
Abstract
Background:
The use of fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) in the assessment of infectious diseases has been increasing, yet research on its impact during follow-up remains scarce.
Objectives:
To evaluate the impact of follow-up FDG-PET/CT on managing focal infectious diseases.
Design:
An observational, retrospective, single-center study.
Methods:
Patients who underwent FDG-PET/CT for the diagnosis of focal infection and had a follow-up FDG-PET/CT between January 1, 2012 and October 31, 2023 were included. The impact of follow-up FDG-PET/CT on management was defined as findings leading to any change in antibiotic treatment or any source control interventions (impact group), which was compared to follow-up FDG-PET/CT that did not lead to any change in management (no-impact group).
Results:
Eighty-nine patients were included, with a mean age of 62 ± 14.6 years. The most common infections were of skeletal (n = 34, 38.2%) and cardiovascular origin (n = 16, 17.9%). Overall, the follow-up FDG-PET/CT findings resulted in changing the management in 57 (64%) patients. It led to antibiotic change in 54 (60.7%) patients, and to source control intervention in 29 (32.6%) patients. Demographic and clinical characteristics of the impact group and the no-impact group were similar, except for a significantly higher rate of gram-positive bacteremia, which was detected in 26 (93%) patients with bacteremia in the impact group (mostly Staphylococcus aureus) compared to 8 (57%) of patients in the no-impact group, p = 0.01. Impact of FDG-PET/CT was associated with worsening clinical status, observed in 33 patients (57.9%) in the impact group compared to 6 (18.8%) in the no-impact group, p = 0.002.
Conclusion:
Follow-up FDG-PET/CT appears to have a significant impact on managing selected patients with focal infections, particularly those caused by gram-positive bacteremia or with an unfavorable clinical course.
Introduction
The use of fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) in the assessment of infectious diseases has been increasing in parallel with the accumulating experience and knowledge regarding its benefit for the diagnosis of various infectious conditions. 1 FDG PET/CT has been incorporated into the management guidelines of cardiac infections, such as infective endocarditis and cardiac implantable electrical device (CIED)-related infections.2,3
In addition, it has become widely used in the diagnosis of vascular graft infection (VGI) 4 and osteomyelitis. 5 Accumulating evidence has also shown the role of FDG PET/CT in specific infectious etiologies that tend to involve multiple distant sites in the body, such as Staphylococcus aureus bacteremia (SAB). 6
Few studies have shown that, in addition to its role in the initial diagnosis of infectious processes, FDG-PET/CT can also help monitor response to treatment over time.7–9 Its ability to provide both functional and anatomical information makes it an effective tool for managing these conditions and tailoring treatment according to infection activity. Yet, research on the impact of using FDG PET/CT during the follow-up of infectious diseases is lacking
The current study aimed to evaluate the impact of FDG PET/CT as a follow-up tool on the management of focal infectious diseases, and to characterize these conditions by looking for factors associated with having an impact of follow-up FDG PET/CT on management.
Methods and materials
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement, 10 as presented in the Supplemental File.
Study design and setting
This was an observational study conducted at Rambam Health Care Campus (RHCC), a university-affiliated, tertiary 1000-bed hospital. In addition to the infectious disease (ID) consultations given during hospitalization, patients with complicated infections are followed at the hospital outpatient ID clinic after discharge.
We retrospectively identified adult patients diagnosed with focal infection who underwent FDG-PET/CT at initial diagnosis (baseline FDG-PET/CT) and during follow-up (follow-up FDG-PET/CT), between January 1, 2012 and October 31, 2023.
Patient population
The RHCC electronic medical record database was searched for adult patients who had at least two FDG-PET/CT studies. Then, patients whose baseline FDG-PET/CT demonstrated a focal infection and whose second FDG-PET/CT indication was performed for follow-up of the infectious process were identified.
Patients for whom clinical follow-up data were not available were excluded. FDG-PET/CT data that were technically non-informative were also excluded. In addition, patients with chronic Q fever who underwent follow-up FDG-PET/CT periodically as part of a standardized management protocol were excluded.
