
Abstract
Objective
To investigate the correlation between the ABO blood group and the risk of recurrent catheter-associated urinary tract infections (CA-UTI) and multi-drug resistant (MDR) organism reinfection in the critically ill.
Methods
This retrospective cohort study enrolled adult patients admitted to the intensive care unit (ICU) with confirmed CA-UTI to investigate the correlation between ABO type and the susceptibility to recurrent, reinfection and MDR reinfection. Patients were classified into two groups based on ABO type (O blood group versus non-O blood group).
Results
A total of 81 patients were included in the study: 37 in the O blood group and 44 in the non-O blood group. Patients in the O blood group were associated with significantly lower odds of recurrent CA-UTI (adjusted odds ratio 0.28; 95% confidence interval 0.08, 0.95), a shorter ICU length of stay (LOS) (estimate [SE] –0.24 [0.05]), hospital LOS (estimate [SE] –0.15 [0.03]) and mechanical ventilation duration (estimate [SE] –0.41 [0.07]) compared with the non-O blood group type.
Conclusion
Non-O blood group type might be a risk factor for recurrent CA-UTI and infection with MDR organism.
Keywords
Introduction
Catheter-associated urinary tract infections (CA-UTI) are considered one of the most common hospital-acquired infections. 1 Up to 80% of hospital-acquired urinary tract infections (UTI) are attributable to urinary catheterization. 2 The daily risk of acquiring bacteriuria secondary to urinary catheterization varies from 3% to 7%. 1 Of those with bacteriuria, up to 25% of patients become symptomatic. 3 Escherichia coli and Candida species are the most common prevalent organisms causing CA-UTI, followed by Enterococcus species, Pseudomonas species, Klebsiella species and Staphylococcus aureus. 4,5
Several risk factors associated with CA-UTI acquisition have been identified. 6,7 Catheterization duration is one of the most important risk factors and other risk factors include older age, female sex, colonization of the drainage bag with bacteria and diabetes mellitus. 6,7 Several studies show that CA-UTI is associated with increased mortality rates and prolonged length of stay (LOS). 8,9
The relationship between the ABO blood group and the susceptibility to certain infectious diseases is well documented. 10 –14 The blood group antigens are unique markers on the surface of red blood cell (RBC) membranes that determine the blood group type. These antigens are also present on body fluids and tissue cells, including urothelial tissue. Antigens consist of carbohydrate molecules that have roles in the membrane transportation of molecules, acting as receptors for extracellular ligands and enzymes, cell membrane integrity, and cell adhesion. ABO antigens have similar functions on epithelial cells, and RBCs. 15,16 Adherence to solid substrates is a property common to many pathogenic microorganisms (e.g. viruses, bacteria, yeasts and protozoa) that allows them to attach to host structures, which is considered necessary as it is the first step in the colonization of host mucosal surfaces. Microbial pathogens avoid being swept along by the normal flow of body fluids (blood, urine, intestinal contents) and eliminated, which leads to invasive infection in many situations. 17 –20
The wide use of the indwelling urinary catheters for patients admitted to the intensive care unit (ICU) has made CA-UTI the most common healthcare-associated infection in the ICU. 21,22 Thus, the prevention of CA-UTI is challenging in critically ill patients. These patients are highly susceptible to CA-UTI and recurrence. It is known that ABO antigens on the extracellular surface of RBC membranes may influence patient susceptibility to several different pathogens. 23 A few studies have suggested a slightly decreased risk of infection in patients with blood group O when compared with non-O. 24,25 The evidence about the relationship between ABO blood types and the risk of CA-UTI recurrence remains scarce. Therefore, this study investigates the correlation between blood group type (O-group versus non-O group) and the risk of recurrent CA-UTI, CA-UTI reinfection and multi-drug resistant (MDR) reinfection in critically ill patients with an indwelling urinary catheter.
Patients and methods
Study design and participants
This retrospective cohort study enrolled consecutive critically ill patients in the adult medical, surgical, trauma and burn ICUs at King Abdulaziz Medical City, Riyadh, Saudi Arabia between 1 January 2018 and 31 December 2018. The ICUs admit medical, surgical, trauma and burn patients and operate as closed units with 71 ICU bed capacity with 24/7 onsite coverage by critical care board-certified intensivists. Patients were enrolled in the study if they were critically ill patients aged ≥16 years with known ABO group type and confirmed CA-UTI within ICU admission. The exclusion criteria were as follows: (i) patients that were using immunosuppressive medication(s); (ii) immunocompromised patients; (iii) patients receiving inappropriate antibiotic(s) dosing; (iv) patients with a duration within 72 h of a positive culture (using Micromedex® database); (v) patients with previous admissions or antibiotic use within 3 months of admission; (vi) patients with repeated urinary catheter culture within 3 days that was negative without any new antibiotic initiation (s); (vii) sampling from the catheter collection system (e.g. catheter bag), urine culture <100 000 CFU/ml or more than two species of microorganism isolated.
