
Abstract
Objective:
To determine the safety and efficacy of long-term use of mizoribine by undertaking a 3-year post-marketing surveillance study.
Methods:
Subjects were all lupus nephritis patients newly treated with mizoribine between 1 October 2003 and 30 September 2005 at contracted study sites.
Results:
Mizoribine was administered to 881 lupus nephritis patients in the safety analysis set consisting of 946 patients recruited from 281 contracted study sites after satisfying the eligibility criteria. There were 301 events of adverse drug reactions that were observed in 196 (20.7%) of the 946 subjects. There were 34 events of serious adverse drug reactions in 31 patients (3.2%). No deterioration in hematological and biochemical test values was observed, but immunological testing showed significant improvements in C3, CH50, and anti-DNA antibody titers. The negative rate of proteinuria also increased over time. The median steroid dosage was 15 mg/day at the commencement of treatment, but was reduced to 10 mg/day at 12 months and 8 mg/day at 36 months.
Conclusion:
The findings of the 3-year long-term drug use surveillance study indicated that mizoribine can be used over the long term with relatively few adverse drug reactions, suggesting its suitability for use in maintenance drug therapy.
Introduction
Treatment outcomes have improved for patients with lupus nephritis (LN) in recent years, thanks to the use of novel immunosuppressants coupled with early diagnosis and treatment, the development of improved dialysis techniques for patients with reduced renal function, and proper management of steroid dosing.1–3 However, treatment outcomes remain poor among patients with end-stage renal failure, sometimes resulting in death. 4 Long-term management of LN therefore faces a number of lingering treatment issues, such as the proper monitoring of adverse drug reactions (ADRs) and minimization of the decline in renal function due to disease progression.
Bredinin® 25- and 50-mg tablets (nonproprietary name: mizoribine, MZR) became in 1990 the first drug approved in Japan for the treatment of LN. MZR is an immunosuppressant that causes relatively few ADRs 5 and is particularly effective in allowing a reduction in the dosage of concomitant steroids.
Treatment outcomes of MZR in patients with LN have previously been reported in a placebo-controlled comparative study by Homma et al. 6 and in relatively long-term follow-up studies by Yumura et al. 7 and Sugiyama. 8 However, the small patient populations and limited follow-up periods of these studies prevented them from obtaining adequate data on the long-term safety and efficacy of MZR. This study therefore sought to review the data on long-term use of MZR in patients with LN over a 3-year period by conducting post-marketing surveillance and summarizing the efficacy and safety findings.
Methods
Study population
The subjects were all LN patients newly treated with MZR between 1 October 2003 and 30 September 2005 at contracted medical institutions. This study was approved by the Study Review Board at Asahi Kasei Pharma Corporation.
Patient enrollment
When MZR treatment was initiated, each patient was enrolled in the study after the attending physician obtained the patient’s initials and recorded the medical chart number, sex, and date at commencement of treatment on a patient enrollment form, which was then promptly submitted to a medical representative of Asahi Kasei Pharma Corporation.
Follow-up period
The follow-up period was 3 years from the commencement of MZR treatment. The continuation of MZR treatment was reviewed at 1 and 2 years. Patients who were slated to undergo continued treatment were transitioned to the following year’s surveillance. When completion or discontinuation of a patient’s treatment was confirmed after collecting the first- or second-year survey forms, the surveillance was ended and information on the patient’s course of treatment was collected up to that point. However, if the patient’s treatment had been suspended (on the premise of subsequently resuming administration) when the survey form was collected, information was continuously collected without discontinuing the surveillance.
Study parameters
Drugs and concomitant therapy. Conditions of use of prior therapeutic agents (steroids, immunosuppressants), reasons for using MZR, dosage and administration of MZR during surveillance, and details of concomitant drugs and concomitant therapies were all surveyed.
Patient baseline characteristics. Surveyed patient baseline characteristics were patient initials, medical chart number, date of birth, sex, body weight, inpatient/outpatient status at the time the surveillance was initiated, systemic lupus erythematosus (SLE) onset age, LN onset age, study parameters applicable to the SLE classification criteria of the American College of Rheumatology (1982 revised criteria 1997), confirmation of LN, kidney biopsy results (1995 World Health Organization classification), comorbidities at the time the surveillance was initiated, previous medical history (PMH), history of ADRs, allergic diathesis, and pregnancy.