Data collection
Clinical data at diagnosis and during follow-up were collected from the hospital admissions and the ID clinic charts, including demographics, comorbidities, clinical presentation, source of infection, and microbiological information such as blood or other body fluid or tissue culture and histopathological analysis of samples taken from suspected or confirmed infectious processes. In addition, laboratory measurements such as white blood cell count (WBC) at initial presentation and C-reactive protein (CRP) levels (the highest value in the week before the baseline FDG-PET/CT performance) were collected. Data regarding treatment strategies and intervention procedures were also recorded.
Outcome
The study outcome was the impact of follow-up FDG-PET/CT on patient management. Management data including antimicrobial treatment (type, route of administration, duration) and modifications following FDG-PET/CT findings were recorded for both the baseline and follow-up FDG-PET/CT scans. Data regarding intervention procedures that were performed within 2 weeks from FD-PET/CT, such as the extraction of a foreign body, drainage/debridement of an infection process, surgical excision, and/or replacement of involved sites (such as infected vascular graft, cardiac valve, or prosthetic joint), were also recorded.
The impact on the management of follow-up FDG-PET/CT was defined as any modification of either antimicrobial treatment (stopping or starting an antimicrobial agent, adding a new agent, or changing the route of administration) or intervention made based on the follow-up FDG-PET/CT results within 2 weeks.
Based on their outcome, patients were classified into two groups: the “impact group,” which included patients in whom the follow-up FDG-PET/CT led to a change in management, and the “no-impact group,” in which follow-up FDG-PET/CT did not result in any change to patient management.
Fluorodeoxyglucose-positron emission tomography/computed tomography
FDG imaging was performed using three FDG-PET/CT devices (Discovery 690, Discovery MI and Omni Legend; GE Healthcare). Images were acquired on average 1 h after intravenous injection of 0.14 mCi/kg of F18-FDG. Oral and/or intravenous contrast media were administered if not contraindicated. In suspected cardiac infection, patients were instructed to keep a free-carbohydrate, fat, and protein-enriched diet for 12 h, followed by a prolonged fasting period of 12–14 h before the FDG PET/CT scan. In cases other than suspected cardiac infection, patients fasted for at least 4 h before the FDG PET/CT scan. Blood glucose levels were measured and recorded before radiotracer administration. Patients underwent eye-to-mid-thigh FDG-PET/CT acquisition, with head and lower limb scans added when clinically indicated. For this study, the original written reports of FDG-PET/CT images generated at the time of clinical interpretation were used. The interpretation of FDG-PET/CT was based on visual assessment, where a focus was considered suspicious for infection if it demonstrated increased FDG uptake greater than that of surrounding tissues, located in an area not consistent with physiologic radiotracer distribution or known degenerative skeletal changes.
On follow-up FDG-PET/CT, improvement was defined as either complete resolution of previously demonstrated suspicious foci or a noticeable decrease in FDG uptake intensity compared to the baseline study. Conversely, worsening was defined as increased FDG uptake intensity or extent of involvement in previously identified infectious foci, and/or the appearance of new hypermetabolic lesions suspicious for infection.
Statistical analysis
Descriptive statistics in terms of mean, standard deviation, percentages, median, and ranges were presented for all study parameters. Normal distribution of continuous parameters was tested by Kolmogorov–Smirnov test. As a result of this test, we used the t-test or Mann–Whitney U test for differences between the two groups (no-impact or with impact). For categorical variables, we used Fisher’s exact test or Pearson’s chi-square test. p < 0.05 was considered statistically significant. SPSS version 28 (Armonk, NY, 2022) was used for all statistical analysis.
Results
During the study period, 123 patients with a focal infection in the baseline FDG-PET/CT who had a second FDG PET/CT were identified. Thirty-four patients were excluded because the second FDG PET/CT was performed for noninfectious indications, such as oncological assessment, or because critical clinical data were missing. Eventually, 89 patients were included for analysis in our study (see Figure 1).
