
Abstract
Introduction:
Data on specific abdominal surgery and Cushing’s syndrome are infrequent and are usually included in the adrenalectomy reports. Current literature suggests the feasibility and reproducibility of the surgical adrenalectomies for patients diagnosed with non-functioning tumours and functioning adrenal tumours including pheochromocytoma, Conn’s syndrome and Cushing’s syndrome.
Discussion:
Medical treatment for Cushing’s syndrome is feasible but follow-up or clinical situations force the patient to undergo a surgical procedure. Laparoscopic surgery has become a gold standard nowadays in a broad spectrum of pathologies. Laparoscopic adrenalectomies are also standard procedures nowadays. However, despite the different characteristics and clinical disorders related to the laparoscopically removed adrenal tumours, the intraoperative and postoperative outcomes do not significantly differ in most cases between the different groups of patients, techniques and types of tumours. Tumour size, hormonal type and surgeon’s experience could be different factors that predict intraoperative and postoperative complications. Transabdominal and retroperitoneal approaches can be considered. Outcomes for Cushing’s syndrome do not differ depending on the surgical approach. Novel technologies and approaches such as single-port surgery or robotic surgery have proven to be safe and feasible.
Conclusion:
Laparoscopic adrenalectomy is a safe and feasible approach to adrenal pathology, providing the patients with all the benefits of minimally invasive surgery. Single-port access and robotic surgery can be performed but more data are required to identify their correct role between the different surgical approaches. Factors such as surgeon’s experience, tumour size and optimal technique can affect the outcomes of this surgery.
Introduction
Cushing’s syndrome (CS) results from chronic levels of the hormone cortisol in the body either from endogenous or exogenous sources. Endogenous CS is a rare entity, with estimated incidence of 2.4 cases per million populations per year. 1 Traditionally, most of these cases are due to a pituitary adenoma (Cushing disease), which is thought to occur in 80%−85% of cases. Small percentage of cases include adrenocorticotropic hormone (ACTH)-dependent CS (<10%) resulting from (non-pituitary) ectopic ACTH secretion (EAS) or, more rarely, corticotropin-releasing hormone by benign or malignant neoplasias such as a neuroendocrine tumour. The remaining percentage of patients (15%−20%) has ACTH-independent CS, which is the result of either bilateral adrenocortical hyperplasia or adrenocortical tumours that secrete excessive cortisol, causing suppression of ACTH. 2
The clinical manifestations are multiple. The typical complaints of the patients are weight gain, especially in the face developing the classic ‘moon face’, supraclavicular fat pads, buffalo hump and central obesity. Other frequent signs are purple striae, acne, skin thinning, easy bruising, osteopenia, proximal muscle weakness, emotional liability, menstrual dysfunction, virilization in women and infertility 2 (Figure 1). CS shortens the expectancy of life of the patients due to cardiovascular disease, diabetes as well as hypertension (caused by cortisol, excess of sodium and water retention).1,2

Patient who underwent laparoscopic adrenalectomy presenting weight gain, supraclavicular fat pads, buffalo hump and central obesity. We can observe the classical purple striae with acne.
As for the diagnosis, a detailed clinical history, physical examination, laboratory tests and radiologic evaluation can confirm the existence of a CS as well as determine its cause.
