
Abstract
Background:
Urinary tract infections (UTIs) are common and result in a significant impact on quality of life (QoL). Despite their prevalence, there seems to be a lack of evidence around patient-reported outcomes and measuring tools such as scoring systems and nomograms in UTIs. Patient-reported outcome measures (PROMs) help us measure patient-related symptoms and their QoL.
Objective:
Our literature review shows an up-to-date “atlas” of the available PROMs, nomograms and scoring systems that can help clinicians in treatment decisions and track treatment response in patients with UTIs.
Design:
Systematic review of the literature.
Data sources and methods:
A comprehensive systematic review was carried out on PubMed Medline, Scopus and CINAHL, according to PRISMA guidelines, using search terms related to PROMs, nomograms and scoring systems used in simple and complicated UTIs. A narrative review was done, and tool characteristics, accuracy, validation, and applicability were collected and summarized.
Results:
Sixty-two articles (with 16 different PROMs) were included in the final review. These included generic tools such as the 36-Item Short Form Health Survey and specific tools like the Acute Cystitis Symptom Score and Recurrent Urinary Tract Infection Impact Questionnaire, amongst others. While scoring systems seemed to be used for severe infections such as Fournier’s gangrene and emphysematous pyelonephritis, nomograms were primarily used for diagnosis and risk prediction. PROMs are useful tools and have utility within the management of patients with UTIs, but further clarity is needed as to which of these tools is most appropriate for each type of UTI as each offer their respective advantages and disadvantages.
Conclusion:
This atlas is the first comprehensive review of PROMs, scoring systems and nomograms in the management of UTIs. While PROMs improve patient care, further standardisation, external validation and accuracy are needed. While nomograms and scoring systems can help clinicians, these must be tailored to individual patients based on their specific clinical scenarios.
Trial registration:
PROSPERO registration number CRD42025625865.
Background
Urinary tract infections (UTIs) are amongst the most common bacterial infections,1,2 with an estimated annual incidence of 12.6% in females and 3% for men 3 Between 50% and 60% of females will have a UTI in their lifetime. 4 Furthermore, UTIs can affect all ages and their presentation can vary immensely. Uncomplicated UTIs often resolve quickly, especially in young females. Contrastingly, UTIs affecting elderly patients can result in significant morbidity. 5 In addition, UTIs can often recur, with approximately 25% of females with UTI going on to suffer a further UTI within 6 months.1–3,6,7 Recurrent UTI (rUTI) can have a significant effect on patients, affecting quality of life (QoL) and daily activities, leading to a reduced quality of both intimate and social relationships, reduced self-esteem and impaired capacity for work.7–9
Classification of UTI is important. They are classified according to the location, whether they are confined to the lower urinary tract or upper urinary tract, as well as to whether they are complicated or uncomplicated. 3 Of note, any UTI affecting male patients is classified as complicated. An uncomplicated UTI is one occurring in a non-pregnant patient in the absence of structural or functional abnormality, who has not had instrumentation of the urinary tract, either through catheterisation or surgical instrumentation. 3 Further, UTI can be recurrent, defined as at least three UTIs in a year or two UTIs in 6 months, 9 or associated with a catheter, referred to as a catheter-associated UTI (CAUTI).
There is a paucity of literature concerning the impact of UTIs on patients’ QoL. 8 Patient-reported outcomes (PROs) are studied throughout medicine and have become increasingly utilised, with the volume of academic literature concerning them increasing rapidly.10–14 These PROs are measured using patient-reported outcome measures (PROMs). These are instruments or tools, usually patient completed questionnaires, used to provide information from a patient perspective, without interpretation of a clinician, giving valuable information regarding a patient’s symptoms, health-related quality of life (HRQoL) and functional status. 13 By including the patient’s perspective, it allows for more holistic and patient-centred care, 13 which can facilitate shared decision making, monitor symptoms and improve overall patient care. 15 Generally, PROMs can be characterised as disease specific and generic.10,14 Generic PROMs allow for comparison across several patient groups and settings, 10 whereas disease-specific PROMs tend to inherently possess higher validity. 14 It has been recommended that using disease-specific and generic PROMs in conjunction provides the broadest range of information. PROMs in urology have been studied in a number of sub-specialities, including endourology,16,17 andrology, 18 reconstructive urology19,20 and oncology.21–24 There is, however, little literature concerning PROMs regarding UTI. Piontek et al. 25 recently carried out a systematic review and analysis of PROMs specifically for uncomplicated UTI in women, and Bermingham and Ashe 26 carried out a systematic review in 2012 to specifically assess QoL measures available for patients with UTI.
In addition to PROMs, we have compiled the current scoring systems and nomograms used in relation to UTIs. Scoring systems use different physiological, biochemical and radiological variables to provide an objective measurement of the severity of an illness. 27 Nomograms are a pictorial representation of a complex mathematical formula. Medical nomograms use biochemical and clinical variables to predict the probability of an event, such as death, for a given individual. 28 Scoring systems in medicine traverse the full spectrum of specialities and disease severity, with an estimated 250,000 available for use. 29
The aim of this study was to conduct a review of the literature to compile an up-to-date “atlas” of the available PROMs, nomograms and scoring systems that can be used in patients with urinary tract infections, which are common and can in. We aim to provide the clinician with an overview of the available tools that can be used when managing patients with UTI, both in terms of disease severity and the impact of UTIs on patients’ QoL. We also hope this atlas will serve as a reference point for future researchers and clinicians assessing the psychosocial impact of UTI on patients.
Methodology
A comprehensive systematic review of the literature was carried out using the clinical databases PubMed Medline, Scopus and CINAHL, according to Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. 30 The review was registered with PROSPERO (Registration number CRD42025625865). Search protocols were tailored to each of the databases. Search terms can be found in Appendix 1. Boolean operators “AND”/”OR” were used to refine results. Due to the heterogenous nature of the reported data, quantitative analysis was not possible and therefore a narrative review was carried out. Bibliographies of included studies were manually searched to identify other relevant articles. Screening of articles was carried out by authors NH and AD, with queries regarding articles answered by author BKS. An assessment of the risk of bias of studies was made using Cochrane risk of bias tools.
The PICO statement for this review is as follows:
P = All patients with UTI (uncomplicated acute urinary tract infection, complicated urinary tract infection, rUTI, CAUTI, pyelonephritis, emphysematous pyelonephritis (EP), emphysematous cystitis, Fournier’s gangrene (FG), epididymitis, epididymoorchitis, prostatitis and urethritis).
I = PROMs, nomograms and scoring systems used for patients with UTI.
C = Not applicable.
O = Which PROMs, nomograms and scoring systems are currently available for UTI and what are their benefits and drawbacks.