Laboratory test values. Information on the following test results was collected in a recordable format at baseline and every month thereafter.
Hematological tests: red blood cell (RBC) count, hemoglobin (Hb), hematocrit (Ht), white blood cell (WBC) count, and platelet count (PC); Blood biochemistry tests: total protein (TP), albumin (Alb), aspartate transaminase (AST), alanine transaminase (ALT), alkaline phosphatase (ALP), blood urea nitrogen (BUN), creatinine (Cr), uric acid (UA), and blood glucose (BG); Urine tests: urine protein (UP) (quantitative and qualitative), presence/absence of cellular casts, and urinary glucose (UG) (qualitative). Immunological tests: C3, CH50, and anti-DNA antibodies.
Adverse events. An adverse event (AE) was defined as any unfavorable or unintended sign (including an abnormal change in laboratory test values), symptom, or disease occurring after treatment with MZR. The AE name, onset date, seriousness, administration of MZR relative to AE onset, causal relationship between AE onset and MZR, causes of AE onset other than MZR, and outcomes were all surveyed. Wherever possible, AEs were followed up until they resolved or dissipated.
Patient prognosis. Prognosis was surveyed at the end of each surveillance year based on the patient’s level of social functioning (i.e. “same as that of a healthy individual,” “almost normal but less than that of a healthy individual,” “uncertain,” “minimal social rehabilitation,” and “almost always at home or in hospital”) and presence/absence of dialysis.
Statistical analysis
Classification of events listed as ADRs was performed using the Medical Dictionary for Regulatory Activities Japanese Edition version 12.1 (MedDRA/J) developed by the International Conference on Harmonisation (ICH). The incidence of ADRs was listed overall and for each event.
In patients treated with MZR for ≥1005 days, time courses of hematological, blood biochemistry, and immunological (C3, CH50, anti-DNA antibodies) test values; urinary findings; and steroid dosage were compared with those at baseline, while level of social functioning was compared for each year of surveillance. All statistical analyses were performed with SAS software, version 9.1 (SAS Institute, Inc., Cary, NC, USA).
Results
Survey forms were collected from 950 patients at the 281 contracted study medical institutions. The safety analysis set (SAS) consisted of 946 of these patients after excluding two patients lost to follow-up after enrollment and two patients who were treated with MZR prior to commencement of the surveillance (Figure 1). Of these 946 SAS patients, 881 were identified as LN patients after subtracting the 65 patients treated with MZR for other collagen diseases and were analyzed in terms of their treatment continuation rate, time course of laboratory test values, and time course of steroid dosage.

Patient disposition.
Baseline characteristics of the SAS patients are shown in Table 1. The patients were predominantly women (83.7%). The mean age of the study subjects was 38.8 years, with 13.2% of the subjects aged <20 years. The mean LN duration was 5.8 years; approximately half of the cases had occurred during the past 5 years, with 245 cases within the past 1 year (25.9%) and 245 cases during the past 1–5 years (25.9%).
Patient baseline characteristics.

LN: lupus nephritis; WHO: World Health Organization; PMH: previous medical history; ADR: adverse drug reaction; MZR: mizoribine; ISN/RPS: International Society of Nephrology/Renal Pathology Society; SD: standard deviation.
Mean ± SD (minimum–maximum).
Includes 65 non-LN patients treated with MZR.
Breakdown of 14 “other” patients: classes II + III: 1 patient; classes II + V: 3 patients; classes III + V: 4 patients; classes IV + V: 6 patients.
The most common nephritis symptom was persistent proteinuria, lasting ≥4 weeks, which was observed in 740 patients (78.2%). The histological classification of renal biopsy specimens was class IV in 219 patients (23.2%) and class V in 126 patients (13.3%).
The most common reason for starting MZR therapy was to adjust (i.e. reduce) steroid and immunosuppressant use in 508 patients (53.7%), followed by inadequate efficacy of maintenance therapy that had consisted solely of steroids or immunosuppressants in 490 patients (51.8%).
