates the feasibility of objective cognitive testing using CANTAB across phases of the menstrual cycle. All women returned for repeat assessments and biochemical estimation, suggesting this study design was acceptable to them. Because this was an exploratory study using CANTAB, formal sample size calculations were not undertaken. Even so when results were analysed by hormone- and peptide-estimated phase opposed to self-reported phase, significant differences were demonstrated for the SRM and DMS tests. We investigated the possible influence of order of assessment on results and found a significant effect for the DMS all delays and simultaneous percent correct measures, subsequent analysis, however, did not demonstrate a carry-over/interaction effect between phase of cycle and order of assessment, suggesting that the former significant findings for these two measures were random errors, possibly due to the small sample size.
The examination of hormone and peptide levels in our study suggests different phases to those indicated by the self-reports of some of the participants. For example, phases were reversed for participant 3 in group 1 (Table 5). Our results suggest that fluctuation in hormone and peptide profile does influence cognitive performance and wellbeing, and therefore, it is essential that phase of cycle is objectively estimated.
The inaccurate self-reporting of cycle day by some participants in our study is critical because for some participants it led to assessment of cognitive performance at a time that did not accurately reflect the hormone/peptide levels usual for that phase of cycle; if self-reported phase only had been relied on to direct grouping for analysis, no differences would have been observed in test results.
Studies that have relied on self-reporting or have assayed few hormone and peptide levels for phase estimation risk inappropriate grouping for analysis, which is a possible explanation for the conflicting findings reported across studies. Many studies in the past have relied on counting days backwards from the predicted start date of menstruation. Counting backwards is done to improve accuracy of phase estimation because the luteal phase is less variable in length compared to the follicular phase; 19 however, non-ovulatory cycles, which are common, will provide differing hormonal profiles to ovulatory cycles. More recent studies have reported a limited selection of hormones, for example, oestradiol and progesterone levels for each cycle phase,20,45 rather than reporting a comprehensive selection of individual participant levels or the ranges of individual variation as we have done in our study.
Other hormones additional to oestradiol and progesterone fluctuate across the menstrual cycle and may influence cognition and emotion processing and will also provide information on cycle stage, therefore a range of hormones and peptides should be assayed to provide a comprehensive hormonal profile and sequential hormone and peptide profiling would be likely to provide the best estimates. We found wide individual variation in steroid and peptide levels which may influence results, though it may also be the relative difference between the nadir and peak levels that are important. A further biochemical consideration is the unbound proportion of hormone; this is the bioactive proportion not bound to proteins such as SHBG. Although knowledge of the unbound proportion is not necessary for cycle phase estimation, it may help understand individual performance differences and free oestradiol, for example, can be estimated easily by dividing oestradiol level by SHBG and multiplying by 100.
Although the inconsistency in results across studies may reflect the difficult nature of measuring complex human behaviour and the inaccurate grouping of participant data for analyses, methodological differences, including different assessment tools, timing of assessments, memory domains and sample sizes are also likely to influence results. For example, some studies report no difference in spatial or verbal performance across phases of the menstrual cycle using varying assessment tools.17–19 Some report improved spatial memory relocation test performance during the luteal phase 22 and some report improved fragmented object identification and mental rotation performance during the follicular phase.21,26
Results differ however, even when the same test is used. For example, Maki et al., 21 using a fragmented object identification test (a measure of implicit memory), reported reduced object priming ability during the follicular phase, which correlated negatively with oestradiol level, menstrual stage was estimated by counting forwards from the first day of menstruation and ‘confirmed’ by serum oestradiol and progesterone levels, if levels were not ‘different’ the participant’s data were excluded from the analyses. Conversely, Hampson et al. 20 report no phase differences using the same object priming test. The method of initial cycle stage estimation is not reported, but was confirmed by salivary oestradiol levels.
The assessment of wellbeing across phases of the menstrual cycle has provided inconsistent results.21,23,24,46 Behavioural intervention seems to influence the extent of symptoms reported, 47 suggesting that psychological as well as physiological factors influence the degree of disturbance. The use of different assessment tools may explain some of the differences reported, for example, Symonds et al. 23 report a lower ‘hedonia’ score for those in the luteal compared to the follicular phase using the University of Wales Institute of Science and Technology’s mood adjective checklist (UWIST-MACL). The detection of subtle changes in affect although interesting, may not represent a clinically relevant difference or a difference that would influence cognitive performance. Again, inaccuracy in cycle day reporting and subsequent inappropriately timed assessments or grouping of data for analyses may account for some of the inconsistencies in cycle phase associated effects observed and our study findings support this.
Conclusion
This study demonstrates that it is feasible to conduct objective assessment of cognitive performance using CANTAB across phases of the menstrual cycle. Steroid and peptide level estimation shows that women may inaccurately report cycle day, this inaccuracy may result in incorrect grouping of data for analyses and is likely to account for some of the inconsistent findings reported in the literature. We have demonstrated that analysing data by hormone-estimated phase rather than self-reported phase can affect results.
The examination of cognitive performance using CANTAB and the influence of wellbeing on these measures warrants further investigation in an adequately powered study. Studies should build an accurate picture of individual participant steroid and peptide profiles so that cognitive assessment and grouping of data for analyses can be undertaken appropriately and robust evidence generated.
Footnotes
Acknowledgements
The authors thank all the women who took part in this study.
Declaration of conflicting interests
D.F., J.N., A.S., D.T. and K.M. have no financial or non-financial interests that may be relevant to the submitted work.
Funding
All aspects of this study were jointly supported by Bradford Teaching Hospitals NHS Foundation Trust and the University of Bradford.