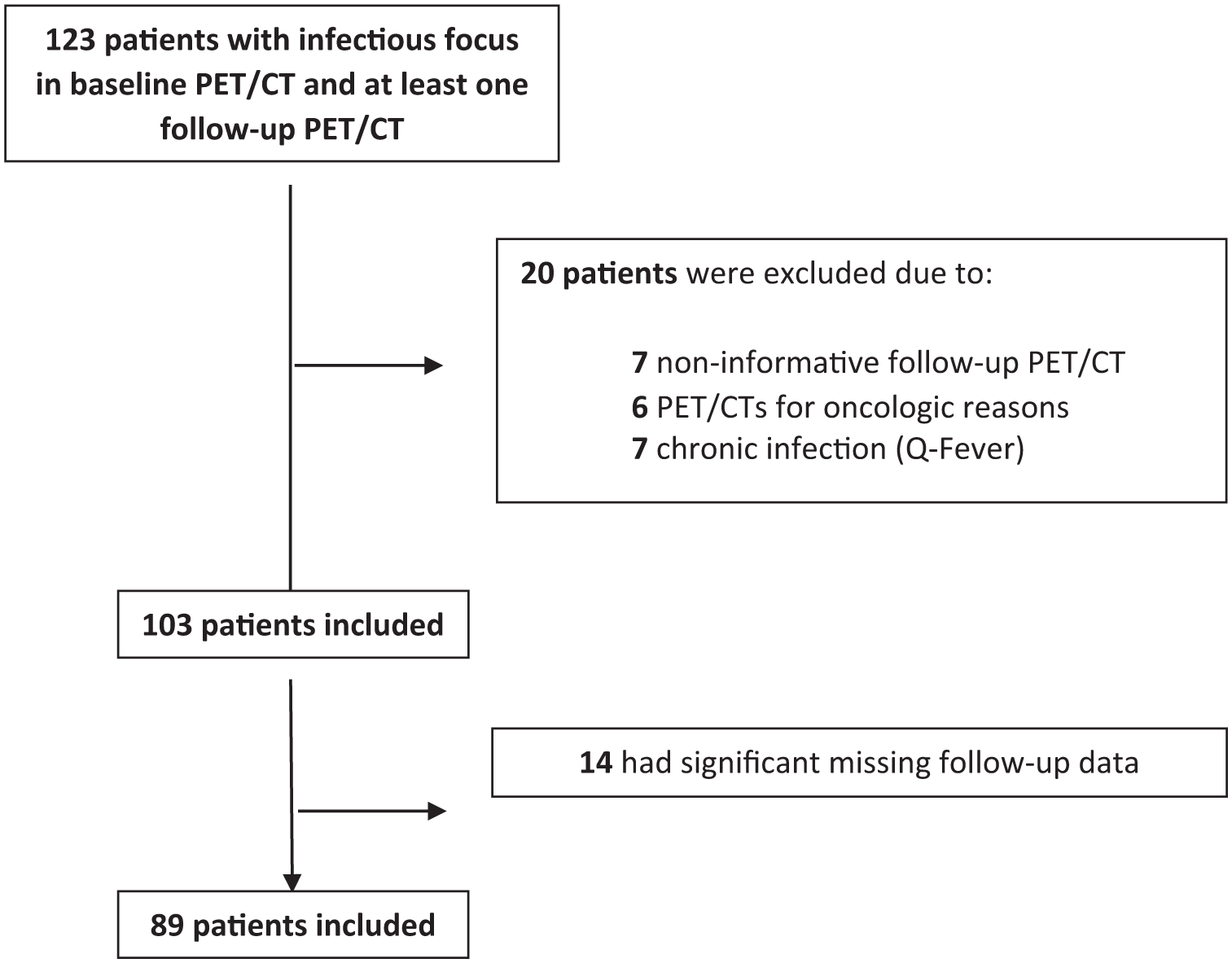
Flowchart of patients’ identification and inclusion.
Patients’ characteristics are summarized in Table 1. Mean patients’ age was 62.2 ± 14.6 years, and 59 (66.3%) were male. The study population had various underlying medical conditions (average Charlson score of 5.10 ± 3.12); 34 (38.2%) had diabetics and 20 (22.5%) had solid malignancy. At the time of the initial presentation (in which the baseline FDG-PET/CT scan was performed), 42 (47.2%) patients had bacteremia, of whom 34 (31.7%) were caused by gram-positive pathogens, of whom 27 (80%) had SAB, and 8 (9.0%) patients had gram-negative bacteremia.
Study population demographics, baseline characteristics, and initial presentation.

C-reactive protein > 0.5 mg/dl.
Lung, soft tissue, and deep-seated abscesses.
According to cultures collected from different samples such as tissue or pus drained or deep seated or blood or other sterile body fluids.
Three fungal infections, two brucella and one nontuberculous mycobacterial infections.
FDG PET/CT, fluorodeoxyglucose positron emission tomography/computed tomography; WBC, white blood cell.