Evidence acquisition: Criteria for considering studies for this review
Inclusion criteria:
All articles written in the English language
Patients of all age groups with UTI, where a PROM, nomogram or scoring system was used and assessed in the English language
For this review, we did not include PROMs, scoring systems or nomograms used to assess patients with urosepsis specifically. This decision was made due to the large volume of available scoring systems and nomograms for urosepsis, which exceeded an acceptable amount for this review. Further work will focus specifically on urosepsis.
Results
A total of 16 different PROMs were identified; we identified studies where the Short form-36 health survey (SF-36) was used for both acute uncomplicated and recurrent UTI (Figure 1). These PROMs, their characteristics, advantages and drawbacks are summarised in Tables 1 to 4. Externally validated tools are highlighted in green. Figure 2 gives an overview of the number of PROMs, nomograms and scoring systems used in each sub-category of UTI.

PRISMA flowchart of the included studies.
Patient-reported outcome measures in acute uncomplicated UTI.

Externally validated tools are highlighted green.
HrQoL, health-related quality of life; LUTS, lower urinary tract symptoms; QoL, quality of life; UTI, urinary tract infection.
Patient-reported outcome measures in acute uncomplicated UTI continued.

Externally validated tools are highlighted green.
ACCS, Acute cystitis symptoms score; AIA, Activity impairment assessment; EQ VAS, EQ visual analogue scale; HrQoL, health-related quality of life; LUTS, lower urinary tract symptoms; PGCMS, Philadelphia Geriatric Center Morale Scale; QoL, quality of life; QWB, Quality of Well-Being scale; SF-36, 36-Item Short Form Health Survey; UTI, urinary tract infection; UTISA, UTI symptoms assessment questionnaire; UTI-SIQ-8, Urinary tract infection-Symptom and Impairment Questionnaire.
Patient-reported outcome measures in recurrent UTI.

Externally validated tools are highlighted green.
HrQoL, health-related quality of life; SF-12v2, short form – 12 version 2; UTI, urinary tract infection.
Patient-reported outcome measures in recurrent UTI continued.
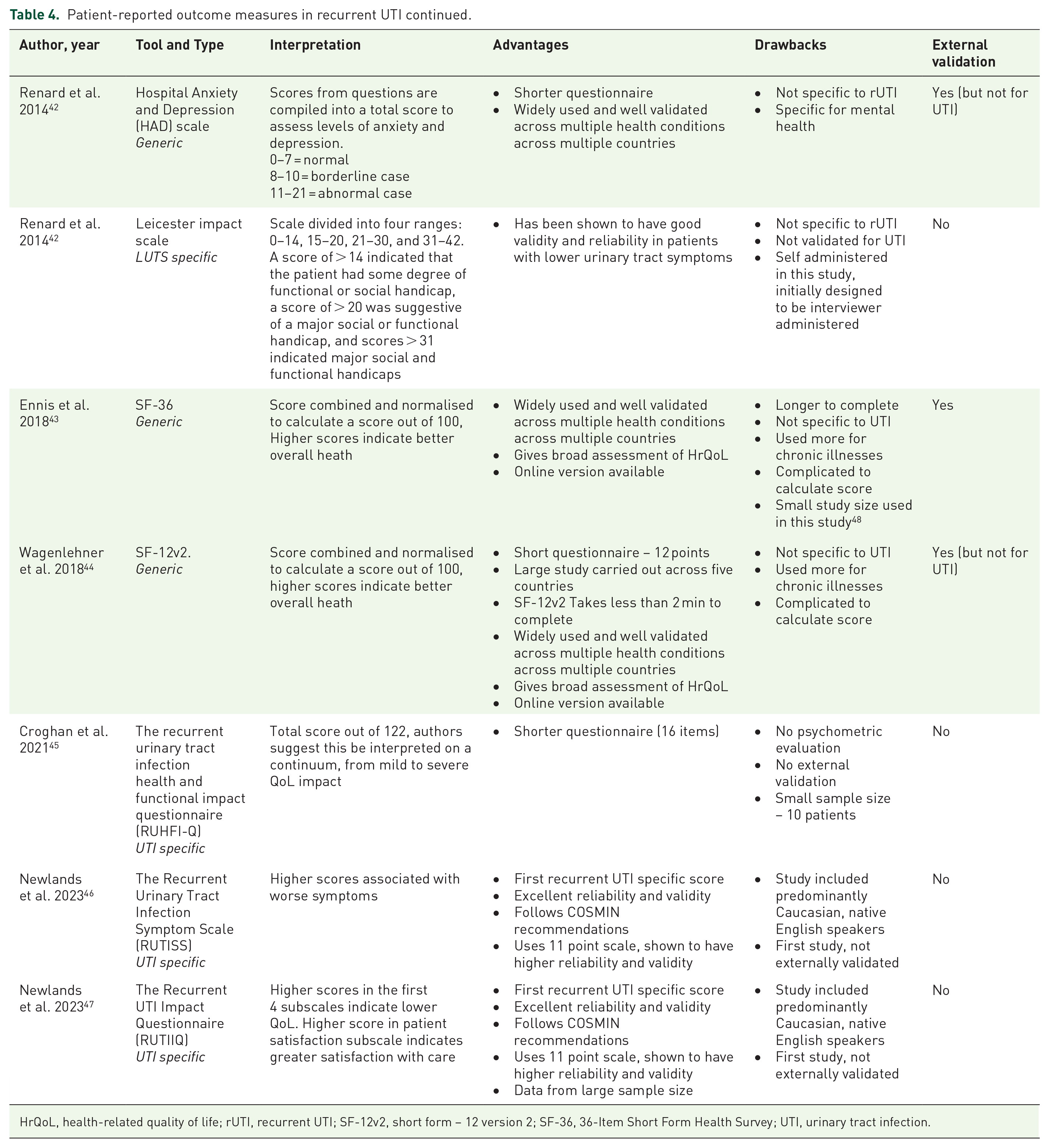
HrQoL, health-related quality of life; rUTI, recurrent UTI; SF-12v2, short form – 12 version 2; SF-36, 36-Item Short Form Health Survey; UTI, urinary tract infection.

Summary of the number of PROMs, nomograms and scoring systems identified for each sub-category of UTI.
Patient-reported outcome measures
Acute uncomplicated UTI
Ten PROMs were identified that were used to assess patients with acute uncomplicated UTI31–40 are summarised in Tables 1 and 2. The activity impairment assessment (AIA) was the first UTI-specific PROM and was developed by Wild et al. in 2005, 31 based on an existing work productivity measure. 49 This PROM was designed to assess the degree to which work or normal activities had been impaired as a result of a UTI. The data for the validation study for the AIA came from an existing clinical trial, with the psychometric properties of the PROM assessed by the pattern of association with the Kings health questionnaire (KHQ), which is a validated PROM used to assess the impact of urinary incontinence on female patients’ QoL. 50 The AIA is a 5-item questionnaire, making it quick to complete. It has also been translated to the French language and been externally validated. Despite its rigorous study design, with a reasonable sample size of 326 patients, plus its ease of use, it has not been studied widely in the literature.