The number of SAS patients (n = 946) continuing MZR therapy at the first-year review was 654 (69.1%); second-year survey forms were collected from 566 of these patients. The number of patients continuing MZR therapy at the second-year review was 450 (79.5%), this proportion exceeded that of the previous year. Third-year survey forms were collected from 415 of these patients. The number of patients continuing MZR therapy at the third-year review was 362 (87.2%) (Figure 1).
Lack of therapeutic response was provided as the reason for completion/discontinuation of MZR therapy in 110 patients (11.6%) at the end of the first year of surveillance. The frequency of this reason declined to 45 patients (8.0%) at the end of the second year and 22 patients (5.3%) at the end of the third year.
ADRs occurred in 20.7% of the SAS patients (n = 946), with 301 events observed in 196 patients (Table 2). The main ADRs were 33 events (3.5%) of increased UA level, 23 events (2.4%) of increased blood UA, 10 events (1.1%) of hyperuricemia, 16 events (1.7%) of herpes zoster, 16 events (1.7%) of increased alanine aminotransferase, and 16 events (1.7%) of decreased WBC count. There were nine observed events of ADRs (including abnormal test values) associated with reduced renal function, specifically, six events of increased blood creatinine and one event each of renal impairment, increased blood urea, and decreased creatinine renal clearance. In all, 34 events of serious adverse drug reactions (SADRs) were observed in 31 patients (3.2%) (data not shown). Specifically, there were 3 events of herpes zoster, 2 events each of pneumonia and decreased RBC count, and 27 events of other SADRs, and 1 event (0.1%) each of diverticulitis, endocarditis, sepsis, septic shock, tuberculous pleurisy, beta hemolytic streptococcal infection, enteritis infectious, atypical mycobacterial infection, herpes zoster oticus, anemia, pancytopenia, hyperglycemia, decreased appetite, loss of consciousness, iridocyclitis, interstitial lung disease, respiratory failure, gastroduodenal ulcer, hepatic function abnormal, rash generalized, abortion spontaneous, blood urea increase, hematocrit decrease, PC decrease, WBC count decrease, and blood ALP increase.
List of ADRs.

ADR: adverse drug reaction; SAS: safety analysis set.
Terms: ICH Medical Dictionary for Regulatory Activities Terminology, Japanese Edition (MedDRA/J).
Time to ADR onset from the start of MZR therapy was less than 30 days for 18.3% of all ADRs, but was 31–91 days for 24.3% of ADRs. In terms of ADR outcomes, 62.8% of all ADRs resolved and 23.3% were in the process of resolving. An outcome of death was observed in three patients, specifically, one event each of sepsis, beta hemolytic streptococcal infection, and respiratory failure.
ADR incidence rates were compared according to patient baseline characteristics, but no significant intergroup differences were seen for age, kidney biopsy classification, PMH, and presence or absence of allergic diathesis (Table 3). Conversely, ADR incidence was significantly higher in patients with prolonged LN duration, confirmed LN patients with reduced renal function (i.e. creatinine clearance rate (Ccr) ≤ 70 mL/min or serum creatinine (S-Cr) ≥ 1.5 mg/dL), patients with comorbidities, and patients with a history of ADRs.
Comparison of baseline characteristics of patients experiencing ADRs.

LN: lupus nephritis; WHO: World Health Organization; PMH: previous medical history; ADR: adverse drug reaction; MZR: mizoribine; ISN/RPS: International Society of Nephrology/Renal Pathology Society; a: Includes 65 non-LN patients treated with MZR; b: Breakdown of 14 “other” patients: classes II + III: 1 patient; classes II + V: 3 patients; classes III + V: 4 patients; classes IV + V: 6 patients; c: Chi-square test; d: Kruskal-Wallis test.
Table 4 shows the time course of laboratory test values of LN patients (n = 881) treated with MZR for ≥1005 days (33 months). No significant deterioration was observed in safety evaluation indices including RBC and WBC counts, S-Cr, BUN, UA, and BG. There was significant improvement in the immunological indices of C3 and CH50 (p < 0.01), and no deterioration in anti-DNA antibody titers. There was also a significant increase in the ratio of patients whose UP, which is an indicator of nephritis, became negative over the course of treatment (p < 0.001). Concomitant steroid dosage decreased significantly over time from 15 mg/day at the start of treatment to 8 mg/day at 36 months (p < 0.01) (Figure 2).