Baseline FDG-PET/CT findings
Focal infections as detected by FDG PET/CT were consistent with joint and bone infections in 50 (56.2%) of patients (constituted of 23 vertebral osteomyelitis, 22 non-spinal osteomyelitis and 6 patients with septic arthritis), cardiovascular infections in 28 (31.5%) patients (17 vascular graft infections, one aortitis, and 11 infective endocarditis and one implantable cardiac device infection) and other types of focal infections in 27 (30.3%) patients in lungs, soft tissue, and deep-seated abscesses (spleen, kidney, liver, and other internal organs). More than one focus was observed in 17 (19.1%) patients (Table 1).
A causative agent was isolated in 81 cases (91%) from blood, tissue, or pus cultures. The pathogens were gram-positive in 41 (46.1%) patients, gram-negative in 20 (22.5%) and polymicrobial in 14 (15.7%). In 8 (9.0%) patients, no pathogen was identified.
For the initial focal infection diagnosis, antibiotic coverage duration was 53.85 ± 44.9 days. Antibiotics were administered intravenously in 57 patients (64.0%), orally in 18 (20.2%) and as a combination of both in 14 patients (15.7%).
Follow-up FDG PET/CT findings
Follow-up FDG-PET/CT scan was performed in a median of 90 (Q1–Q3, 50.5–169) days after the baseline FDG-PET/CT, showing no infectious foci in 32 (36%) patients, a single focus in 42 (47.2%), and more than one focus in 15 (16.8%) of patients. At the time of the follow-up FDG-PET/CT, 20 (23.5%) patients were under antibiotic coverage (Table 2).
Follow-up FDG-PET/CT.

FDG PET/CT, fluorodeoxyglucose positron emission tomography/computed tomography.
The clinical status at the time of the follow-up FDG-PET/CT was reported as improving in 40 (44.9%) patients, worsening in 39 (43.8%), and the rest 10 (11.2%) patients had no significant clinical change. When comparing the follow-up FDG-PET/CT findings with the baseline FDG-PET/CT scan, the results showed an improvement in 47 (52.9%) patients, worsening in 36 (40.4%) patients, and no change in 6 (6.7%) patients. Clinical and imaging (FDG-PET/CT) concordance was found in 63 patients (70.8%).
Overall, follow-up FDG-PET/CT findings resulted in changing the management in 57 (64.0%) patients. In 54 (60.7%) patients, it led to antibiotic change as follows: prolongation of treatment in 16 (18%), stopping treatment in 7 (7.8%), restarting antimicrobial treatment in 13 (14.6%), and adding antimicrobial agents or changing type of antimicrobial drugs in 18 (20.2%). In addition, 29 (32.6%) patients underwent source intervention after the follow-up FDG PET/CT. These interventions included orthopedic surgeries such as infected bone and soft tissue debridement, and cardiovascular surgeries for replacement of infected vascular grafts/infected valves, and procedures for extraction of an infected CIED. Two examples of cases in which the follow-up FDG-PET/CT showed dynamics that contributed to management change are presented in Figures 2 and 3.

A 18-year-old female patient with Staphylococcus aureus bacteremia (SAB), presenting with fever and anterior chest wall pain. Baseline FDG PET/CT images (a, b) demonstrate pathological FDG uptake in a left parasternal mass involving the pectoralis muscle and the sternum (arrows), consistent with an infectious process. Follow-up FDG-PET/CT images (c, d), obtained 2 months after initiation of antibiotic therapy, show significant improvement with resolution of the previously noted pathological uptake. These results were followed by discontinuation of antimicrobial treatment.

A 63-year-old male patient was admitted for an infected diabetic foot following a right hip prosthesis implantation. He was diagnosed with endocarditis secondary to nosocomial methicillin-resistant Staphylococcus aureus bacteremia. Initial FDG-PET/CT performed at the time of diagnosis did not reveal any foci of FDG uptake suspicious for infection, including cardiac structures and around the right hip prosthesis (Images a, b, c, d). The patient subsequently underwent aortic valve replacement and was treated with appropriate antibiotic therapy. Due to clinical deterioration and new-onset back pain, a follow-up FDG-PET/CT was performed within 2 months. The follow-up study (Images e, f) demonstrated a new focus of pathological FDG uptake at the D9–D10 vertebral level, localized to CT findings consistent with discitis/osteomyelitis (white arrows). Additionally, new pathological FDG uptake was shown around the right hip prosthesis and in a hypodense area along the lateral aspect of the hip (red arrows), suggestive of periprosthetic infection (Images g, h). The patient underwent several surgical interventions on both the spine and right hip. He was discharged to rehabilitation 6 months after a prolonged antimicrobial treatment.
