
Abstract
Group B streptococcus (GBS) or Streptococcus agalactiae is a beta-hemolytic, Gram-positive coccus that can colonize the genitourinary and gastrointestinal tract of pregnant people. GBS can transition from asymptomatic colonization to pathogenic bacterium which can then lead to adverse pregnancy, maternal and neonatal outcomes. While much of the literature focuses on outcomes affecting the neonate, such as early- and late-onset neonatal sepsis, GBS is also thought to be associated with specific pregnancy and fetal adverse outcomes including preterm birth, preterm premature rupture of membranes, urinary tract infection, endometritis, and maternal sepsis. The objective of this literature review is to further address the known associations of these maternal and pregnancy outcomes, review the current strategies for GBS screening and preventative strategies, and explore the current maternal GBS vaccine candidates in development that may address the limitations of current prevention strategies with intrapartum antibiotic prophylaxis.
Introduction
Group B streptococcus (GBS) or Streptococcus agalactiae is a beta-hemolytic, Gram-positive coccus that can colonize the genitourinary (GU) and gastrointestinal (GI) tract of pregnant people.1,2 GBS in pregnancy can be associated with adverse maternal, fetal, and neonatal outcomes. Much of the published literature focuses on outcomes affecting the neonate such as early- and late-onset neonatal sepsis; however, less is known about direct mechanisms connecting these adverse maternal and pregnancy outcomes and GBS such as preterm delivery, preterm premature rupture of membranes (PPROM), urinary tract infection, endometritis, and maternal sepsis. The objective of this literature review is to further address the known associations of these maternal and pregnancy outcomes, review the current strategies for GBS screening and preventative strategies, and explore the current maternal GBS vaccine candidates in development that may address the limitations of current prevention strategies with intrapartum antibiotic prophylaxis. Given the large amount of literature available on neonatal outcomes associated with GBS, we focused instead specifically on maternal and pregnancy outcomes in our review.
Group B streptococcus in pregnancy
GBS classification is based on capsular polysaccharide (CPS) phenotype, with 10 known GBS serotypes: Ia, Ib, II, III, IV, V, VI, VII, VIII, and IX.3–7 Some serotypes have been associated with a higher likelihood of maternal and neonatal GBS disease while others have been more associated with asymptomatic carrier status.4,8 Schindler et al. showed that the dominant serotype in asymptomatic pregnant people was serotype VI (98 out of 240 isolates, 48%), while the dominant serotype in neonates with early onset GBS disease was serotype III (16 out of 19, 84.2%). 8 Serotype III has also been frequently associated with late onset neonatal GBS disease, neonatal sepsis, and meningitis. 9 In one South African study serotype III was noted to be more likely to be associated with persistent colonization. 10 In addition, GBS can be even further classified by sequence type (ST), or allelic profile, the majority of GBS human isolates being ST-1, ST-17, ST-19, or ST-23. 11 In one study ST-1 and ST-19 were more highly associated with asymptomatic GBS colonization, while ST-17 was more associated with neonatal invasive infections (p < 0.001). 11 Interestingly, all the strains of ST-17 were in serotype III. 11 The virulence of GBS is dependent on the CPS, thus antibodies against the CPS can provide type-specific protection, an important target for future GBS vaccines. 12
Prevalence of GBS colonization varies based on global geographic region. In a systematic review from studies published between 1997 and 2015 the prevalence of GBS colonization worldwide in pregnant people was found to be approximately 17.9% overall, with the highest rates noted in Africa (22.4%) followed by the Americas (19.7%) and Europe (19.0%). 13 The lowest prevalence was seen in southeast Asia (11.1%). 13 In a more recent meta-analysis, 19.7 million pregnant people were estimated to have been colonized by GBS globally in the year 2020, with the highest rates of colonization found in sub-Saharan Africa (6.1 million) and central and south Asia (4.4 million). 14 A meta-analysis that included 390 articles, 85 countries, and a total of 299,924 pregnant people found that the serotypes Ia, Ib, II, III, and V account for 98% of serotypes globally. The prevalence of serotype III is 25% (95% CI: 23%–28%) and is less often found in Central America (11%) and Asia (Southeast Asia 12% and South Asia 11%). There is a greater prevalence of serotype V in Western Africa and other serotypes (VI–IX) are more commonly found in Southeast Asia (Figure 1). 4

Distribution of maternal group B streptococcus colonizing serotype by United Nations subregion.