Time course of laboratory test values.
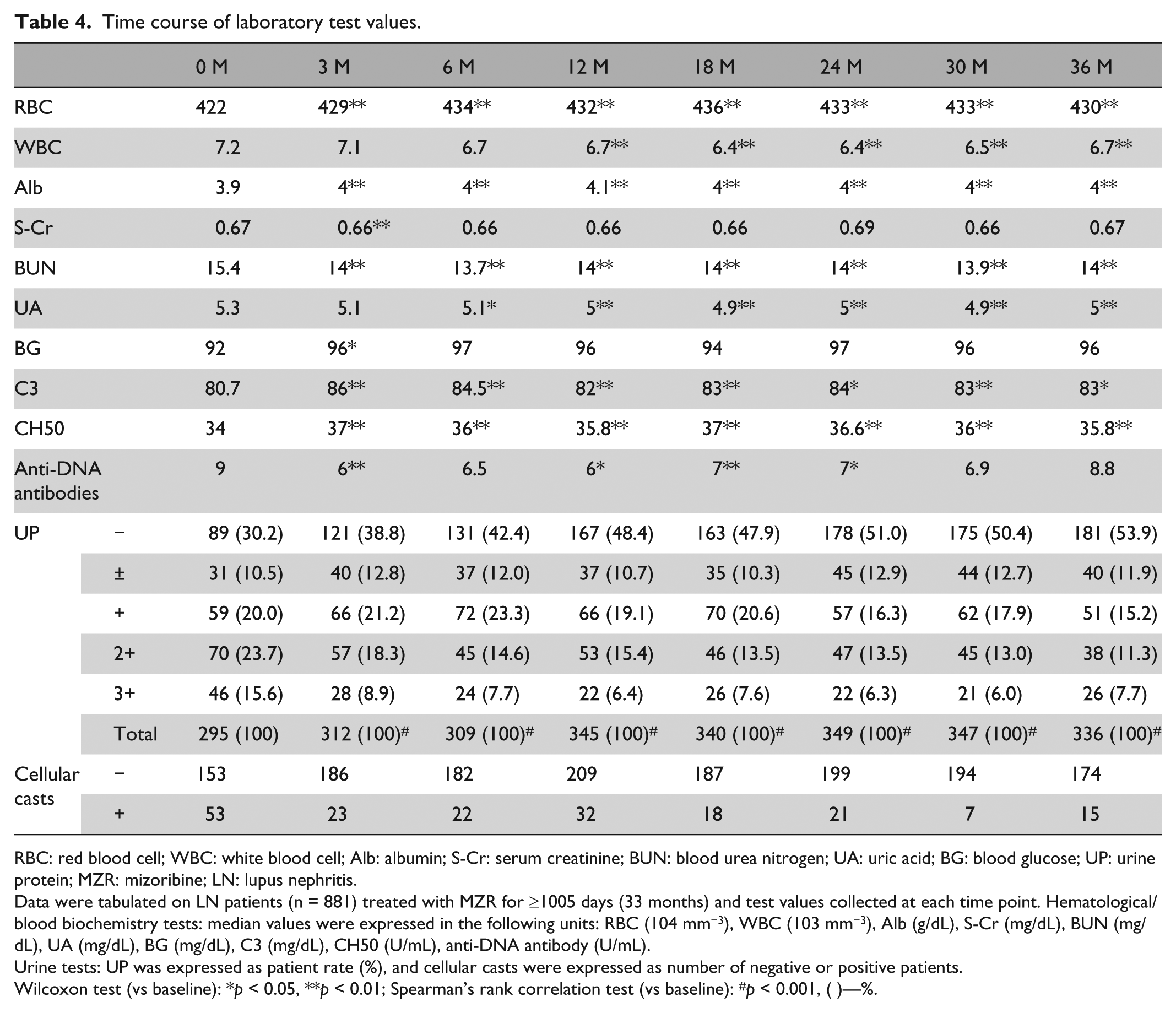
RBC: red blood cell; WBC: white blood cell; Alb: albumin; S-Cr: serum creatinine; BUN: blood urea nitrogen; UA: uric acid; BG: blood glucose; UP: urine protein; MZR: mizoribine; LN: lupus nephritis.
