
Abstract
Objective:
We compared a three-drug combination therapy (control group) consisting of tacrolimus, mycophenolate mofetil, and corticosteroids in living donor renal transplantation with a four-drug combination therapy (study group), in which the doses of tacrolimus and mycophenolate mofetil were halved and the immunosuppressive drug mizoribine was added, in order to determine whether the incidence rates of acute rejection after transplantation between the study group and the control group are similar, whether the study group regimen prevents the occurrence of calcineurin inhibitor–induced renal damage, and whether the study group regimen prevents adverse effects such as diarrhea caused by mycophenolate mofetil.
Methods:
We investigated the incidence of acute rejection, serum creatinine levels, and estimated glomerular filtration rate and the incidence of adverse effects such as diarrhea.
Results:
There was no significant difference between the two groups in the incidence of acute rejection. Renal function (estimated glomerular filtration rate and serum creatinine) was maintained in the control group whereas in the study group renal function gradually improved, with a statistical difference observed at 12 months. The incidence of gastrointestinal symptoms including diarrhea was significantly higher in the control group than in the study group. There was no significant difference in the incidence of cytomegalovirus infection and other adverse effects.
Conclusion:
These results suggest the study group therapy is an effective regimen in preventing acute rejection and the deterioration of renal function. These results also show this therapy can reduce the incidence of adverse effects such as gastrointestinal symptoms.
Keywords
Introduction
The renal transplantation center of Henan Provincial People’s Hospital performs about 40 ABO compatible living donor renal transplants per year. ABO incompatible living donor renal transplants are not permitted by the Chinese government. The drug regimen used for such renal transplants is a three-drug combination therapy consisting of tacrolimus as the calcineurin inhibitor (CNI), mycophenolate mofetil (MMF) as the immunosuppressive drug, and corticosteroids. Tacrolimus is an effective drug widely used for the suppression of acute rejection in renal transplantation in China. However, as a CNI, its typical adverse effects include hypertension, hyperglycemia, and nephrotoxicity, with renal damage being an adverse effect that requires particular attention.1–4
MMF is an immunosuppressive drug widely used in China that is effective for the suppression of renal transplant rejection. However, gastrointestinal disorders (including diarrhea) and infections are common adverse effects with high rates of incidence.5–9
Mizoribine (MZR) is an immunosuppressant developed in Japan that inhibits DNA synthesis by selectively inhibiting inosine monophosphate dehydrogenase in the de novo pathway.10–12 The mechanism of action of MZR is similar to MMF and is used for the suppression of acute rejection in renal transplantation instead of MMF. However, MZR is known to possess antiviral activity against cytomegalovirus (CMV) and hepatitis C virus (HCV) and has few significant adverse effects such as infections.13–17
Suppression of nephrotoxicity, which is presumably caused by CNIs, is considered to be an important factor for the long-term engraftment of transplanted kidneys. We also have experienced difficulties with refractory diarrhea and infections during treatment with MMF.
In this study, we thought that a decrease in the doses of tacrolimus and MMF would prevent deterioration of renal function caused by CNIs and reduce the incidence of adverse effects such as gastrointestinal symptoms caused by MMF. However, we were concerned about a decline in immunosuppression, so we added MZR, which has a mechanism of action similar to MMF and few significant adverse effects. We examined whether this new protocol could reduce the problematic adverse effects of tacrolimus and MMF while preserving their efficacy, to become, at least in China, a useful treatment method for living donor renal transplantation.