There are many risk factors that have been associated with GBS colonization in pregnancy, including race, ethnicity, age, socioeconomic factors, and medical conditions. One US study assessed 40,459 cases of GBS colonization and found that Black race was associated with increased maternal GBS colonization (odds ratio 1.54, CI: 1.36–1.74, p < 0.01), while Hispanic ethnicity decreased the risk of GBS colonization (OR 0.88, CI: 0.80–0.96; p = 0.003).15,16 There is conflicting data on whether maternal age impacts GBS colonization, as both younger and older maternal age have been associated with GBS colonization. One study in Canada found that women greater than 36 years old were eight times more likely to have persistent colonization, in the third trimester and 6 weeks postpartum, when compared to women less than 25 years. 17 While another study in the US found that the mean observed maternal age at delivery was lower among GBS colonized compared to GBS negative people. 16 Socioeconomic factors have also been associated with increased risk of GBS colonization; healthcare occupation, higher income, and greater educational attainment were associated with increased odds ratios for GBS colonization. 15
Lastly, certain medical conditions and co-morbidities have also been associated with increased risk of GBS colonization. Elevated BMI, including overweight, obese, and severely obese categories, has also been seen as an independent risk factor for GBS colonization.15,18,19 There is conflicting data on whether preexisting diabetes mellitus (DM) or gestational diabetes mellitus (GDM) increases risk of colonization in pregnancy. Nguyen et al. completed a literature review, including published studies on GBS colonization and diabetes from 1985 to 2016. 20 One study that assessed 60,029 pregnant people found that 3.5% versus 2.8% (p < 0.001) of pregnant people colonized with GBS had preexisting diabetes.16,20 This study additionally noted that there was a higher risk of GDM (RR 1.21, CI: 1.11–1.32). However, another study that evaluated 446 pregnant people with GDM and 1046 without GDM found no difference in colonization rates (12% and 12%, respectively).20,21 Similarly, a study conducted in Italy of 473 pregnant patients, 127 with DM and 346 without DM did not find a difference in GBS vaginal colonization between the two groups.20,22
The GI tract is the primary source of GBS colonization of the genitourinary tract. The study by Badri et al. was one of the first to describe the GI tract as the primary site of colonization by GBS. In their study of 789 pregnant patients, 142 (17.9%) rectal cultures tested positive for GBS versus 81 (10.2%) of vaginal cultures, 23 thus illustrating that vaginal colonization may be due to contamination from the GI tract. Colonization in the GU tract can be intermittent, transitory, or persistent.1,24,25 One Danish study collected GBS samples during early first trimester and late third trimester and found that 53% of participants were permanent non-GBS carriers, 28% were persistent GBS carriers, and 19% were intermittent carriers. 24 Another study assessed GBS colonization during each trimester and found that vaginal colonization changed from 24% in the first trimester to 18% in the second trimester, and 17% in the third trimester in their group of 42 pregnant patients. 25 Kwatra et al. found that the prevalence of the GBS colonization varied between 20–25 weeks, 26–30 weeks, 31–35 weeks, and greater than 37 weeks of gestational age in South Africa, with 27% of participants acquiring a new serotype. 10 All these studies illustrate the dynamic nature of GBS colonization in the GU tract. There is no evidence that GBS is transmitted sexually. Honing et al. in a case-control study of 432 non-pregnant female patients that attended a STI clinic in Rotterdam had a vaginal swab taken for bacterial culture that showed 12% of patients were colonized with GBS and no significant correlation was seen between sexual behavior variables, including lifetime partners, partners in last 6 months and 1 month, mean number of days since last sexual contact and use of condoms. 26 In addition, Jackson et al. collected perineal and anorectal swabs from 92 couples that attended a STI clinic and found that of the 20 patients that were both colonized only three were colonized with the same strains of GBS. 27
Association of GBS colonization with adverse maternal and fetal outcomes
GBS can transition from asymptomatic colonization to pathogenic bacterium which can then lead to adverse pregnancy, maternal and neonatal outcomes. Asymptomatic colonization is defined as a commensal bacterium of the microbiota that does not proceed to cause invasive infection.1,28 The transition from colonization to bacterial pathogen that causes invasive infection is not well understood. 28 Some observation studies suggest that a change from acidic to neutral environments can switch on the virulence-related genes of GBS, and that the control of virulence (Cov) regulator (R)-sensor (S) (CovRS) two-component regulatory system (TCS) can switch GBS from mucosal colonization to invasive infection. 28
While much of the literature focuses on outcomes affecting the neonate such as early- and late-onset neonatal sepsis, GBS is also thought to be associated with specific pregnancy and fetal adverse outcomes including preterm birth, PPROM, urinary tract infection, endometritis, and maternal sepsis.14,29–35 However, less is known about direct mechanisms connecting these maternal and pregnancy outcomes and GBS.