Data were tabulated on LN patients (n = 881) treated with MZR for ≥1005 days (33 months) and test values collected at each time point. Hematological/blood biochemistry tests: median values were expressed in the following units: RBC (104 mm−3), WBC (103 mm−3), Alb (g/dL), S-Cr (mg/dL), BUN (mg/dL), UA (mg/dL), BG (mg/dL), C3 (mg/dL), CH50 (U/mL), anti-DNA antibody (U/mL).
Urine tests: UP was expressed as patient rate (%), and cellular casts were expressed as number of negative or positive patients.
Wilcoxon test (vs baseline): *p < 0.05, **p < 0.01; Spearman’s rank correlation test (vs baseline): #p < 0.001, ( )—%.

Time course of steroid dosage.
Self-assessments of the level of social functioning at the end of the first, second, and third years of surveillance showed that the proportion of patients who responded that their level of social functioning was the “same as that of a healthy individual” increased each year from 345/881 (39.2%) to 273/552 (49.5%) and finally 219/410 (53.4%). At the same time, the number of patients who responded that they were “almost always at home or in hospital” declined annually from 30/881 (3.4%) to 10/552 (1.8%) and 2/410 (0.5%) (data not shown).
Discussion
LN is known as a factor that worsens the prognosis of SLE such that different treatments are required for new, recurring, and prolonged cases of the disease. LN treatment algorithms have been reported in the recent literature,1–3,9 with steroid and immunosuppressant usage described separately for remission induction therapy and maintenance therapy.
MZR is an immunosuppressant that was developed in Japan. It was approved for the prevention of renal transplant rejection in 1984 and for the effective and efficient treatment of LN in 1990. Its mechanism of action works by blocking inosine monophosphate dehydrogenase (IMPDH) in de novo purine biosynthesis. This is the same mechanism of action as that of mycophenolate mofetil (MMF), which has garnered high expectations as a maintenance therapy in Europe and the United States. 5
In this study, the most common reasons provided for commencing use of MZR were “to reduce steroid dosage” (53.7%) and “as a maintenance therapy in addition to current treatment” (51.8%). This suggests that MZR is used as a maintenance therapy in the same manner as MMF.
Furthermore, ADRs occurred in 20.7% of patients treated with MZR in this study, and SADRs were experienced by 3.2% of patients. The incidence of ADRs in this study is virtually the same as the 16% ADR incidence observed in the 24-week follow-up of Phase III clinical study of MZR for LN. 6
MMF has the same mechanism of action as MZR and is used widely throughout the world. However, there are no papers on MMF with a large number of LN patients like this study. There is one systematic review and meta-analysis of randomized trials and cohort studies of MMF in LN in which AE discontinuations were estimated to occur at a rate of 14% and lack of efficacy was estimated at 10% of dosed patients. In our study, serious infection occurred in 10% of patients with all infections presenting in 23.2% of patients. 10 A direct comparison of MZR and MMF can be seen for renal transplantation, with reports of incidences of infection (cytomegalovirus (CMV) and BK virus (BKV)) at 25% and 42% for MZR and MMF, respectively. 11 Thus, MZR is a safer medicine in comparison to MMF.
Hyperuricemia and increased UA levels were frequently occurring ADRs of MZR in the clinical trial and were also observed in this study at an incidence of 3.5%. However, monitoring via regular blood tests can likely prevent these ADRs from becoming serious. The incidence of ADRs was high among patients with reduced renal function (Ccr ≤ 70 mL/min or S-Cr ≥ 1.5 mg/dL) at 35.3%. This finding was previously reported by Koshikawa et al. 12 and suggests that the blood concentration of MZR, a renally excreted drug, increases when kidney function declines. The dosage of MZR therefore needs to be adjusted in response to renal function (Ccr), as indicated in the drug information for MZR. Measuring drug concentration in the blood is a useful way to monitor patients with reduced kidney function.