The study hypothesized that patients with blood type O might be at a lower risk of CA-UTI recurrence and complications than non-O groups. Patients were categorized into two groups based on their blood group type since earlier studies suggested that patients with blood type O have a lower risk of infection than those with non-O blood types (O group versus non-O group). All patients were followed until they were discharged from the hospital or died during their hospital stay.
This study was approved in May 2019 by King Abdullah International Medical Research Centre – Institutional Review Board, Riyadh, Saudi Arabia (no. RC20. 587.R). The reporting of this study followed the STROBE guideline. 26 The confidentiality of the study participants was strictly observed throughout the study by using anonymous unique serial numbers for each patient and restricting access to the data to the investigators alone. Informed consent was not required due to the retrospective nature of the study as per the policy of the governmental and local research centre.
Data collection and definitions
Demographic and clinical data, including age, sex, weight, body mass index, associated comorbidities, laboratory baseline, ABO and rhesus blood group types, urine output (the amount of urine produced in ml/kg per h) and renal function within 24 h of ICU admission were collected from an electronic record system (Best Care System). Additionally, Glasgow Coma Scale, Acute Physiology and Chronic Health Evaluation (APACHE II) score, Sequential Organ Failure Assessment score and Nutrition Risk in Critically ill score were recorded for eligible patients on the first day. Urinary culture(s), recurrent, reinfection and MDR reinfection CA-UTI, antibiotic dosing and duration, ICU admission date, ICU discharge date, ICU mortality within 30 days, mechanical ventilation duration and history of admission, surgery, or dialysis within 3 months of ICU admission were reviewed and recorded. Patients with latex allergies or those expected to remain on a urinary catheter for a long time were switched to silicone catheters.
Asymptomatic CA-UTI is defined by the Infectious Diseases Society of America (IDSA) as a culture growth of ≥100 000 CFU/ml of uropathogenic bacteria in asymptomatic patients with urinary catheterization (e.g. indwelling urethral, indwelling suprapubic or intermittent catheterization). 17 In contrast, symptomatic CA-UTI is defined by the IDSA as culture growth of ≥10 000 CFU/ml of uropathogenic bacteria in the presence of symptoms or signs compatible with a UTI. 17 CA-UTI reinfection was defined as a UTI occurring more than 14 days after the original CA-UTI with a different organism. The recurrence of CA-UTI was defined as a UTI by the same organism that caused the primary infection. According to the US Centers for Disease Control and Prevention, MDR was defined as microorganisms that are resistant to one or more classes of antimicrobial agents. 27
Clinical outcomes
The primary outcome was the correlation between O-group types (O+ and O–) versus non-O group types (A+, A–, B+, B–, AB+, AB–) and the risk of having recurrent CA-UTI in critically ill patients. Secondary outcomes were CA-UTI reinfection, MDR reinfection, ICU LOS, hospital LOS, mechanical ventilation (MV) duration and ICU mortality.
Statistical analyses
Collected data were entered into Microsoft® Excel® 2010 (Microsoft Corporation, Redmond, WA, USA) after being coded as a master list. No identifiable information, such as patient name and medical record number, was recorded in the list. The analytical data set was then de-identified. This study considered two groups: patients with O group types versus patients with non-O group types.
All statistical analyses were performed using the SAS statistical package, version 9.4 (SAS Institute Inc., Cary, NC, USA). The categorical data are presented as n (%) and the continuous data are presented as mean ± SD. The denominator for the percentage (%) calculations was based on the actual observation of outcomes. The normality assumptions were assessed for all continuous data using statistical tests (i.e. Shapiro–Wilk test) and graphical representation (i.e. histograms and Q-Q plots). The categorical data were compared using χ2-test or Fisher’s exact test. Normally distributed continuous data were compared using Student’s t-test and other continuous variables that were not normally distributed were compared using Mann–Whitney U-test (Wilcoxon rank sum test). Baseline characteristics, baseline severity and outcome variables were compared between the two groups. Multivariate logistic regression and generalized linear regression analyses were used to determine the relationship between blood groups and the different outcomes considered in this study, after adjusting for the patient's baseline APACHE II score. The odds ratios (OR) and 95% confidence intervals (CI) were reported for the associations. A P-value <0.05 was considered statistically significant.