-
There are conflicting findings on associations between preterm birth and GBS colonization in the published literature. A global landscape review of GBS prevalence found an estimated odds ratio for an association between GBS and prematurity to be 1.30 (1.02–1.71), with an estimated 518,100 preterm birth associated with GBS colonization globally, corresponding to 3.5% of preterm births globally. 14 A systematic review and meta-analysis by Valkenburg-van den Berg et al. showed conflicting findings; an association was seen between maternal GBS colonization and preterm birth in cross-sectional and case-control studies when the GBS culture was completed at the time of delivery. However, this association was not seen in longitudinal cohort studies, when the GBS culture was collected earlier in pregnancy.29,30 A more recent systematic review and meta-analysis by Bianchi-Jassir et al. found a consistent increase in risk of preterm birth with maternal GBS colonization, with a strong association if GBS bacteriuria was present. 30
-
GBS colonization has been associated with a greater risk of PPROM and PROM in the published literature. A single-center retrospective cohort study from Japan of 1079 singleton pregnancies found that the incidence of PPROM (3.3% vs 1.9%, p = 0.335) and PROM (23% vs 14.2%, p = 0.062) was higher in GBS positive groups. However it was not statistically significant. 32 Older studies also show a statistically significant increase incidence of PROM in patients colonized with GBS. One prospective study of 6706 patients found PROM occurred in 15.3% of colonized patients compared to 8.1% not colonized (p = 0.0005). 39 Another study found that patients with GBS bacteriuria were at increased risk of PROM and premature delivery. 40
-
-
-
-
Current screening and preventive strategies
GBS can also be identified in pregnancy either through culture- or molecular-based methods. Culture-based screening is the gold standard for GBS detection as it maximizes GBS identification through the incubation of the specimen in enrichment broth prior to inoculation on the agar culture plates.1,49 In addition, the culture-based methods allow for antibiotic susceptibility testing to be completed. Molecular-based methods, such as nucleic acid amplification testing (NAAT), have been shown to offer similar or better rates of detection to culture-based screening if the incubation step precedes the NAAT analysis; however, it does not allow for antibiotic susceptibility testing.50–54 The benefit of NAAT methods is the rapid turnaround time which can be used in the intrapartum management of pregnant people with unknown or unavailable GBS status. However, due to swift turnaround time and lack of full enrichment broth incubation, sensitivity of the assay may be compromised. 52 Thus, at this time the Centers for Disease Control and Prevention (CDC) recommends that specimens undergo both the appropriate incubation time of 18–24 h at 35–37°C in the appropriate enrichment broth medium, to ensure accurate results over rapid turnaround times, regardless of the method used. 55
Earlier CDC guidelines had recommended the use of culture-based or risk-based screening as acceptable approaches to identify pregnant people that should receive intrapartum prophylaxis. 56 The risk-based approach used the presence of any of the following intrapartum risk factors: delivery prior to 37 weeks’ gestation, intrapartum temperature of greater than or equal to 100.4°F (38.0°C), or rupture of membranes greater than or equal to 18 h. 56 However, a large retrospective cohort study in 1998–1999 found that culture-based screening significantly lowered the risk of early onset GBS disease among infant when compared to the risk-based approach (adjusted related risk, 0.46; 95% CI: 0.36–0.60). 57 These findings led the CDC to change its guidelines.