Predictors of the impact of follow-up FDG-PET/CT on management
Comparison between the 57 patients in the impact group (follow-up FDG-PET/CT led to change in management) with the 32 patients in the no-impact group (n = 32) is presented in Table 3. The two groups were similar in their demographic and clinical characteristics, including age, gender, comorbidities, and initial clinical presentation parameters, as well as in baseline FDG-PET/CT findings, indications, number of infectious foci, location/origin of foci, intervention, and antimicrobial treatment and duration. The time interval between baseline and follow-up FDG PET/CT was 77 (55–172) days in the impact group and 177 (68–188) days in the no-impact group. This time interval difference was found to be statistically nonsignificant (p = 0.37).
Comparison between patients for whom follow-up FDG-PET/CT had impact on management to those who had not (no impact).

C-reactive protein > 0.5 mg/dl.
Lung, soft tissue, and deep-seated abscesses.
According to cultures collected from different samples such as tissue or pus drained or deep seated or blood or other sterile body fluids.
Three fungal infections, two brucella and one nontuberculous mycobacterial infections.
FDG PET/CT, fluorodeoxyglucose positron emission tomography/computed tomography; WBC, white blood cell.
Bold to highlight the statistically significant values (p < 0.05).
Although both groups were similar in terms of the presence and duration of bacteremia, a statistically significant difference was found in the type of bacteremia. Specifically, in the impact group, 26 out of 28 bacteremic patients (93%) had a gram-positive causative agent, compared to 8 out of 14 patients (57%) in the no-impact group, p = 0.01. Focusing specifically on S. aureus bacteremia, there was a trend toward a higher prevalence in the impact group (21 out of 57 patients (36.8%)) compared to the no-impact group (6 out of 32 patients (18.8%)). However, this difference did not reach statistical significance (p = 0.07).
The second significant difference between the groups was the clinical status before the follow-up FDG-PET/CT. Specifically, 33 patients (57.9%) in the impact group had a worsening clinical status compared to 6 patients (18.8%) in the no-impact group, p = 0.002.
Differences in the follow-up FDG-PET/CT findings were observed in the focus of infection with higher rates of bone and joint infections (32 (56.1%) vs 2 (6.3%), p = 0.001 and deep-seated abscesses (12 (21.1%) vs 0, p = 0.003) in the impact group and the no-impact group, respectively.
Discussion
Our study evaluated the impact of follow-up FDG-PET/CT on managing patients with focal infectious diseases. We observed that in selected cases of complicated infections, mostly of skeletal and cardiovascular involvement, a follow-up FDG-PET/CT has a very high impact on patient management, manifesting in supporting decision-making regarding antimicrobial treatment in 60% and source control decisions in 33% of the patients. The high impact of follow-up FDG-PET/CT was observed in association with the presence of gram-positive bacteremia, mostly of S. aureus bacteremia, and in accordance with worsening in clinical status. The impact of follow-up FDG-PET/CT seemed to be related to the detection of new or worsening known foci of skeletal infections and deep-seated abscesses.