Methods
Trial design and participants
This study was a randomized, controlled, open-label, parallel group, single-site clinical trial. A total of 60 patients were screened for this study, with 56 patients finally enrolled and randomized in a parallel group design between a four-drug combination therapy group (study group) and a three-drug combination therapy group (control group) at the renal transplantation center of Henan Provincial People’s Hospital (Figure 1). If the medical chart number of a patient to be enrolled in the study was odd, the patient was allocated to the study group. If the chart number was even, the patient was allocated to the control group. Patients were enrolled by the lead author. All patients included in this study had undergone an ABO-identical or compatible living donor renal transplantation. Study patients ranged in age from 17 to 60 years. Patients with serious infections or cardiac diseases, women who were pregnant or seeking to become pregnant during the study period, and patients with white blood cell counts of <3000/mm3 were excluded from the study. This study was conducted according to the Declaration of Helsinki. A review of the protocol was conducted by the hospital institutional review board (2011 Henan Provincial People’s Hospital IRB Approval No. 19), and written informed consent was obtained from all the patients who participated in this study.
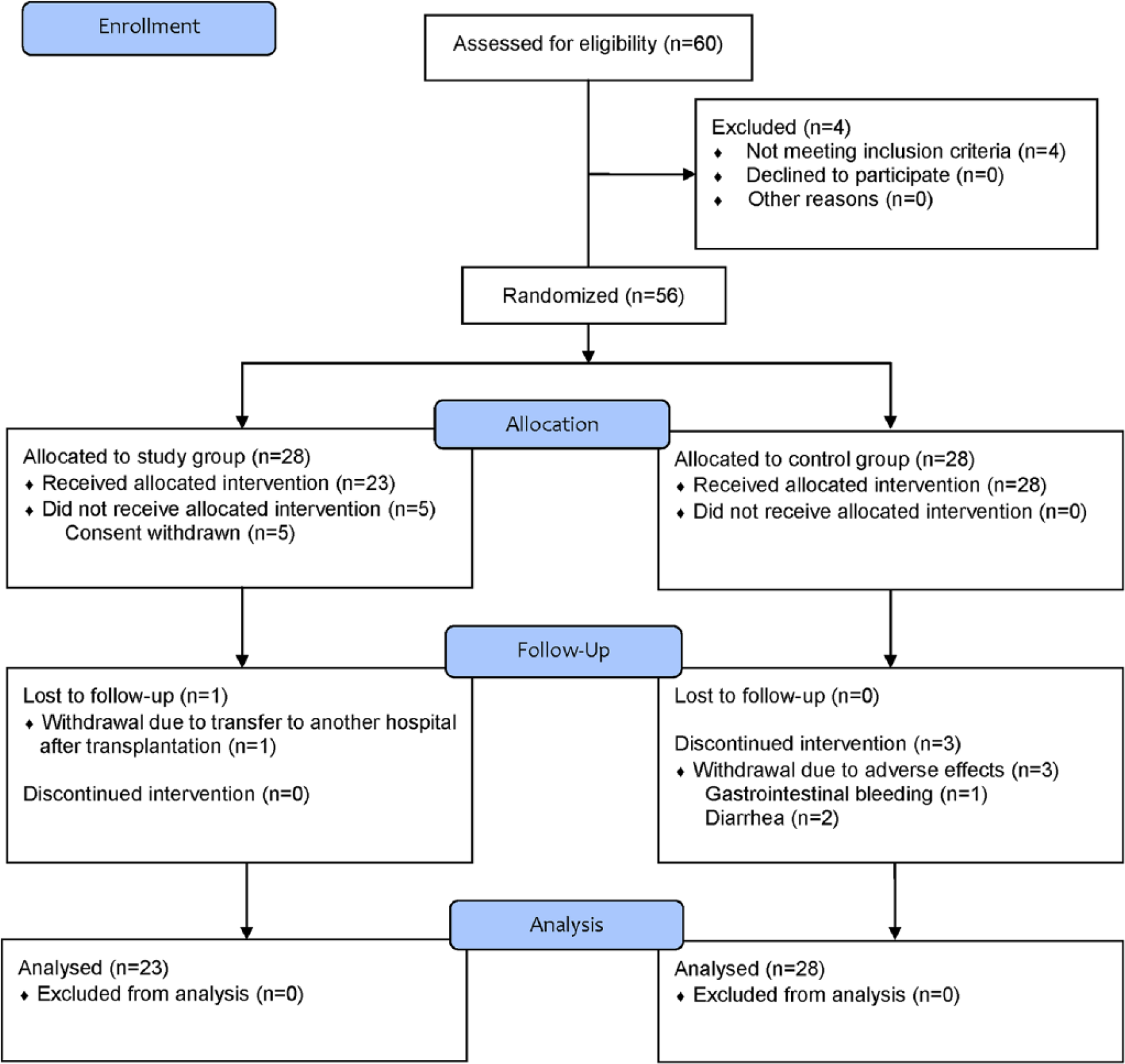
CONSORT 2010 flow diagram for this study.