Starting in 2002 the CDC has recommended universal antepartum culture-based screening of all pregnant people between 36 weeks and 37 weeks 6 days of gestation, regardless of mode ofdelivery.51,58 The screening goal is to collect the cultures within 5 weeks of birth, as studies have shown this time period to have the highest degree of accuracy in predicting GBS colonization at the time of delivery.59,60 The specimen should be collected from the lower vagina and rectum to increase the culture yield, as sampling from each location alone decreases the positive predictive value of the test. 61 Multiple studies have shown that self-obtained samples and clinician-obtained samples result in similar GBS culture yields.62–65 The results from the antepartum screening culture then dictate eligibility to receive intrapartum antibiotics to prevent early onset GBS disease. For pregnant patients with unknown GBS screening at the onset of labor, intrapartum prophylaxis is recommended with the presence of any of the risk factors discussed above, including a prior neonate with invasive GBS disease, known GBS positive status in previous pregnancy, or GBS bacteriuria during any trimester of the current pregnancy. 1
Given loose associations of maternal and pregnancy outcomes and limited knowledge of pathophysiological mechanisms between GBS colonization and these outcomes, the focus on preventive therapy and treatment has been to decrease the risk of early-onset neonatal sepsis in the infant with intrapartum antibiotic prophylaxis. The efficacy of intravenous intrapartum antibiotic prophylaxis has been shown to be anywhere from 85% to 100% to prevent EOD among pregnant patients colonized with GBS.66–69 Intravenous penicillin is the preferred first-line antibiotic for intrapartum prophylaxis, with intravenous ampicillin as an acceptable alternative to penicillin.1,67,70 However, penicillin is preferred due to its narrower antimicrobial activity against Gram-positive bacteria and decreased possibility of development of resistance in other vaginal organisms.1,55
Patients with a penicillin allergy are recommended (1) to be assessed for severity of reaction and (2) to assess the susceptibility of GBS isolate to clindamycin to determine the optimal intrapartum antibiotic therapy. 1 A high-risk penicillin allergy is defined as the development of anaphylaxis, recurrent reactions, reactions to multiple beta-lactam antibiotics, positive penicillin allergy test, or severe delayed-onset reactions (e.g., eosinophilia and systemic symptoms/drug-induced hypersensitivity syndrome, Stevens-Johnson syndrome, or toxic epidermal necrolysis).1,71 In patients without a high-risk penicillin allergy, cefazolin, a first-generation cephalosporin, is recommended as intrapartum prophylaxis, as GBS has a high susceptibility to this antibiotic, and cefazolin has been shown to have high amniotic fluid and fetal blood levels.1,72–75 In patients identified as high-risk, either clindamycin or vancomycin are recommended as intrapartum prophylaxis. 1 Erythromycin is no longer recommended as an alternative given the high rates of GBS resistance to this antibiotic and its poor ability to cross the placenta which leads to low drug levels in amniotic fluid and fetal blood.75–77 Clindamycin is recommended as an alternative if the GBS isolate is known to be susceptible to clindamycin.1,76 If the GBS isolate is not susceptible to clindamycin, intravenous vancomycin is recommended.1,78–80
Other preventative modalities such as intramuscular intrapartum antibiotic prophylaxis, antenatal antibiotics, chlorhexidine vaginal wipes, or douches have not been proven to be as effective in the prevention of EOD.55,81–84 There is some concern regarding the development of antibiotic resistance of some GBS isolates. 57 There are no preventative strategies in place that address the prevention of many of the adverse pregnancy and maternal outcomes described above.