Medical treatment is based on the administration of adrenal enzyme inhibitors, such as ketoconazole, metyrapone, mitotane or aminogluthetimide. 3 However, the blockage achieved is only transient and leads to significant potential liver toxicity. Many of these patients, however, will benefit from a surgical procedure. When considering surgery for CS, which results from an ACTH-producing tumour of the pituitary gland (Cushing’s disease), treatment may include medical inhibitors of the ACTH secretion, but also surgical removal of a small, well-defined pituitary adenoma. 3 The transsphenoidal adenomectomy surgical approach is the gold standard for the removal of these tumours. 4 The access to this area through the gums above the upper front teeth or the nose is feasible with minimally invasive surgery. 5 By using special instruments, the surgeon makes an incision which is extended through the sphenoid sinus. Thus, the endoscopic view facilitates to remove the adenoma. This type of surgery and surgical approach permanently cures CS in 60%−70% of patients. 6 In those cases where the tumour cannot be identified, hemihypophysectomy may be considered or even subtotal hypophysectomy. 7 For some other patients, for whom the previous treatments have not been successful, surgical removal of the adrenal glands should be recommended, including total excision of one or both adrenal glands. Also, patients diagnosed with non-functioning adrenal tumour (NFT) and functioning adrenal tumour (FT) including pheochromocytoma (PH), Conn’s syndrome (CO) and CS might benefit from a surgical approach. For patients with corticotropin (ACTH)-dependent CS who have experienced failed attempts to remove the pituitary or ectopic neoplasm, bilateral adrenalectomy emerges as an excellent treatment option, resulting in immediate cure of hypercortisolism-related symptoms even in those patients with disseminated, untreatable malignancy.3,8
Surgical management and factors related
It is generally accepted that the laparoscopic approach (LA) offers some advantages compared with the open approach (OA) such as shorter postoperative recovery time, less long-term morbidity, earlier return to daily activities, early return of bowel function and low rate of wound infection and hernia.2,3,9 Some authors have tried to define which should be the criteria to perform LA versus OA. Factors such as suspicious of malignancy, a large size of the tumour, morbid obesity and invasion of the surrounding structures have been described as some reasons for conversion to open surgery without a doubt. 10
In a survey conducted by the endocrine surgery section of Spanish Association of Surgeons, 11 it was found that the LA was generally the procedure chosen by 84% of the surgeons who responded to the survey. According to their results, they had a lower rate for conversion to laparotomy (6.7%), overall morbidity (8.9%), urgent re-operation (2.3%) and mortality (0.3%) as well as a length of hospital stay of 4.9 days. In addition, it was shown that laparoscopic adrenal surgery was usually performed by a small number of surgeons in endocrine surgery units in large hospitals. Various US and European articles have analysed the influence of the volume of activity on the patients’ outcome. The outcome of these procedures does not appear to depend generally on the type of hormonal secretion by the adrenal lesion. Laparoscopy offers the possibility to operate tumours responsible for incidentalomas, CO, CS or even PH.12–15
The surgeon should choose the type of procedure after a thorough preoperative study. 16 Once the approach is chosen, which in most of the cases will be laparoscopically, adrenalectomies can be performed safely. 11
LA to the adrenal gland
There are many ways to approach the adrenal gland laparoscopically, such as by a lateral transperitoneal approach, anterior transperitoneal approach, lateral retroperitoneal approach and posterior transperitoneal approach. A clear evolution has been observed during the past 20 years in the endocrinologic surgical field, especially when dealing with new approaches and technologies.
The standard LA was first reported in 1992 by Gagner et al., 17 and nowadays, it is defined as the standard of care for adrenal pathology. 3 Even when there is suspicious of malignancy or adrenal masses >7 cm, LA is considered a safe option. 9 When compared to medical therapy, laparoscopic adrenalectomy is superior in terms of tolerance, efficacy and safety. 3 The choice of approach in laparoscopic adrenalectomy is dependent upon surgeon because there have not been found any superiority in either the transperitoneal or the retroperitoneal approach. Some surgeons do prefer the retroperitoneal approach for patients who have had prior abdominal surgery. 3 In addition, the benefits of this approach are said to be a shorter operating time, reduced blood loss and reduced risk of injury to the viscera. The retroperitoneal approach uses the retroperitoneal space in order to access the gland. A bilateral adrenalectomy can be performed in this fashion by experienced surgeons with the patient in prone position without having to move the patient. 9 Nevertheless, the lateral transperitoneal approach is preferred by most of the surgeons because the working space is wider, the anatomic landmarks are clearer and the fact that lateral decubitus and the medial rotation of the viscera allow gravity to keep the viscera away from the surgical field. The transperitoneal route is a more standardised approach where the adrenal gland is reached by entering the abdominal cavity (Figure 2).