The UTI symptoms assessment questionnaire (UTISA) is a 14-item UTI-specific PROM designed specifically for females with UTI and developed by the same authors of the AIA.32,31 Data for the UTISA 32 validation study came again from a clinic trial. The UTISA is designed to assess the severity and bother of seven key UTI symptoms. It was again compared against the KHQ and has been externally validated. Is should however be noted that in their systematic review, Piontek et al. 25 found that the PROM had insufficient content validity.
Ernst et al. 33 in 2006 used the quality of well-being (QWB) scale to assess QoL in patients with acute uncomplicated UTI. This is a 71-item generic PROM already widely used and taking up to 20 min to complete. The study did not aim to assess the validity or accuracy of the PROM, and we did not find QWB used elsewhere in UTI patients, possibly due to the prolonged administration time of the PROM. Another generic PROM, the Health Utilities Index Mark 2 measure of health-related quality of life (HUI2), was used by Maxwell et al. 34 in 2009 to assess the HRQoL of elderly care home residents. They used linear regression models to assess the association between patient characteristics, including UTI and that of HRQoL. They found that UTI had a statistically significant negative impact on HRQoL. The PROM itself is 31 items long, available in multiple languages and states that it can identify 24,000 ‘individual health states’. 34 Regardless, UTI was only one of several patient characteristics studied in this article, and there is no further literature describing the use or external validation of the HIU2 in UTI patients.
The Philadelphia Geriatric Center Morale Scale (PGCMS) is a generic PROM designed for elderly patients and is a 17-item questionnaire designed to assess morale of patients. 35 The authors found that UTI significantly reduced morale. However, as with the QWB and HUI2, there is no other literature showing its use in assessing UTI patients. In 2014, Alidjanov et al. 36 produced the Acute cystitis symptoms score (ACSS). This is an 18-point, self-administered questionnaire designed to aid in clinical diagnosis and follow-up of acute uncomplicated cystitis (AUC) in women, including questions regarding symptoms of UTI and QoL. It has been found to be highly sensitive (94%) and specific (90%) in diagnosing UTI and has been validated in multiple languages. While acting as a diagnostic tool, the ACSS also assesses the impact of UTI on patients’ HRQoL. It has been described as having sufficient content validity and alongside the UTI-SIQ-8, was one of only two PROMs recommended for use in acute uncomplicated UTI in females by Piontek et al.
In 2017, Holm et al. 37 published their work on a UTI-specific PROM in the form of a symptom diary. This covers a broad range of different dimensions of patient-experienced UTI not addressed in other PROMs and shows good content validity as well as being psychometrically validated. However, the PROM itself is only available for use after written confirmation by the authors and we could not identify any external validation in the literature. Alanazi et al. 38 in 2020 evaluated the HRQoL of women with acute UTI using the generic PROM the EQ-5D-3L, an extensively validated and robust PROM developed by the EuroQoL group. The EQ-5D-3L consists of two pages: the EQ-5D descriptive system and the EQ visual analogue scale (EQ VAS). The EQ-5D sections collect PRO information concerning mobility, self-care, usual activities, pain/discomfort and anxiety/depression. The EQ VAS consists of a patient-rated numerical score out of 100 for a patient’s perceived overall health. This combination allows for a broad range of information concerning patients’ HRQoL. Although this PROM has been externally validated across a number of conditions, it has not been externally validated for UTI.
As previously mentioned, the UTI-SIQ-8, developed by Gágyor et al. in 2021, 39 is another PROM that was recommended for use by Piontek et al. 25 This PROM has been shown to have high reliability and validity when compared with the validated tools EQ-5D and VAS and is available in an online version. Of note, the authors did not recommend use in clinical practice at the time of publication, perhaps whilst awaiting external validation. This tool is short, only eight items long, with four questions concerning UTI symptoms and four concerning impact on QoL. The final PROM that we identified was the short form-36 (SF-36) survey, that was used in a 2023 study by Thompson et al. 40 assessing activity impairment, health-related quality of life and productivity in patients with UTI. The SF-36, like the EQ-5D-3L, is a well-validated PROM that is used across a number of conditions, although these tend to be chronic conditions primarily. It is a longer tool, with 36 items producing a total score out of 100, although it is noted that calculation of the final score is difficult.
Recurrent UTI
Seven PROMs were identified that were used in patients with rUTI,42–46 these are summarised in Tables 3 and 4. Renard et al. 42 carried out a study involving 575 patients where they utilised the Hospital Anxiety and Depression (HAD) scale and Leicester impact scale, to assess the impact of rUTI on patients’ QoL. The HAD is a generic PROM that is over 30 years old and has been widely used and well validated. It assesses levels of anxiety and depression, and was designed for patients in an outpatient setting. It is quickly completed, with only 14 questions. It has not been used elsewhere in patients with UTI but has been recently used in patients with lower urinary tract symptoms (LUTS). 51 The Leicester impact scale was developed in 2004 by Shaw et al. 52 as a PROM to be used to assess the HRQoL of patients with LUTS. The initial study revealed high levels of internal consistency and acceptable construct validity, however, this PROM was interviewer administered in this initial study and was patient-administered in the study by Renard et al. 42
A generic PROM that was used in both acute uncomplicated and rUTI patient populations was the SF-36. For rUTI patients, it was assessed in the study by Ennis et al. 43 in 2018. This was a small study with a sample size of 85 patients. As the SF-36 is more often used for chronic conditions, rUTI is perhaps a more suitable population to use the SF-36. Wagenlehner et al. 44 used the Short form – 12 version 2 (SF-12v2) in their GESPRIT study assessing the effect of rUTI on QoL. The SF-12v2 is a shortened version of the SF-36, 12 items long and taking only 2 min to complete. It is widely used and well validated across multiple health conditions across multiple countries, although this is the first study that we identified that used this PROM.
Since 2021, we identified three rUTI-specific PROMs that have been developed. The first of which is the recurrent urinary tract infection health and functional impact questionnaire (RUHFI-Q), developed by Croghan et al. 45 This article reports on the development and feasibility testing of the PROM, but unfortunately is a small sample size of 10 patients, it has yet to undergo psychometric testing or external validation. The two most recent PROMs for patients with rUTI were developed by Newlands et al.46,47 The Recurrent Urinary Tract Infection Symptom Scale (RUTISS) is a PROM focusing on symptoms and pain associated with rUTI. The 28-item questionnaire includes an assessment of UTI symptom frequency, a global rating of change scale, a urinary symptom subscale, a UTI pain subscale, and an additional section evaluating critical clinical features such as diabetes and pregnancy. It shows excellent reliability and construct validity. The Recurrent UTI Impact Questionnaire (RUTIIQ) 47 is a 28-item questionnaire that assesses the patient-reported psychosocial impact of living with rUTI symptoms and pain. It has been developed by the same team as that of the RUTISS and instead focused on the impact of rUTI on HRQoL. It shows good psychometric properties and construct validity. Of note, development of the PROM was rigorous, with a heterogeneous and international patient cohort utilised. These two PROMs have yet to be externally validated, but we predict that they will provide a broad assessment of the impact of rUTI on patients from a symptomatology and QoL perspective.