Immunosuppressive protocols
The corticosteroid therapy in the control group and the study group was the same, with methylprednisolone 800 mg administered by intravenous infusion, followed by prednisone starting at 40–50 mg, the dose of which was tapered by 5 mg every 2 weeks. After 3 months, the prednisone dose was reduced to 10 mg, and this was further reduced to 5 mg while observing the patient’s condition and maintained until 12 months. Tacrolimus in the control group was started at a dose of 0.1 mg/kg after transplantation and adjusted to reach target trough levels of 8–10 ng/mL after 1 week. This was adjusted to 6–8 ng/mL from 3 months after the transplantation and then further reduced and maintained at 5–7 ng/mL by 12 months. Tacrolimus in the study group was also started at a dose of 0.1 mg/kg after transplantation and adjusted to reach target trough levels of 5–7 ng/mL after 1 week. This was adjusted to 3–5 ng/mL from 3 months after transplantation and maintained at the same level until 12 months. The dose of MMF in the control group was started at 750–1000 mg twice daily, and after 3 months was maintained at 750 mg twice daily until 6 months. Afterward, it was reduced to 500–750 mg until 12 months. The dose of MMF in the study group was started at 500 mg twice daily and maintained until 6 months, after which it was reduced to 250–500 mg until 12 months.
MZR was administered at a dose of 150 mg daily (100 mg, 50 mg) in patients whose body weight was less than 50 kg and at a dose of 100 mg twice daily in patients whose body weight was more than 50 kg. MZR was maintained at the same dose until 12 months.
Study parameters
The two groups showed no significant differences in patient background characteristics, such as underlying age, gender, dialysis period, disease in recipient, and number of human leukocyte antigen (HLA) mismatches (Table 1). At each follow-up visit (monthly for 12 months after enrollment), serum creatinine and trough levels of tacrolimus were determined by a biochemistry laboratory in our hospital. Estimated glomerular filtration rate (estimated GFR) was calculated using a version of the modification of diet in renal disease (MDRD) formula as follows: GFR (mL/min/1.73 m2) = 186 × (serum creatinine)−1.154 × (age)−0.203 × 0.742 (if female). 18 Acute rejection was judged according to the Banff classification (1997) after conducting a renal biopsy.
Patient characteristics in this study.

SD: standard deviation; HLA: human leukocyte antigen.
Endpoints
This study was an exploratory study designed to evaluate, as a drug regimen following renal transplantation, the incidence of acute rejection 1 year between the study group and the control group, whether the four-drug combination therapy prevents the occurrence of CNI-induced renal damage, and whether the four-drug combination therapy prevents gastrointestinal symptoms (in particular, diarrhea) caused by MMF.
Sample size
Among the three endpoints (i.e. the incidence of acute rejection, the occurrence of CNI-induced renal damage, and gastrointestinal symptoms (in particular, diarrhea)), the incidence of diarrhea was the primary focus for which the sample size was set. The previously reported incidence rates of diarrhea caused by MMF were 32.1%, 31.5%, and 31.4%.5,6,9 In direct comparisons of MZR with MMF, diarrhea incidence rates were not reported, but Y. Kawasaki reported a diarrhea incidence rate of 0.22% among 916 renal transplant cases treated with MZR. 17 From these reports, we estimated that a sample group of approximately 23 subjects would be needed to reach a level of significance of 0.05 and a power of 0.8 using Fisher’s exact test. Taking into account a subject attrition rate of 10%, we set the target number of subjects for this study to 60 patients.