Patient’s positioning before performing a left robotic transabdominal laparoscopic adrenalectomy in a patient with CS.
The laparoscopic technique pretends to remove the gland by previously identifying, clipping and dividing the adrenal vein (right or left). Each adrenalectomy performed on each side has specific anatomical landmarks that skilled endocrine surgeon has to respect in order to perform a standard adrenalectomy. 11
Factors related to laparoscopic outcomes
In a personal review, limiting the search for reviews and systematic reviews with the keywords ‘adrenalectomy, surgery and Cushing syndrome’, 154 articles were included in the final study after performing the first search. All abstracts were reviewed and 33 articles were selected according to the information provided with reference to CS. All these studies suggest the feasibility and reproducibility of the adrenalectomies. Many of the articles showed results with patients diagnosed with NFT, FT, PH, CO syndrome and CS. However, despite the different characteristics and clinical disorders related to laparoscopically removed adrenal tumours, the intraoperative and postoperative outcomes did not significantly differ in most cases between the different groups of patients, techniques and types of tumours. Tumour size, hormonal type and surgeon’s experience could be different factors that predict intraoperative and postoperative complications. CS does not differ in terms of surgical approach compared to other types of adrenal tumours. LA for CS is highly successful for pituitary-dependent CS and most ACTH-independent adrenal causes.
Size could be an issue in non-functional tumours, where a size of an adrenal tumour (>8 cm) and/or the evidence of its local invasiveness (both primary and metastatic adrenal malignancy) are still considered in many centres to be contraindications to a LA.12,13,15–19
Many authors have suggested that outcomes after laparoscopic procedure are related to endocrine tumour secretion, size of the tumour and the patient’s age.15,20 We believe that in the case of larger tumours, the transabdominal approach should be used in order to have an early closure of the adrenal vein avoiding, for example, the life-threatening output of catecholamine.20,21 The commonest complication reported is the tissue bleeding. 22 This complication can usually be controlled surgically during LA, but conversion to open surgery can be necessary because the ongoing tissue bleeding could not allow a safe tumour dissection. Severe bleedings can occur when dealing with the inferior cava vein during removal of a right adrenal lesion. The lesion of the peritoneum can be a problem when undergoing extraperitoneal LA. An anterior approach can then be required. Surgeon’s experience with advanced laparoscopic procedures is related to outcomes, and they are comparable to the outcome of LA performed for all tumours with hormonal disorders.21,23–26 Thus, a lower rate of postoperative complications and hospital stay after adrenalectomy is found when it is performed by a surgeon and in a hospital with a high volume of surgical activity. 11 Laparoscopic adrenalectomy is currently used to treat patients for whom malignancy is not suspected, while open surgery is still considered the standard treatment approach in patients with suspect of malignancy. 27