Results
This retrospective cohort study screened 1730 patients, of which 203 were found to have confirmed CA-UTI. Of these, 122 patients had confirmed CA-UTI but did not meet the eligibility criteria. The remaining 81 patients were included in the study, of which 37 (45.7%) were in the O blood group and 44 patients (54.3%) were in the non-O blood group. In the non-O blood group, most patients were A+ (22 of 44 patients; 50.0%) followed by B+ (15 of 44 patients; 34.1%).
Table 1 presents the baseline demographic and clinical characteristics of the O blood and non-O blood groups. There were no significant differences between the two groups in terms of the baseline demographic and clinical characteristics except for albumin level, which was significantly lower in the non-O blood group (P = 0.0223). The most common CA-UTI organisms in the O blood group were E. coli (13 of 37 patients; 35.1%) followed by Candida species (12 of 37 patients; 32.4%) and Klebsiella (12 of 37 patients; 32.4%) (Table 2). Whereas, in the non-O blood group, the most common CA-UTI organisms were Candida (10 of 44 patients; 22.7%) followed by E. coli (eight of 44 patients; 18.2%).
Baseline demographic and clinical characteristics of patients with confirmed catheter-associated urinary tract infections and admitted to the intensive care unit (ICU) stratified into O blood and non-O blood groups.
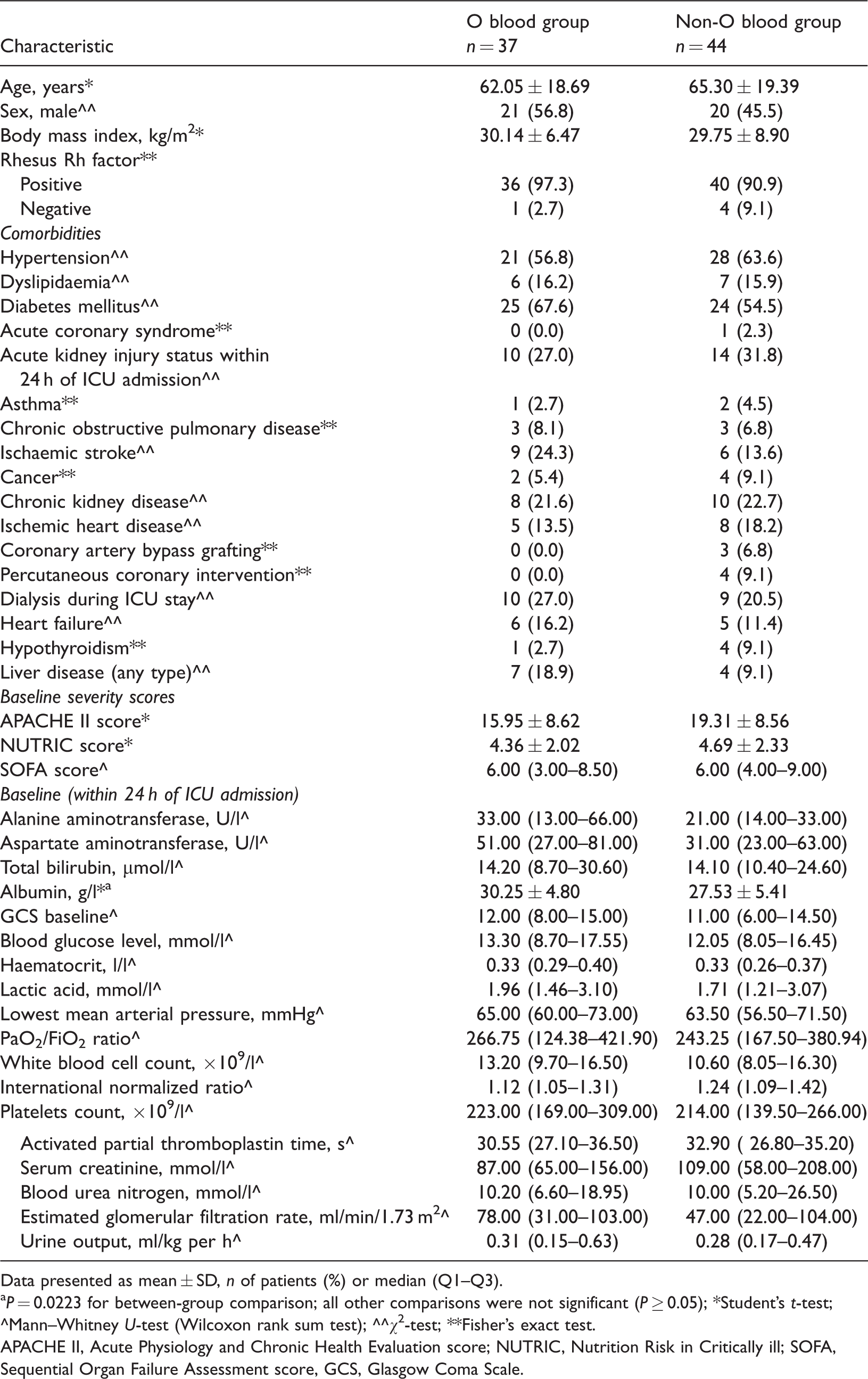
Data presented as mean ± SD, n of patients (%) or median (Q1–Q3).