Other types of UTI
We did not identify other examples of PROMs being used in patients with other types of UTI. In their 2023 qualitative analysis, Suijker et al. 53 found that necrotising soft tissue infections have a significant impact on patients’ HRQoL similar to that of burns victims. However, a specific PROM was not used in this study.
Scoring systems and nomograms
Acute uncomplicated UTI
The accuracy of most nomograms was measured using the C-index. These scores range from 0.5 to 1.0, with a score of 0.7 or higher generally accepted as a good predictive model. 54 Scoring systems analysis was tested using receiver operating characteristic (ROC) curves and area under the curve (AUC) values. Again, AUC values range from 0.5 to 1.0, with a value of 0.5 indicating that the test is no better than random chance. Values of 0.8 and above are generally thought to correspond to a good predictive model. 55
We identified six nomograms used in patients with acute uncomplicated UTI are summarised in Table 5.56–61 The earliest nomogram identified was that of García-Tello et al. in 2018. 56 This nomogram was developed to predict the probability of UTI by extended spectrum beta-lactamase (ESBL) producing Enterobacteriaceae. This was a large study involving 1524 patients, with the development of the nomogram involving a development cohort and validation cohort and showing good discriminative accuracy of 79% (95% CI 0.77–0.83). It should be noted that all but select few of the nomograms and scoring systems we identified were single centre, retrospective studies, without external validation, unless specified otherwise in this article.
Scoring systems and nomograms in acute uncomplicated UTI.

AUC, area under the curve.
In 2019, Ben Ayed et al. 57 produced a scoring system to predict the risk of multi-drug resistant (MDR) organisms in community-acquired UTI. This showed an AUC score of 0.71. The total score was out of 18 and at a cut-off score of ⩾ 12), the specificity and PPV achieved 100%. Again, this was a single centre, retrospective study and it should be noted that rates of MDR organisms vary globally, limiting the generalisability of these two scoring systems.
In 2021, Zhang et al. 58 developed a nomogram to predict the risk of sepsis in patients with UTI, and this nomogram included 11 variables and is the first model to predict probability of sepsis in patients with UTI. It has been shown to have a reasonable AUC of 0.775 and at the optimal cut-off, reasonable sensitivity, and specificity at 0.706 and 0.701, respectively. A nomogram developed to predict UTI risk in a specific population was that developed by Li et al. in 2023. 59 This nomogram predicts the risk of UTI in children less than three years of age. This was a large study involving 1271 patients and interestingly, the authors created three different nomograms for three different clinical settings. These settings were a local clinic, medical centre and regional hospital, and the nomogram variables were altered depending on the setting, according to what investigations would be commonly available. All the nomograms were shown to be accurate with AUC’s for the local clinic being 0.9133, the medical center being 0.9033 and regional hospital being 0.8933. The final nomogram identified was another developed to predict the probability of ESBL-positive UTI. Lu et al. 60 collected data over a 25-year period from a single institution and found that the nomogram had moderate accuracy (C-index 0.741). As previously mentioned, the variation of resistant organisms’ from region-to-region makes generalisability of the nomogram difficult.
Complicated UTI and rUTI
We identified six nomograms and one scoring system used in patients with either rUTI or complicated UTIs61–67 are summarised in Table 6. Cai et al. 62 developed the LUTIRE nomogram in 2014 to predict the risk of UTI recurrence within 12 months, the only nomogram identified that assessed patients regarding rUTI. It contains only six variables, is quick to calculate, and is shown to be accurate (AUC 0.85, 95% CI 0.79–0.91). Of note, LUTIRE was externally validated in a Brazilian cohort in 2020. 68
Scoring systems and Nomograms in complicated UTI and rUTI.

Externally validated tools are highlighted green.
AUC, area under the curve; CRP C-reactive protein; rUTI, Recurrent UTI; UTI, urinary tract infection.
In 2014, Van der Starre et al. 63 assessed the prognostic value of pro-adrenomedullin, procalcitonin (MR-proADM) and C-reactive protein (CRP) in predicting outcome of febrile UTI. They found that the AUC for MR-proADM was 0.83 (95% CI 0.71–0.94) and PCT was 0.71 (95% CI 0.56–0.85). CRP, erythrocyte sedimentation rate (ESR) and leucocyte count lacked diagnostic value. This was a prospective, multicentre study and the first to assess the prognostic value of MR-proADM. Lalueza et al. 64 developed a nomogram in 2019 to predict the risk of bacteraemia in patients with UTI attending the emergency department. This has been classified as a complicated UTI related nomogram as only patients that underwent blood culture were included in this retrospective study, which would have likely led to patients with more severe UTIs being included in the development of the model. The nomogram had a C-index of 0.793, indicating moderate accuracy of the model.
Wang et al.’s 2021 nomogram concerns UTI risk in patients with neurogenic bladder. 65 This short and easy to use, five item nomogram was shown to be highly accurate with a C-index value of 0.921 (95% confidence interval: 0.87396–0.96804). Another nomogram identified was developed to assess the 90-day risk of UTI in patients undergoing radical cystectomy and urinary diversion. 67 This nomogram was shown to be accurate with a C-index of 0.823 (95% CI: 0.723–0.824). Buzzi et al. 67 produced a nomogram designed to assess the risk of positive urine culture in patients who had undergone recent lower gastrointestinal surgery. It should be noted that the end point was positive urine culture, not UTI. Also, the C-index of 0.71 did not confer excellent accuracy. The final nomogram identified was that of Tang et al. 66 They developed a nomogram to predict the risk of UTI in geriatric patients with hip fractures in 2023. This study included 900 patients and was found to have an AUC of 0.803 and a C-Index of 0.829 (95% CI, 0.758–0.900), showing good accuracy.
Catheter associated UTI
We identified two nomograms concerning CAUTI,65,66 summarised in Table 7. Li et al. 69 developed a nomogram to predict the risk of CAUTI in neuro-intensive care patients. The nomogram only consisted of four variables and showed good calibration and discrimination ability. The second nomogram we identified for CAUTI was developed by Wang et al., 70 this was another quick and easy to use nomogram only including five variables. It was shown to be accurate with a C-index of 0.810.
Scoring systems and nomograms in catheter-associated UTI.

AUC, area under the curve; UTI, urinary tract infection.