The treatment of LN is often protracted; therefore, reduced renal function due to long-term therapy, which is an ADR of immunosuppressants, is a matter of concern.13,14 In this study, there were nine ADRs associated with reduced renal function (including abnormal test values). On the other hand, the time course of laboratory test values of patients who underwent long-term MZR therapy did not reveal any tendency toward deterioration in S-Cr and BUN levels. Moreover, the number of patients who needed to start dialysis was 10/881 (1.1%) at the end of the first year of surveillance, 4/552 (0.7%) at the end of the second year, and 2/410 (0.5%) at the end of the third year.
MZR has been reported to have an ameliorative effect on kidney function15,16 and a protective effect on renal tissue 17 in patients with rheumatoid arthritis, immunoglobulin A nephropathy (IgAN), and primary nephrotic syndrome. MZR has also been shown not to cause renal impairment in animal-based safety testing. 5 Recent studies have attributed the renoprotective mechanism of MZR to suppression of activated macrophages 18 and increased adenosine triphosphate (ATP) synthesis in the podocytes. 19 Because LN follows a protracted course, these findings imply that MZR is a viable long-term immunosuppressant, given its effect in preserving kidney function.
Epidemiologically speaking, 90% of LN patients are women of childbearing age, 2 many of whom conceivably wish to become pregnant and give birth at some time. Accordingly, these patients must avoid therapies that adversely affect reproductive organs, particularly those with teratogenic effects on the fetus. In fact, a meta-analysis 20 of randomized controlled trials (RCTs) reported that therapy with cyclophosphamide plus steroids significantly increased the risk for ovarian failure (3 RCTs, 147 patients; relative risk: 2.18; 95% confidence interval: 1.10–4.34).
In this study, 61.8% of female patients (462/747) were of childbearing age, at 20–49 years old. The only reproductive ADRs observed in these patients were one event of menstrual disorder and one event of irregular menstruation. Pregnancy/childbirth was reported in eight patients, with no neonatal abnormalities in two patients, spontaneous abortion in three patients, and induced abortion in three patients (data not shown). MZR was found to cause teratogenicity at doses approaching the clinical dosage in an animal experiment conducted by Sasaki et al. 21 MZR should therefore be administered with care in patients who may be pregnant. However, many female LN patients may also wish to become pregnant and give birth in the future. Careful use of MZR, leveraging its low rate of gonadal suppression as an ADR compared with that of other immunosuppressants, may allow these patients to receive treatment without denying their wish to bear children.
This study investigated the efficacy of MZR in terms of reduction in steroid dosage and patient prognosis at the end of surveillance. The findings showed that steroid dosage decreased over time, with half of the patients down to 10 mg/day or less after 1 year. The ratio of patients whose reported level of social functioning was the same as that of a healthy individual also increased over time, reaching 53.4% in the third year. These findings suggest that long-term administration of MZR reduced steroid dosage and helped to improve the quality of life of long-term convalescent patients.
This study did not include any parameters for assessing LN activity; therefore, further detailed study is required. Specifically, future studies should attempt to investigate the role of MZR based on assessments using disease activity indices and remission criteria, such as the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) 22 and the British Isles Lupus Assessment Group (BILAG) Index, 23 to allow comparison of other drugs and activity assessments.
Several recent studies have also reported on MZR treatment outcomes in pediatric LN patients.24–27 MZR is used in children because of its low incidence of ADRs, its minimal gonadal suppressive effect, and the consequent effect of reducing concomitant steroid dosage in adults. Detailed analysis is needed in the future to determine whether MZR also has these advantages in children.
In conclusion, the findings of this 3-year drug use surveillance study demonstrated that MZR is a drug that can be used over the long term with relatively few ADRs, suggesting its suitability for use in maintenance drug therapy.
Footnotes
Acknowledgements
The authors would like to thank the physicians in the rheumatology and nephrology departments at the participating medical institutions all over Japan for their cooperation in this study. Additionally, we would like to thank the members of the Bredinin Lupus Nephritis PMS Expert Committee for their advice on the study analysis.
Declaration of conflicting interests
All authors are employees of Asahi Kasei Pharma Corporation, Tokyo, Japan.
Funding
This study was funded by Asahi Kasei Pharma Corporation, Tokyo, Japan.