Conversion from LA to OA ranges between 0% and 13%. 14 Bleeding is the main cause for conversion and other causes include the following: difficult dissection or detection of the adrenal tumour, opening of the peritoneum when performing extraperitoneal approach and the presence of a pneumothorax. Gumbs and Gagner did not found differences related to the hormonal type of tumour, 14 although the surgeon’s experience, the size of the tumour and the body mass index could be predictive for conversion to OA.21,24–27 The keys to successful laparoscopic adrenalectomy should be an appropriate patient selection, a clear knowledge of the anatomy, delicate tissue handling, meticulous haemostasis and experience with the technique of laparoscopic adrenalectomy. 28 Finally, patients undergoing surgery with CS have a higher predisposition to develop complications related to cicatrisation, coagulation and also related to infections. 29
New surgical technologies
Clearly, recent advances in imaging, along with developments in neurosurgery with the transsphenoidal approach and also the laparoscopic surgery, have had the greatest impact on today’s management of the complex patient with CS. All these advances include the use of new devices and approaches. New surgical approaches such as robotic or single-port access (SPA) surgery have been used in many other procedures such as appendectomy, cholecystectomy or even bariatric procedures.29–31 Adrenalectomy has also been one of the indications in which single access can be used.32–34 Last but not least, the robotic approach in selected patients with ACTH-dependent CS, such as patients with persistent Cushing’s disease after failed hypophysectomy or patients with ectopic ACTH production that may require bilateral adrenalectomy, could be used. 35
Robotic adrenal surgery
As mentioned before, a new special tool for adrenal surgery came from a continuous development of new devices, and technologies such as robotic systems (da Vinci®) and single-port robotic incision/access devices have lead to better postoperative pain control, better cosmetic result, decreased length of stay and same postoperative results. 36 Robotic surgery has proven to assess the surgical anatomy of the adrenal glands, its vascularisation and the surrounding structures, through a high-definition and magnified three-dimensional view of the operating field provided by the da Vinci surgical system (Intuitive Surgical, Sunnyvale, CA, USA) (Figures 2 and 3). This technique performed under the da Vinci Surgical system can be safer and can offer the promise of a unique combination of advantages over open and conventional LAs. However, there is still a lack of clinical data demonstrating improved outcomes for robotic surgical applications within the abdomen and also for adrenalectomy.37–39 Thus, more outcome data for surgical robotics should be given in order to elucidate the real benefit compared to the exorbitant costs associated with the use of these tools. The performance of unilateral or synchronous bilateral adrenalectomy treated using the da Vinci robot (Intuitive Surgical) has been described. 38 Although, some studies have mentioned that laparoscopic adrenalectomy is superior to robot-assisted adrenalectomy in terms of feasibility, morbidity and cost.40–42 We can conclude, and according to some of the reviewed papers, that bilateral total adrenalectomy can also provide effective palliation from hypercortisolism in patients with ectopic ACTH syndrome and for those who have failed previous transsphenoidal surgery. 43 The da Vinci technology can nowadays be applied through a single incision. 44