Pyelonephritis
We identified one nomogram and three scoring systems used in patients with pyelonephritis.71–73 These are summarised in Table 8. Fang et al. 73 developed a nomogram to diagnose pyelonephritis in paediatric patients with UTI. This easy-to-use nomogram, with only four variables, was highly accurate with an AUC of 0.89. Of note, patients who did not undergo dimercaptosuccinic acid (DMSA) scan were excluded from the study, likely leading to a bias in the patients included, who would likely have more severe UTI. In 2016, Kubota et al. 71 published a scoring system that they named the PUSH score, an acronym for P – Performance status ≧ 3, U – presence of Ureteral stones, S – Sex, female, H – Hydronephrosis. They found that the group of patients with a PUSH score of 3 points or more had a significantly higher rate of SS complications than the group of patients with a PUSH score of 1 to 2 points (p = 0.0000036). This is a short score, again only consisting of four variables. Following this, Valent et al. 72 used the Acute Physiology and Chronic Health Evaluation II (APACHE II), as well as the Modified Obstetric Early Warning System (MOEWS), to assess for correlation between these two scores and prolonged admission or maternal morbidity. This was the only example of the utilisation of established scoring systems being studied in pyelonephritis specifically. They found reasonable accuracy for predicting maternal morbidity in both the APACHE II (AUC 0.72) and MOEWS (AUC 0.71). This was a multicentre study involving five centres, but the sample size was small, at 123 patients. Both scores are widely used, APACHE II specifically for intensive care patients and MOEWS for pregnant patients, but not externally validated for use in pyelonephritis patients.
Scoring systems and nomograms in pyelonephritis.
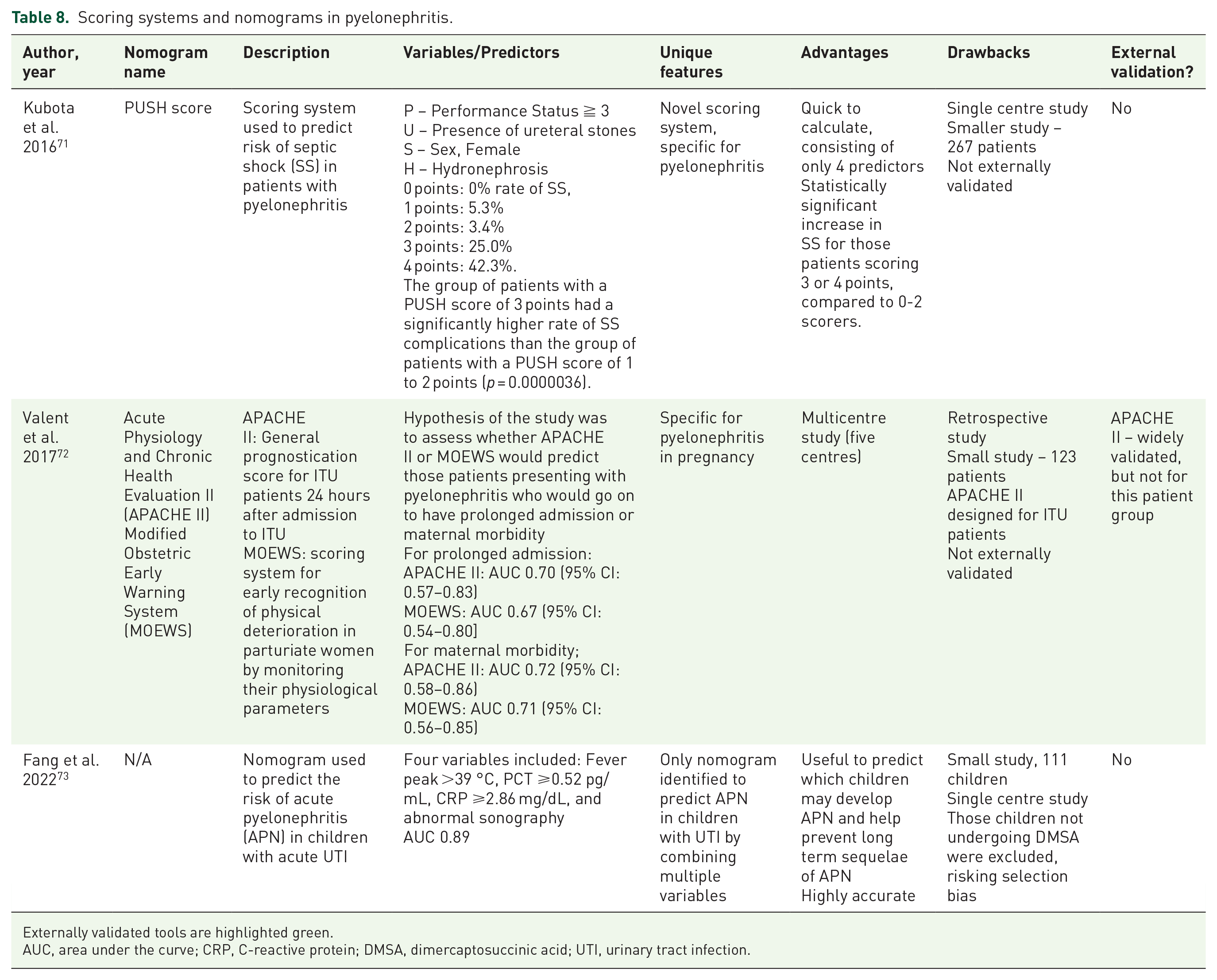
Externally validated tools are highlighted green.
AUC, area under the curve; CRP, C-reactive protein; DMSA, dimercaptosuccinic acid; UTI, urinary tract infection.
Emphysematous pyelonephritis
Emphysematous pyelonephritis (EP) is a condition historically associated with a high mortality rate. As a result, scoring systems are frequently employed in its management to aid in prognostication. 74 We identified ten scoring systems used in EP, studied in six articles.75–79 These are summarised in Table 9.
Scoring systems and nomograms in EP.

Externally validated tools are highlighted green.
AUC, area under the curve; EP, Emphysematous Pyelonephritis; qSOFA: Quick Sepsis-related Organ Failure Assessment score.
Stojadinović et al. 70 developed a scoring system consisting of only three variables to predict early treatment failure in EP. It showed excellent accuracy with an AUC of 0.944; however, this was a small study with 106 patients, that included patients with pyonephrosis also. In their 2019 paper, Jain et al. 74 developed another scoring system for EP patients, this time a prognostic scoring system. Ten variables were included and a total score out of 10 was used to classify patients into favourable, intermediate, and poor prognosis groups. There was no multivariate analysis or AUC/C-index calculation, and this was a score developed from only 72 patients. Similarly, Prakash et al. 76 developed the “Stanley scoring system,” consisting of five variables valued at one point each, including shock, hypoalbuminaemia, bacteraemia, thrombocytopenia and need for haemodialysis. They found that scores of four or more were associated with poor outcomes, defined as death or recurrent EP (sensitivity 95.45% specificity 98.43%, positive predictive value 95.45% negative predictive value 98.43%). This was a small study of 128 patients, and there was no AUC/C-index calculation. Krishnamoorthy et al. 77 reported their prognostic scoring system for EP in 2021. This is an 18-point scoring system that allows for risk stratification of patients. Of note, on multivariate analysis, no single factor was found to be statistically significant, there was also no AUC/C-index calculation.