Most patients in the current study were initially diagnosed with skeletal and/or cardiovascular infections, which explains the initial use of FDG PET/CT, a central tool in diagnosing these infections. 2 However, few studies have evaluated the role of FDG-PET/CT in the follow-up of such patients. In a prospective study of 25 patients diagnosed with vascular graft infection, follow-up FDG-PET/CT that was performed at an average time of 170 days from the baseline FDG-PET/CT was found to have an impact on management in all patients, affecting the treatment plan in 19 patients (76%) and leading to a different clinical approach in the rest 8 (32%) of patients due to incidental findings. 7 In another retrospective study that included 29 patients with spondylitis, a significant impact of FDG-PET/CT on clinical management was observed in 15 (52%) of patients. 8 In a single-center study, which included 133 patients with confirmed spondylitis, FDG-PET/CT use for follow-up was associated with a high rate of clinical cure rate with an odds ratio of 0.45 (0.31–0.78), p = 0.02. 9
Gram-positive bacteremia was associated with a significant impact on follow-up FDG-PET/CT results. The predominant pathogen in this group was S. aureus, being the most common pathogen causing focal infections, particularly skeletal and cardiovascular infections. The high impact of FDG-PET/CT in the management of SAB and on clinical outcomes has been demonstrated in several studies. In one prospective study, adding FDG-PET/CT as a diagnostic tool in SAB was associated with decreased mortality, by changing the duration of antibiotic treatment and leading to interventional procedures for source control. 11 Similarly, in a retrospective study, FDG PET/CT led to management modifications in 74% of 99 high-risk SAB patients. 12 In the present study, we observed that FDG-PET/CT had an important role in the management during follow-up of patients with gram-positive bacteremia, who were mostly with SAB, who were diagnosed initially with focal infection. This finding supports the fact that FDG-PET/CT can play an important role in individualizing the treatment of focal infectious diseases, as has been suggested in previous studies.6,13,14 The association between having a worsening clinical status during follow-up and having an impact on follow-up FDG-PET/CT can further guide the use of this modality in infectious disease management. The impact on patients with gram-positive bacteremia with focal infections, particularly in SAB, could be related to the tendency of this type of infection to seed multiple sites, frequently resulting in multifocal infections.11,12 Therefore, whole-body imaging showing the status of multiple foci of the infection in remote sites is potentially informative, since infection in one site might improve while worsening in other sites, necessitating repeated therapeutic interventions. It also helps in detecting new sites of infection that might have been missed, or even did not exist, in the initial FDG-PET/CT. This assumption of different sites of infection detected over time is further supported by our study results showing a statistically significantly higher rate of skeletal infections and deep-seated abscesses in the impact versus no impact groups, which was observed in the follow-up FDG-PET/CT but not in the initial FDG-PET/CT.
In the present study, we could not establish the optimal suggested time interval for when to perform the follow-up FDG-PET/CT. The lack of difference in the timing of follow-up FDG PET/CT between the impact and no-impact groups is likely due to the retrospective nature of this study, where follow-up FDG-PET/CT was performed at variable intervals based on the clinical course of the patients. To determine the optimal timing for follow-up FDG-PET/CT in monitoring treatment and its impact on management, future research should involve a prospective study with a planned algorithm that compares different time intervals.
Our study has several limitations. The retrospective design may have affected the quality of data collected and the ability to accurately assess the clinical impact of the FDG PET/CT. Additionally, there is an inherent selection bias in this observational study, as follow-up FDG-PET/CT was performed in specific patients where a change in the treatment was anticipated. The absence of data regarding whether the changes driven by FDG-PET/CT have improved patient outcomes (e.g., cure rate, recurrence rate) is another limitation of this retrospective study. The small sample size further limits our ability to perform subgroup analysis for specific focal infections. Moreover, being conducted at a single tertiary hospital, the present study population consisted of more complex cases, which may affect the generalizability of our results. Future prospective studies with larger cohorts are needed to validate these results, and such studies should also include cost-effectiveness analyses to support the integration of FDG-PET/CT into standard infectious disease management protocols.
In summary, follow-up FDG-PET/CT appears to play an important role in managing patients with focal infectious diseases by influencing therapeutic decisions, particularly in cases of focal infections caused by gram-positive bacteremia and in patients with unfavorable clinical courses. It could also help individualize the management of focal complicated infections.
Our study findings are consistent with recent literature, underscoring the increasing recognition of FDG-PET/CT’s impact on clinical outcomes in infectious disease management. As the use of FDG PET/CT becomes more widespread, future research should continue to explore and quantify the benefits of 18F-FDG PET/CT in the clinical practice of infectious diseases and its impact on personalized patient care.
Supplemental Material
sj-docx-1-tai-10.1177_20499361251391254 – Supplemental material for The impact of follow-up FDG-PET/CT on the management of focal infectious diseases: a retrospective cohort study
Supplemental material, sj-docx-1-tai-10.1177_20499361251391254 for The impact of follow-up FDG-PET/CT on the management of focal infectious diseases: a retrospective cohort study by Badarne Mohammad, Kagna Olga, Keidar Zohar and Ghanem-Zoubi Nesrin in Therapeutic Advances in Infectious Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.