aP = 0.0223 for between-group comparison; all other comparisons were not significant (P ≥ 0.05); *Student’s t-test; ^Mann–Whitney U-test (Wilcoxon rank sum test); ^^χ2-test; **Fisher’s exact test.
APACHE II, Acute Physiology and Chronic Health Evaluation score; NUTRIC, Nutrition Risk in Critically ill; SOFA, Sequential Organ Failure Assessment score, GCS, Glasgow Coma Scale.
Comparison of the most common microorganisms causing catheter-associated urinary tract infections (CA-UTI) in patients with confirmed CA-UTI and admitted to the intensive care unit stratified into stratified into O blood and non-O blood groups.

Data presented as n of patients (%) for each organism.
In a crude analysis, more patients in the non-O blood group had recurrent infections than the O blood group (14 of 42 patients [33.3%] versus six of 35 patients [17.1%], respectively), but the difference was not significant (Table 3). The odds of getting at least one recurrent infection were 82% less in the O blood group than in the non-O blood group (adjusted OR 0.28; 95% CI 0.08, 0.95; P = 0.04). The CA-UTI reinfection rate was not significantly different between the two blood groups (adjusted OR 1.47; 95% CI 0.35, 6.05).
Comparison of the primary and secondary outcomes of patients with confirmed catheter-associated urinary tract infections (CA-UTI) and admitted to the intensive care unit (ICU) stratified into O blood and non-O blood groups.

Data presented n of patients (%) or median (Q1–Q3); the denominator for the percentage (%) calculations was based on the actual observation of outcomes as shown.
^Mann–Whitney U-test (Wilcoxon rank sum test); ^^χ2-test; **Fisher’s exact test; $logistic regression was used to calculate odds ratio and P-value; $*generalized linear model was used to calculate estimates and P-value; $**model adjusted based on patient’s APACHE II severity score.
UOR, unadjusted odds ratio; CI, confidence interval; AOR, adjusted odds ratio; Ref, reference category; MDR, multi-drug resistant; APACHE II, Acute Physiology and Chronic Health Evaluation score; NS, not significant (P ≥ 0.05).
There were four of 11 patients (36.4%) with MDR organisms in the O blood group compared with 15 of 21 patients (71.4%) in the non-O blood group, which was significantly different in a crude analysis (P = 0.03) (Table 3). However, the differences between the two groups were not significant in the regression analysis (adjusted OR 0.21; 95% CI 0.03, 1.23).
Patients in the O blood group had a median ICU LOS of 17 days as compared with 23.5 days in the non-O group (Table 3). In the regression analysis, compared with the non-O blood group, the O blood group had a significantly shorter ICU LOS (estimate [SE] –0.24 [0.05]; P < 0.001), hospital LOS (estimate [SE] –0.15 [0.03]; P < 0.001) and MV duration (estimate [SE] –0.41 [0.07]; P < 0.001). The ICU mortality was not significantly different between the two blood groups (adjusted OR 0.70; 95% CI 0.22, 2.26).