GBS vaccine in pregnancy
There are several maternal GBS vaccine candidates in development that may address the limitations of current prevention strategies with intrapartum antibiotic prophylaxis. As previously discussed, while intrapartum prophylaxis can prevent early-onset disease in infants it is not effective in the prevention of late-onset disease and adverse maternal and pregnancy outcomes. Furthermore, a GBS vaccine would reduce antibiotic use intrapartum, thereby reducing risk of antibiotic resistance and possible interference with the infant microbiota. Lastly, a vaccine would have an impact on a global scale, particularly in areas where pregnant patients do not have access to screening or intrapartum antibiotic prophylaxis. 85
Progress toward a GBS vaccine has been slow despite the fact that as early as 1976 Baker et al. demonstrated that transplacental transfer of maternal antibody of CPS type III could protect the infant from invasive GBS infection from CPS type III strains. 86 It was not until 2015 and 2016 that the World Health Organization (WHO) in the Product Development for Vaccines Advisory Committee prioritized the development of GBS vaccine. 87 In addition, the WHO has included milestones in its “Defeating Meningitis roadmap” for the GBS vaccine, including to have at least one GBS vaccine licensed by 2026 and have introduced the vaccine to at least 10 countries by 2030. 88 There have thus far been three GBS vaccine candidates (Figure 2):
1. Two polysaccharide conjugate vaccines that target multiple GBS serotypes.
a. The hexavalent conjugate vaccine that targets the serotypes Ia, Ib, II, III, IV, and V.
b. The trivalent conjugate vaccine that target serotypes Ia, Ib, and III.
The trivalent conjugate vaccine which underwent several phase I and II trials has now been discontinued due to limited disease coverage and variable immunogenicity in human trials.89,90,93

Group B streptococcus (GBS) vaccine development pipeline.
The single dose hexavalent CPS-cross reactive material 197 glycoconjugate vaccine (GBS6) is designed using surveillance data from global whole-genome sequencing of recovered GBS isolates that are responsible for invasive neonatal GBS disease. 93 In phase I/II, placebo-controlled, observer-blinded, dose-escalation trial in healthy, non-pregnant adults in the US the vaccine was found to be well tolerated with a good immune response that persisted for 6 months after vaccination. 92 As of 2025, a phase II randomized clinical trial utilizing GBS6 is underway. 12 Part of phase II was conducted in South Africa where the vaccine was given in six formulations, which included three dose groups (5-, 10-, or 20-μg CPS per serotype) each with and without aluminum. There were 360 pregnant people that underwent randomization, 40 assigned to each of the six formulations and 120 assigned to the placebo. The primary outcome was to assess safety and immunogenicity of a single dose GBS6. No safety concerns, including local and systemic reactions, were associated with the GBS6 compared to placebo in the study. An IgG response was noted for all six serotypes that continued through delivery and was transferred to the infant. 12 Transplacental antibody transfer was noted at levels postulated to be associated with reduced risk of invasive GBS disease, specifically cord blood ST-specific antibody levels were mostly above the protective thresholds identified in the accompanying epidemiological study of natural antibodies, making this a promising vaccine for prevention of GBS disease in the neonate and possibly to reduce risk of adverse maternal and pregnancy outcomes. 95 A final formulation is being evaluated in the US, UK, and South Africa to complete phase II of the clinical trial and inform a planned phase III clinical trial development program.
The protein vaccine, GBS-NN, contains structural components of GBS alpha-like proteins (Alps), fused N-terminal domains of GBS Alpha C and Rib proteins.96,97 It has been shown that low occurring Alpha C or Rib specific titers in maternal and neonatal serum can correlate with GBS disease which influenced the creation of the GBS-NN vaccine.96,98 Phase I clinical trial in non-pregnant individuals of this vaccine was overall well tolerated, with mainly mild injection site reactions observed. The GBS-NN vaccine showed a high immunogenic response after two doses of 50 µg. 97 The vaccine has also been tested in murine models where an increase in GBS-NN IgG specific titers has been shown to lead to reduced burden of systemic GBS and improved fetal and neonatal survival. 96 As of 2025, phase II clinical trial in pregnant patients is ongoing.