External view of a robotic transabdominal laparoscopic adrenalectomy in a patient with CS.
Single-site access adrenal surgery
Recently, advanced laparoscopic skills accumulated from experience and new developments in laparoscopic instruments have led to the introduction of SPA laparoscopic adrenalectomy. 43 Many authors have already reported their previous experience in SPA, with good results. This SPA technique could provide potential benefits (lesser wound pain, better cosmetic satisfaction and shorter convalescence).45,46 Left adrenalectomy is a technically feasible and safe procedure in carefully selected patients. The definitive clinical, aesthetic and functional advantages of this technique require further analysis. The approach can be challenging for bilateral lesions. Although, further studies will be required in order to define and decide the patients who are more eligible for this approach. 36 A summary of the different approaches is shown in Table 1.
Table showing the different laparoscopic approaches with their usual accesses, number of trocars, advantages and disadvantages.
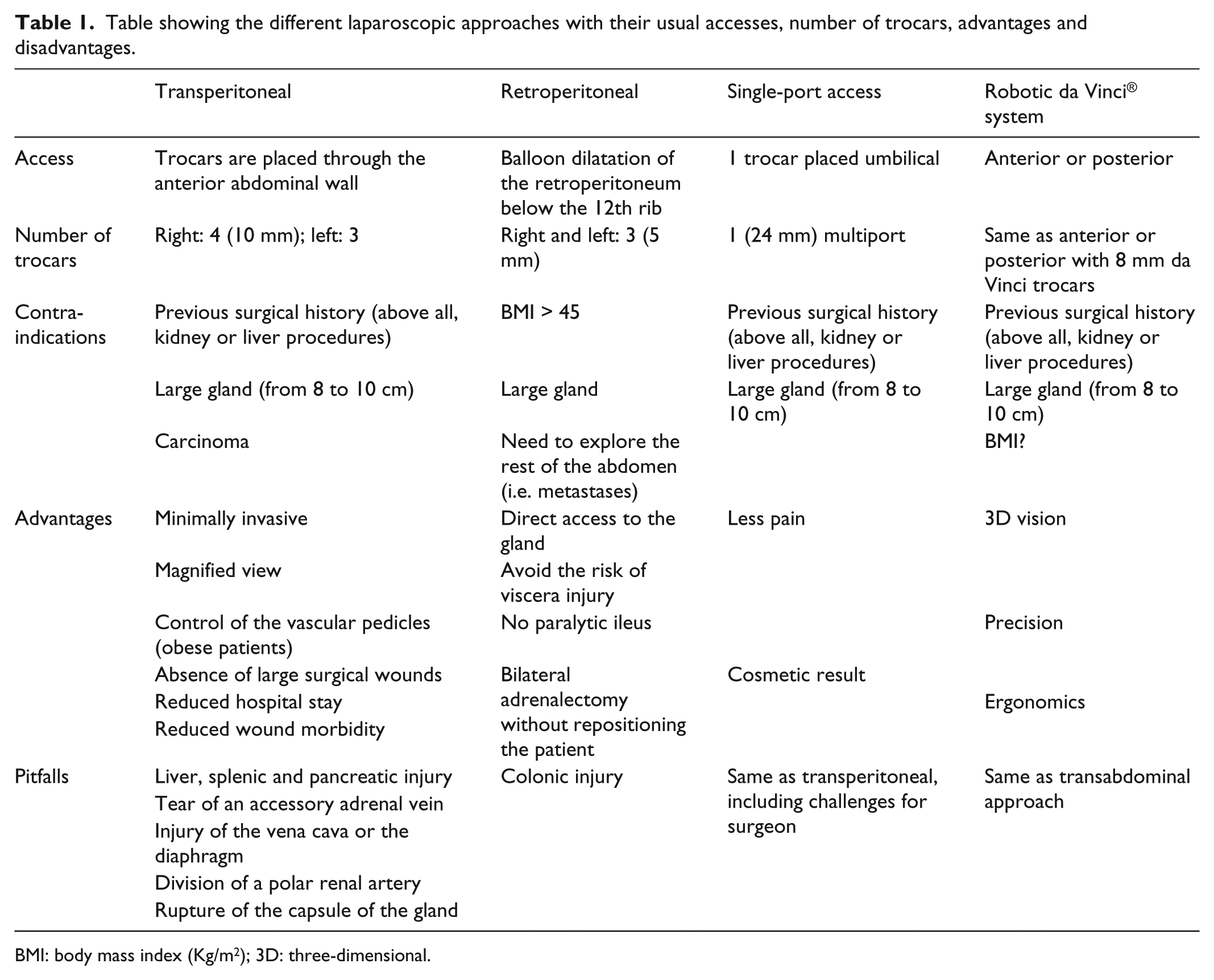
BMI: body mass index (Kg/m2); 3D: three-dimensional.
For all these above-mentioned reasons, during the past decades, surgery has become the treatment of choice for patients with endogenous CS. Adrenalectomy, in particular, is a surgical procedure performed with increasing frequency since 1980s, and over the last two decades, LA has become the surgical procedure of choice in the treatment of most benign adrenal lesions. Also, this approach is suitable for removal of both functional and non-functional tumours. Since then, as we have already mentioned, many authors have reported their experience with their results in OA and LA.
Conclusion
Laparoscopic adrenalectomy is nowadays the technique gold standard for the surgical management of CS because it allows the removal of adrenal lesions or bilateral adrenalectomy in the same act without an increase in morbidity. Moreover, surgery provides an immediate disease control. There are several studies that have shown its advantages compared with the OA such as reduced hospital stay, less postoperative pain and a decrease in transfusion requirements or wound morbidity. There are wide ranges of technical approaches, which are equally effective. As long as the surgeon has taken into account preoperatively key facts such as the size of the adrenal mass, the history of previous abdominal surgeries. Factors such as tumour size and surgeon’s experience may influence the surgical outcomes. New technologies such as robotic surgery or single-port surgery can offer new vistas for the future of adrenal surgery.
Footnotes
Declaration of conflicting interests
The authors declare that they do not have any conflict of interest.
Funding
The Dr Ramon Vilallonga Foundation has financially supported the study and helped to prepare the manuscript ( www.fundacioramonvilallonga.org ).