Discussion
Linking blood types to the occurrence of some diseases and infections is a new area of investigation. 12,28,29 Theories about the relationship between blood types and diseases developed from observations that the carbohydrates located on the cell membranes of RBCs play a crucial role acting as receptors for microorganisms; and the attractiveness of these receptors to bacteria, parasites and viruses varies with the different blood types. 30 –32 This current retrospective study has demonstrated a significant decrease in the odds of CA-UTI recurrence in critically ill patients with an O-blood group type compared with non-O blood group patients (adjusted OR 0.28; 95% CI 0.08, 0.95). In contrast, the odds of a CA-UTI reinfection was numerically higher in the O blood group than the non-O blood group, but it did not reach statistical significance (adjusted OR 1.47; 95% CI 0.35, 6.05). Since optimal antibiotic choice, dosing and duration directly affect treatment success and improve patient outcomes, 33 only the patients that received appropriate antibiotic therapy were included in the current study.
The rate of CA-UTI recurrence was higher in the non-O blood group compared with the O blood group (33.3% versus 17.1%, respectively). This current finding was consistent with a previous study in 307 patients that found that type A blood group patients have a higher predisposition to get UTI than other blood groups. 34 In critically ill patients, a previous prospective cohort study showed that patients with blood type A were independently associated with acute kidney injury (AKI) risk, a tendency to acquire infections and experience more severe sepsis than other blood group types. 35
Another comparative study observed a correlation between the Lewis blood-group phenotype and recurrent UTIs among women. 36 That previous study identified a relationship between recurrent UTI among Lewis blood-group non-secretor (Le[a + b–]) and recessive (Le[a–b–]) phenotypes. 36 Since the identification of these antigens, several studies, including adult and paediatric patients, have been published. 11,36 These studies suggested that the presence of the P2 secretor phenotype blood group protects against asymptomatic colonization of the urinary tract. 37 In addition, certain blood group phenotypes may help identify patients at risk of UTI. 11,36 This has been explained by the expression of a large amount of ABH and Lewis histo-blood group antigens in the epithelial lining of the urinary tracts. 11,36 It has been proposed that the expression of ABO, H, Lewis and secretor histo-blood group carbohydrates can affect the susceptibility and resistance to infections, including UTIs. 38 –41
In this current study, patients with an O-blood group type demonstrated a significantly shorter hospital LOS (47 days versus 56 days) and ICU LOS (17 days versus 23 days) compared with the non-O group. As it has been seen that in critically ill patients, patients with blood type A are associated with a higher risk of ICU complications, including infections and sepsis, this infection tendency and severity could contribute to a longer hospital LOS. 25,28 This current study demonstrated no significant difference in ICU mortality between the two groups. In contrast, a single-centre retrospective cohort study that enrolled 141 patients with severe burn injuries, demonstrated that patients with blood type O had increased mortality and AKI risk. 42
These current results demonstrated that the prevalence of MDR organisms was different between the two groups (P = 0.03). To the best of our knowledge, there are no previous publications reporting on MDR infection risk in relation to blood types, so this is the first study to examine the relationship between CA-UTI recurrence, CA-UTI reinfection and MDR rate with blood group type among ICU patients.
This current retrospective study has several limitations. First, the retrospective design and small sample size might limit the conclusions and findings of the relationship observed. Secondly, the length of ICU stay, MDR rate and CA-UTI reinfection could have been affected by other factors unrelated to blood group types, especially in the research population of critically ill patients. Finally, it is known that latex rubber catheters are associated with higher urinary catheter infections. However, the study could not assess the correlation between the catheter type and the clinical outcomes of interest. Further well-conducted studies with a larger sample size and different statistical analysis approaches (e.g. propensity score matching) are required to avoid potential bias and confirm these current findings.
In conclusion, non-O blood group type was associated with a higher risk of recurrent CA-UTI and infection with MDR organisms compared with O-blood group type in critically ill patients. Identifying patients at risk of CA-UTI recurrence may help determine the appropriate prophylaxis, including the best treatment options and duration. However, larger, extensive and well-conducted studies evaluating the correlation of CA-UTI infections, reinfection and infection severity with blood group types are needed to further clarify this correlation.
Footnotes
Acknowledgements
We would like to thank Princess Nourah bint Abdulrahman University Researchers Supporting Project (no. PNURSP2022R78), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia. In addition, we would like to acknowledge all of the investigators in the Saudi Critical Care Pharmacy Research (SCAPE) Platform that participated in this project.
Author contributions
All authors contributed to data collection and analysis; and drafting, revising and approving the final version of the manuscript. All authors agree to be fully accountable for ensuring the integrity and accuracy of the work.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This study was supported by a grant from the Princess Nourah bint Abdulrahman University Researchers Supporting Project (no. PNURSP2022R78), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.