Statistical analyses
The data are presented as mean ± standard deviation (SD) or percentages. Statistical analyses were performed with IBM SPSS Statistics (Version 19.0, Armonk, NY, USA). Nominal data were compared using the chi-square test or Fisher’s exact test, and numeric means were compared using the unpaired t test. For serum creatinine levels and estimated GFR, repeated-measures analysis of variance (ANOVA) with Bonferroni corrections was used. All tests were two-sided, and a p value <0.05 was considered statistically significant.
Results
A total of 56 patients were enrolled and randomized between January 2012 and July 2013, with 28 patients allocated to the three-drug combination group (control group) and 28 patients allocated to the four-drug combination group (study group). The follow-up period was 1 year post-transplantation. Five patients allocated to the study group withheld consent, and one patient in the study group was lost to follow-up because the patient relocated 4 months post-transplantation to another city. One patient in the control group was lost to follow-up due to gastrointestinal bleeding (stomach ulcer) (at 6 months post-transplantation) and two patients due to diarrhea (at 8 and 9 months post-transplantation) (Figure 1).
Baseline characteristics were similar between the two groups. Main indicators for transplantation were chronic glomerulonephritis and focal glomerulosclerosis in the majority of cases, with no difference between the two groups. The donor type was a parent (mother or father) in most cases in both groups (Table 1).
Steroids and MMF were administered according to the protocol for each group. Target trough levels of tacrolimus were adjusted according to the protocol for each group (Figure 2).

Comparison of profiles of tacrolimus trough levels between the two groups.
At 1 year after transplantation, patient and graft survival rates were 100% in both groups. The results of biopsy for identification of acute rejection are shown in Table 2. The incidence of acute rejection was 4.3% in the study group and 7.1% in the control group, and there was no significant difference between the two groups (p = 1.000). Biopsy examination of the acute rejections revealed one patient with Banff grade 1A in the study group and one patient with Banff grade 1A and another with Banff grade 1B in the control group. Methylprednisolone was administered at a dose of 500 mg intravenously for three consecutive days in two patients as treatment for graft rejection. Anti-thymocyte globulin was administered at a dose of 1.5 mg/kg intravenously for seven consecutive days in one patient as treatment for graft rejection (Table 2).
Acute rejection in this study.

MP: methylprednisolone; ATG: anti-thymocyte globulin.
When serum creatinine levels were compared between the two groups, no difference was found at baseline (0.5 month post-transplantation, Figure 3). While serum creatinine levels did not change for 12 months in the control group, they gradually decreased in the study group, and at 12 months a significant difference was found between the two groups (p = 0.011, Figure 3). Similarly, the estimated GFR (MDRD formula) did not change in the control group while it gradually increased in the study group, and at 12 months a significant difference was found between the two groups (p = 0.005, Figure 4).

Comparison of serum creatinine levels between the two groups.

Comparison of estimated GFR between the two groups.
Adverse effect results are summarized in Table 3. CMV infection occurred in one patient in the study group (4.3%) and six patients in the control group (21.4%); however, there was no significant difference between the two groups (p = 0.112). Gastrointestinal disorders occurred in eight patients (28.6%) in the control group and in one patient (4.3%) in the study group, with a significant difference found between the two groups (p = 0.031, Table 3). Moreover, intravenous infusion of a proton pump inhibitor was given to one patient in the control group due to the development of gastrointestinal bleeding (stomach ulcer). While hyperuricemia presented in eight patients in the study group (34.8%) and four patients in the control group (14.3%), there was no significant difference between the two groups (p = 0.166). One patient in the study group presented with a serum uric acid level of 783 µmoL/L and one patient in the control group presented with a level of 639 µmoL/L. However, all patients with hyperuricemia were managed with a combined treatment of sodium hydrogen carbonate and allopurinol. The degree of hyperuricemia was similar between the two groups with the serum uric acid mean ± SD of study group and the control group, respectively, 575.8 ± 100.1 and 556.5 ± 75.3 µmoL/L (p = 0.743) (Table 3). Patients with hyperuricemia were managed with a combined treatment of sodium hydrogen carbonate and allopurinol. There was no significant difference in the incidence rates of other adverse effects (urinary tract infections, pneumonia, leukopenia, anemia, and alanine aminotransferase increased).