Published in 2022, the GREMP study by Trujillo-Santamaria et al. 78 reported on the multi-centre study of 570 patients. They developed a scoring system consisting of six variables, with a maximum score of seven. The mortality rate was low in patients with a score of ⩽3 (<5%), increased with a score ⩾4, reaching 83.3% mortality with a score of 6 and 100% with a score of seven. It showed excellent accuracy with an AUC of 0.91 (95% CI, 0.84–0.97), and it has been externally validated. This score had a rigorous development process and is highly accurate. The most recent study identified assessing scoring systems in EP was that of Bibi et al. 79 They evaluated the performance of five scoring systems (qSOFA, modified early warning score (MEWS), National Early Warning Score (NEWS), systemic inflammatory response syndrome and the global research in emphysematous pyelonephritis group (GREMP) score) in their ability to predict intensive care unit admission in patients with EP. All five scores showed high levels of accuracy to predict ICU admission with AUC 0.915, 0.895, 0.968, 0.887, and 0.846 for qSOFA, Modified Early Warning Score (MEWS), NEWS, systemic inflammatory response syndrome criteria (SIRS), and GREMP score, respectively. NEWS score was seen to be most accurate, confirming the results from Chawla et al. in 2022. 77 It should be noted that this was as small study involving only 70 patients.
Emphysematous cystitis
We identified two scoring systems that were used in patients with emphysematous cystitis, these were both studied by Chen et al. in 2023. 82 These are summarised in Table 10. In this retrospective observational study, they compared the performance of two scoring systems: the Mortality in Emergency Department Sepsis (MEDS) score and Rapid Emergency Medicine Score (REMS). These are both validated scoring systems used in infections, with this article being the first use in emphysematous cystitis patients specifically. The AUC for MEDS was 0.819 for a cut-off point of 12 points and 0.685 for REMS with a cut-off point of 10 points. This shows the higher accuracy for the MEDS, however, this was a retrospective observational study of a small cohort of 35 patients.
Scoring systems and nomograms in emphysematous cystitis.

Externally validated tools are highlighted green.
AUC, area under the curve; GCS, Glasgow Coma Scale.
Fournier’s gangrene
We identified eight studies assessing nine scoring systems used in patients with Fournier’s gangrene (FG).83–89 These are summarised in Table 11. As in EP, FG is a condition that carries a high mortality rate 87 and as such, scoring systems are often used for prognostication. The first scoring system developed was the Fournier’s gangrene severity index (FGSI). This was developed by Laor et al. 83 in 1995. With a cut-off of nine, there was a 75% probability of death, nine or less was associated with a 78% probability of survival (p = 0.008). This score has been externally validated and also used to develop later scores. It shows excellent accuracy in validation studies. One such score that was developed from the FGSI was the Uludag Fournier’s gangrene severity index (UFGSI) developed by Yilmazlar et al. 84 in 2010. This score uses the same parameters as the FGSI but adds age of patient and extent of gangrene to produce the new score with 11 parameters. In this study, they found the UFGSI to be highly accurate when a cut off score of nine was applied, with an AUC of 0.947. Further, they found that the UFGSI was more accurate than the FGSI (p = 0.002). This was a small study involving 80 patients, but the UFGSI has been externally validated. The main drawback of the score is the subjective nature of classifying the extent of the FG.
Scoring systems and nomograms in FG.
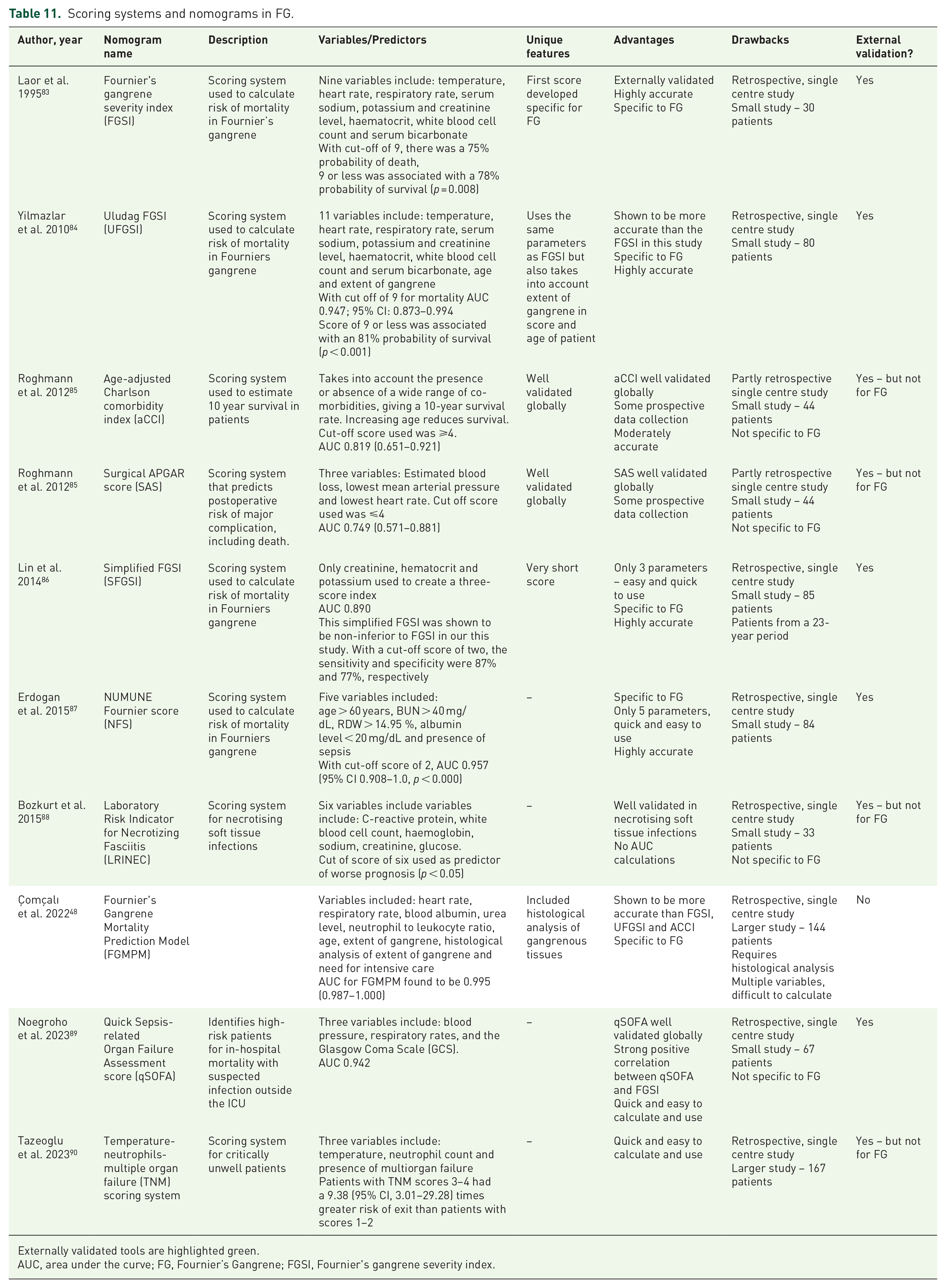
Externally validated tools are highlighted green.