There are several published studies seeking to quantify the impact of a future GBS vaccine on maternal and neonatal morbidity and mortality. One paper summarized the estimated health impact of GBS vaccine using Seale et al.’s global estimates of incidence and case fatality of GBS in 2017 and Gonçalves et al.’s estimates of global burden of GBS in 2020 using Bayesian modelling.14,33,85 The potential health impacts are summarized in Tables 1 and 2. The effect a GBS vaccine may have on adverse maternal and pregnancy outcomes associated with GBS colonization and disease is less clear. More studies in this area are warranted to address this knowledge gap.
Health impacts of a GBS vaccine using previously published 2017 global estimates of incidence and case fatality of GBS, assuming a GBS vaccine with an 80% efficacy rate and reaching 90% coverage.
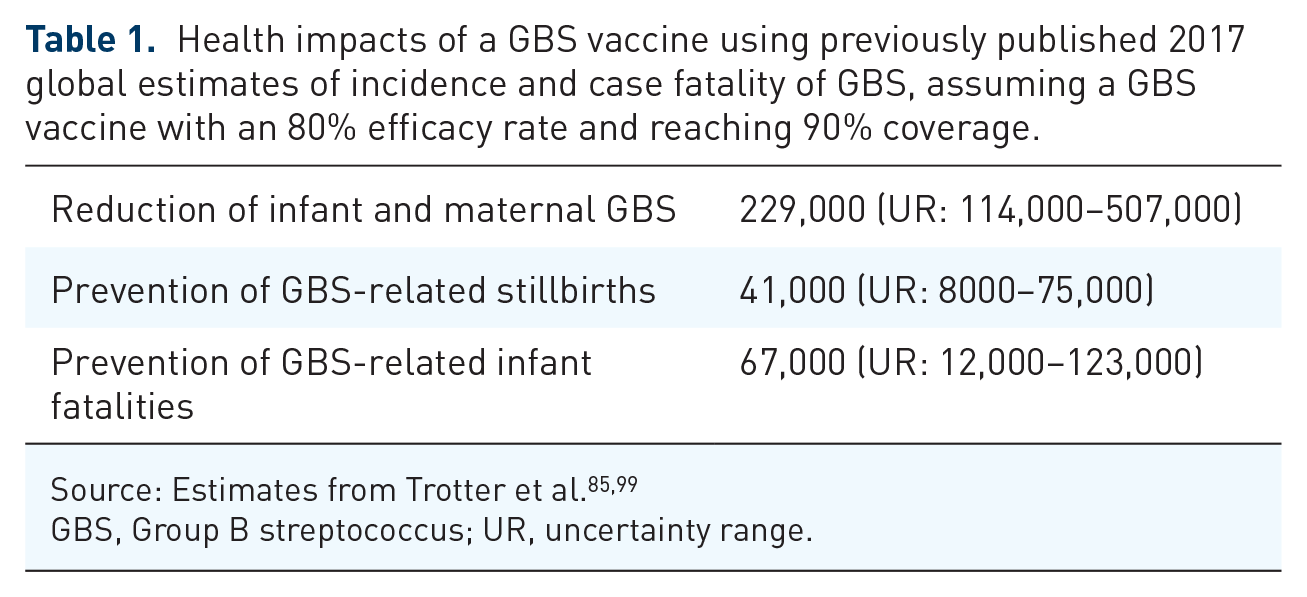
GBS, Group B streptococcus; UR, uncertainty range.
Health impacts of a GBS vaccine using 2020 previously published estimates of global burden of GBS in 2020 using Bayesian modelling, assuming a GBS vaccine with an 80% efficacy rate and reaching 90% coverage.

GBS, Group B streptococcus; UR, uncertainty range.
Conclusion
GBS in pregnancy can transition from asymptomatic colonization to pathogenic bacterial infection which can then lead to adverse pregnancy, maternal, and neonatal outcomes. Literature on associations of GBS with neonatal outcomes such as early- and late-onset neonatal sepsis is more robust compared to associations with maternal outcomes. More research is needed to better understand the impact of GBS colonization in pregnancy and adverse maternal and pregnancy events. The development of a GBS vaccine emerges as a promising avenue that not only will address the risk of adverse neonatal outcomes but may also mitigate adverse pregnancy and maternal outcomes.