Adverse effects in this study.

CMV: cytomegalovirus; ALT: alanine aminotransferase; SD: standard deviation.
Discussion
Five patients allocated to the study group (four-drug combination therapy) withheld consent due to concerns over being allocated to the study group regimen in which the doses of tacrolimus and MMF were half of that of conventional treatment and MZR was added. Three patients withdrew from the control group (three-drug combination therapy) due to adverse events, but no patient in the study group withdrew due to adverse events. One patient from the study group left the study due to a transfer to another hospital for a non-medical reason (Figure 1).
The results showed that there was no difference in the rates of rejection between the two groups, and satisfactory outcomes were also achieved with the study group, in which the doses of tacrolimus and MMF were reduced by half and MZR was added to the regimen. These results suggest that the reduced immunosuppressive effects of tacrolimus and MMF were compensated for by MZR.
When graft function was compared, serum creatinine and estimated GFR (MDRD formula) did not change after 1 year in the control group whereas these parameters gradually improved in the study group, with a significant difference observed between the two groups in serum creatinine and estimated GFR after 12 months. These results suggest that graft function in the control group was maintained because the follow-up period was short. We believe that renal function improved in the study group because of the lower dose (trough level) of tacrolimus in the study group compared to the control group.
CNIs are powerful immunosuppressants, and adequate suppression of T-cell function definitely plays an important role in the suppression of acute rejection. However, it is well known that CNIs trigger renal damage.2–4 The chronic nephrotoxicity of CNIs (CNI toxicity) is considered to be one of the reasons why mid- and long-term survival rates are not improving, and protocols based on CNI avoidance or withdrawal have been considered.19–21 Various protocols based on CNI reduction have been explored, and there has been a report where at 12 months post-transplantation the estimated GFR was higher and the occurrence of acute rejection was lower with low-dose tacrolimus than with standard-dose cyclosporine. 22 On the other hand, there is a report that CNI toxicity and the development of interstitial fibrosis (IF) and tubular atrophy (TA) without any specific etiology correlate. 23 Outside of CNI dosing, acute rejection appears to play a strong role in the development of IF/TA in that if acute rejection occurs within 1 year from renal transplantation, the rate of IF/TA presentation increases significantly at 2 years after transplantation. 24 This suggests that suppressing rejection itself is an important factor in reducing the development of IF/TA. Our results showed that a CNI dose reduction protocol may be able to prevent progress to IF/TA due to CNI nephrotoxicity better than the control group. Moreover, the fact that graft rejection was favorably suppressed in this study during the first year raises the possibility that the development of IF/TA can be halted through the suppression of rejection.
A lower incidence of CMV infection in the study group was observed when the incidence rates of adverse effects were compared, but there was no significant difference between the two groups. In China, CMV prophylactic therapy has been widely used since 2008 for CMV infection prevention in at-risk renal transplant patients. However, while CMV prophylactic therapy can reduce the incidence rates of CMV infection when compared with preemptive therapy, it is now well-recognized that late-onset CMV infection can develop when the administration of ganciclovir is ceased.25,26 In this study, we expected the incidence of CMV infection in the two groups to be similar since the same prophylactic antiviral therapy was administered in both groups. However, we did note a CMV infection incidence rate that was slightly higher in the control group, though insignificantly, than in the study group (p = 0.112). MZR is known to possess antiviral activity against CMV in experimental studies.13,14 Other clinical reports have demonstrated a significantly lower incidence rate of CMV infection with MZR compared to MMF.15,27 Furthermore, MZR can reduce the dose of ganciclovir administered due to a mutually potentiating effect between MZR and ganciclovir. 14 These reports may explain why the rate of incidence of CMV infection may have possibly have been lower in the study group.