AUC, area under the curve; FG, Fournier’s Gangrene; FGSI, Fournier’s gangrene severity index.
In their 2012 study, Roghmann et al. 85 assessed the performance of the age-adjusted Charlson comorbidity index (aCCI) and the surgical APGAR score (SAS) against the FGSI and UFGSI. Concerning the aCCI, which is a generic scoring system that takes into account patients’ age and comorbidities to produce a 10-year mortality risk, this was shown to be accurate in FG patients with an AUC of 0.819 (0.651–0.921). The SAS is a scoring system consisting of three parameters used to calculate postoperative risk of death. In this study, it was shown to be less accurate than the aCCI, FGSI and UFGSI with an AUC of 0.749 (0.571–0.881). Overall, there was no significant difference between the performance of the scoring systems in this partly prospective study of 44 patients.
Another scoring system developed from the FGSI is the Simplified FGSI (SFGSI), developed by Lin et al. 86 In this study, the parameters in the FGSI were assessed and the variables haematocrit, creatinine and potassium were found to be statistically significant. When these variables were used, the AUC was found to be 0.890, and the simplified FGSI was found to be non-inferior to the FGSI. The score has been externally validated.
In 2015, Erdogan et al. 87 developed their score, the Numune Fournier score (NFS). The NFS consists of five variables, so is quick to calculate. With cut-off score of 2, the AUC was 0.957 (95% CI 0.908–1.0, p < 0.000) with a sensitivity of 95.1%, indicating excellent accuracy. The score has been externally validated, with this study finding accuracy with an AUC of 0.823. 91 Bozkurt et al. 88 assessed the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score, a scoring system validated for use in necrotising soft tissue infections. They found that a cut-off score of six used as predictor of worse prognosis (p < 0.05); however, there was no AUC calculation done in this study and the LRINEC is not specific to Fournier’s gangrene.
In 2022, Çomçalı et al. 48 developed, through logarithmic regression, the Fournier’s Gangrene Mortality Prediction Model (FGMPM). They compared the strengths of the FGSI, UFGSI and aCCI and the newly developed model was reported to have high levels of accuracy, with an AUC of 0.995, more accurate than the FGSO, UFGSI and aCCI. This was with the largest cohort seen in the literature, of 144 patients. Of note, a variable in the score is that of histological analysis of the tissue, which would be extremely difficult to obtain given the rapid onset of the condition. Noegroho et al. 89 assessed the performance of the quick sepsis-related organ failure assessment score (qSOFA). This is a well-established score that is extremely quick and easy to calculate. It was shown to be highly accurate in FG patients with an AUC 0.942. It has been externally validated. Lastly, Tazeoglu et al., in 2023, 90 reported on the Temperature-Neutrophils-Multiple Organ Failure (TNM) scoring system in FG patients, a relatively new scoring system used to evaluate critically unwell patients. This score consists of three variables and as such, is very quick and easy to calculate. They found that patients with TNM scores 3–4 had a 9.38 (95% CI, 3.01–29.28) times greater risk of exit than patients with scores 1–2.
Epididymitis
Only one nomogram was identified for epididymitis, developed by Liu et al. in 2023, 92 this is shown in Table 12. This diagnostic nomogram was developed to differentiate epididymal tuberculosis (TB) from bacterial epididymitis. It was shown to be accurate with a C-index of 0.98.
Scoring systems and nomograms in epididymitis.
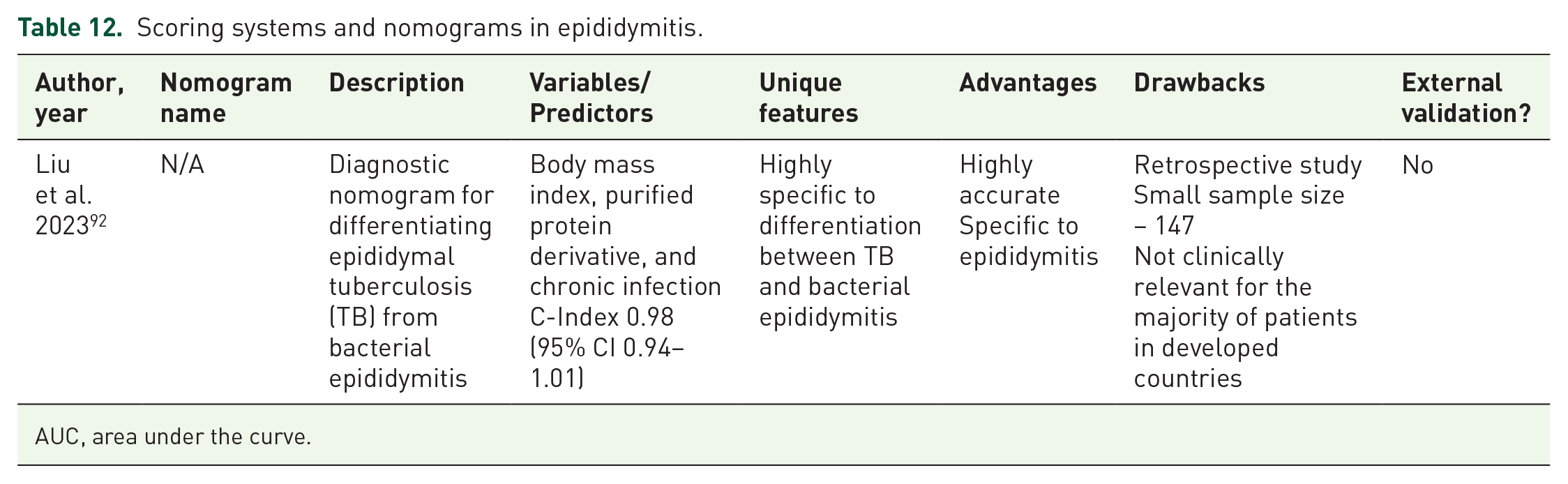
AUC, area under the curve.
Discussion
Given the subjective nature of PROMs, which can often involve complex topics, the development of an effective PROM is difficult and requires the acquisition of a large volume of qualitative data from relevant sources prior to development. 11 All items in a PROM should be relevant for the issue being assessed and the PROM should consider all concerns relevant to the patient, whilst concomitantly being understood by the patient. 12 Several guidelines concerning the development and evaluation of PROMs have been developed, including the consensus-based standards for the selection of health measurement instruments (COSMIN) guidelines, 12 which aim to ensure PROMs are effective tools for gathering such data. Concurrently, there have been concerns raised regarding diversity, inclusion and equity in PROMs, with calls to ensure that PROMs are developed by taking into account a range of populations and developed to be accessible and suitable for all patients. 15 In this atlas, we provide the first overview of the different PROMs used in UTIs and allied conditions. We have not carried out formal analysis of the available PROMs using a validated tool such as the COSMIN methodology, as this was felt to be beyond the scope of this article. This study is designed to provide a comprehensive overview of the literature, with the PROMS that can be utilised in UTI available in one place for the clinician managing patients with UTI.
PROMs have significant utility in the management of patients with UTI. As part of a general shift in medicine towards greater consideration of the impact of disease on patients’ QoL, these allow an opportunity for clinicians to understand this effect. Most are easy for patients to complete and would be easily transferrable to a digital form for patients to complete on a smartphone whilst waiting for an appointment, for example. Further, specific to rUTI, there are now a plethora of available treatments ranging from conservative to intravesical therapies. By better understanding the effect of recurrent UTI on patients’ QoL, this will allow clinicians to better empathise with patients and make decisions in partnership, perhaps with a view to initiating more, or less, invasive therapies depending on the severity of the rUTI on the patient’s QoL. Following treatment of acute and recurrent UTI, the use of a validated PROM will allow clinicians to track the effect of this on the patient’s QoL and symptoms in an objective manner.
There are a plethora of scoring systems and nomograms available to the modern-day clinician, it is vital that the tool that is used is suitable for the patient being treated. Scoring systems concerning urolithiasis and urosepsis were not included in this overview. There were no other scoring systems or PROMs identified in the literature regarding UTIs. We have seen in this review, the large number of scoring systems and nomograms available for patients with UTI. For less severe UTI, nomograms seem to take precedence. The use of nomograms to calculate the risk of ESBL positive UTI56,60 gives a perfect example of the use of patient data to help predict the risk of MDR organisms, which is of great concern to modern medicine. Further, as there is often uncertainty in the diagnosis of UTI, nomograms can help to more accurately and confidently diagnose UTI. Li et al. 59 developed a highly accurate nomogram for predicting the risk of UTI in children under the age of 3, we hope that further accurate nomograms can be developed for the wider population. Scoring systems tended to be used for more severe UTI as they are typically used in prognostication, allowing clinicians to assess the severity of a UTI, which plays a crucial role in the management of patients. Alongside clinical judgement, the generation of an objective score as to the severity of a UTI better informs the clinician when deciding on level of management of patients, for example, early referral to intensive or critical care departments. Further, as can be the case in Fournier’s gangrene, there can be a significant risk of mortality, which can be difficult to quantify. With the use of scoring systems, this helps the clinician not only in the management of the patient but also in prognostication, which is needed during discussions with the patient and their relatives. It is vital that the accuracy of these scoring systems is assessed and the systems externally validated. We have reported on the available nomograms and scoring systems being used in UTI, as well as their reported accuracy and whether they have been externally validated.
Future directions
With the ongoing incorporation of artificial intelligence (AI) into medicine, as well as the ongoing digitisation, collection and analysis of health-related data, this provides fascinating and exciting opportunities to utilise PROMs. Work is being done to integrate PROMs into AI health-care technologies, which hopes to ensure that outcomes important to patients are included in such technologies. 93 Another interesting avenue for collection of this data is that of social media-based surveys such as that carried out by Gonzalez et al. in 2022. 94 In an increasingly technological, online world, social media provides rapid access to patients, whilst in the comfort of their own environment, away from the healthcare setting. Further analysis of PROMs using structured guidelines such as COSMIN is vital to ensure that the available PROMs are effective tools for clinicians and researchers. Further, agreement in governing bodies as to which PROM, nomogram or scoring system is most appropriate for each type of UTI could ensure standardisation across clinicians.
Conclusion
PROMs are useful tools and have utility within the management of patients with UTIs. Scoring systems can help in prognostication and have been used predominantly in patients with more severe urinary infections. This atlas allows clinicians access to a single point of reference for the wide range of PROMs, scoring systems and nomograms used in the management of UTIs. It is the first study to do so. By reporting on the type of tool, presence of external validation and accuracy of these tools, this atlas will help clinicians decide on which tools will be most helpful to each specific patient. However, further clarity is needed as to which of these tools is most appropriate for each type of UTI as each of these offers their own respective advantages and disadvantages. Formal analysis of all PROMs used in UTI using guidance such as that of COSMIN was outside the scope of this review, but future work using such frameworks to further analyse each PROM will help to clarify which PROMs are most useful for each type of UTI. Lastly, the increasing use of PROMs in healthcare and the integration of these into AI healthcare technologies provides an important tool in ensuring that consideration of patient wellbeing is incorporated in such technologies, as well as providing an exciting avenue for future research.
Supplemental Material
sj-docx-1-tai-10.1177_20499361251328258 – Supplemental material for Atlas of patient-reported outcome measures, nomograms and scoring systems used in simple and complicated urinary tract infections: a systematic review
Supplemental material, sj-docx-1-tai-10.1177_20499361251328258 for Atlas of patient-reported outcome measures, nomograms and scoring systems used in simple and complicated urinary tract infections: a systematic review by Nicholas L. Harrison, Arthur W. Day, Zafer Tandogdu, Gernot Bonkat and Bhaskar K. Somani in Therapeutic Advances in Infectious Disease
Footnotes
Appendix 1 – Search terms
“urinary tract infection” OR “UTI” OR “acute urinary tract infection” OR “uncomplicated lower urinary tract infection” OR “complicated urinary tract infection” OR “acute lower urinary tract infection” OR “recurrent urinary tract infection” OR “cystitis” OR “acute cystitis” OR “recurrent cystitis” OR “urinary symptom*” OR “upper urinary tract infection” OR “pyelonephritis” OR “prostatitis” OR “urethritis” OR “epididymitis” OR “epididymoorchitis” OR “epididymo-orchitis” OR “orchitis” OR “urosepsis” OR “fourniers gangrene” OR “emphysematous pyelonephritis” AND “Patient Reported Outcome Measures”[Mesh] OR “Quality of Life”[Mesh] OR “patient reported outcome measure*” OR “prom” OR “pro” OR “quality of life” OR “health index” OR “health indices” OR “scoring system*” OR “nomogram” OR “grading tool*”
Acknowledgements
None.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.