The incidence of gastrointestinal disorders was 28.6% in the control group and 4.3% in the study group, with a significant difference found between the two groups (p = 0.031). The incidence rate, however, of diarrhea in the control group was 17.9% and lower than the previous MMF reports that were used to determine the sample size of this study. The lower incidence rate may have been due to insufficient questioning by study investigators or patients may have had a lower level of awareness regarding any manifestation of diarrhea. Furthermore, the incidence rates of diarrhea reported with MMF may have been increased due to the use of questionnaires like the Gastrointestinal Symptom Rating Scale (GSRS). 28 Diarrhea not only lowers the quality of life of transplant patients, but it can also decrease the absorption of immunosuppressive drugs from the digestive tract and possibly trigger graft rejection, and its prevention is therefore important. The development of diarrhea is a well-known and important adverse effect of MMF and has been reported to occur at a higher incidence than with MZR.15,27 In our study, serious gastrointestinal bleeding occurred in one patient in the control group. Adequate management is necessary when using MMF.
Hyperuricemia occurred at a rate of 34.8% in the study group and 14.3% in the control group; however, there was no significant difference between the two groups (p = 0.166). Since hyperuricemia may be a cause of renal damage, lower the survival rate of the kidney, and be a cause of CNI toxicity and the development of IF/TA, attention is required. It has been reported that the incidence of hyperuricemia is higher with MZR than with MMF.15,27 Similar results were observed in this study with a slightly higher incidence of hyperuricemia in the study group. However, there are also reports that there is no difference in the incidence of hyperuricemia between MZR and MMF.29,30 With respect to degree of hyperuricemia, one patient in the study group had a serum uric acid level of 783 µmoL/L, but the serum uric acid levels of this patient were elevated prior to transplantation and further increased up to the fourth day post-transplantation. Thus, the serum uric acid levels of this patient may have increased due to unstable renal function.
The mechanism of action of MZR is similar to MMF in that it inhibits DNA synthesis by selectively inhibiting inosine monophosphate dehydrogenase in the de novo pathway.10–12,31,32 However, why the incidence of hyperuricemia is higher with MZR than MMF is largely unknown. Unlike MMF, MZR is excreted in urine and this difference in excretion mechanism gives rise to hyperuricemia, but since gradual lowering of uric acid can be managed through the concomitant use of sodium hydrogen carbonate and allopurinol, adequate management is therefore considered to be possible.
This study had a number of limitations. First, this study was an open-label study subject to bias since patients could elect to withhold consent if allocated to the study group. As described earlier, only patients allocated to the study group withheld consent due to concerns over the study group regimen. Second, as this study was conducted at a single hospital in a mid-sized city in Central China, bias may be present in patient characteristics. Third, the study sample size was small, and the study duration was short. Due to these limitations, further long-term studies with longer follow-up periods and larger numbers of patients drawn from a more diverse patient population are needed to assess any long-term benefits of the study group regimen to transplant patients.
In conclusion, the four-drug combination therapy (study group) tested in this study reduced nephrotoxicity using a lower CNI dose and suppressed acute graft rejection as well as the control group. Furthermore, since gastrointestinal disorders due to MMF could also be reduced, the study group regimen can be considered a recommended protocol. Moreover, in China, we reduce the amount of drugs used and focus on preventing the occurrence of adverse effects because the physique of Chinese patients is comparatively smaller than Europeans and Americans. Given the foregoing, the study group regimen could at least be satisfactorily adopted for use in China.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from the 2011 Henan Provincial People’s Hospital Institutional Review Board (Approval No. 19).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.