
Abstract
Background:
Sepsis is one of the leading causes of morbidity and mortality worldwide. Early detection and reliable prediction of sepsis-related mortality are crucial. The prognostic value of National Early Warning Score 2 (NEWS-2) in sepsis patients with cardiovascular and neurovascular diseases is not well elucidated.
Objectives:
This study aims to evaluate and compare the qSOFA, SOFA, qPitt, and NEWS-2 scores for predicting mortality in sepsis and septic shock patients.
Design:
An observational retrospective study was conducted involving patients with sepsis or septic shock.
Methods:
Data were collected between 2023 and 2024. Baseline measures included sociodemographic and clinical characteristics. All subjects were identified from a database of a highly complex healthcare institution focused on the diagnosis and treatment of cardiovascular and neurovascular diseases. The scores qSOFA, SOFA, NEWS-2, and qPitt were collected from medical records and analyzed. A sample size was estimated. The area under the receiver operating characteristic curve (AUROC) analysis was established for each score. A multivariate analysis adjusted for confounding factors through logistic regression was performed.
Results:
A total of 126 participants were included, with a median age of 72 years (IQR: 59–81), and 76 (60.32%) being men. The overall mortality rate in the population was 19.8%, with 84% of deaths occurring in males. Statistically significant differences in variables such as heart failure, mild liver disease, and atrial fibrillation were observed between the groups (p < 0.05). The NEWS-2 score with a cut-off point of ⩾8 showed a significant association with mortality (p = 0.0001). The AUROC for NEWS-2 was 0.80, compared to a ROC of 0.6960 for qPitt, 0.6776 for SOFA, and 0.5868 for qSOFA (χ2 = 16.60, Prob > χ2 = 0.0009).
Conclusion:
NEWS 2 exhibits better performance in predicting mortality among elderly adults with cardiovascular and neurovascular diseases suffering from sepsis or septic shock, compared to the qPitt, SOFA, and qSOFA scores.
Plain language summary
Sepsis is a life-threatening condition that can lead to death, especially in people with heart or brain conditions. Quickly identifying patients at high risk of death is crucial for providing timely treatment. This study looked at different scoring tools used to predict the risk of death in patients with sepsis or septic shock who also have cardiovascular or neurovascular diseases. Researchers examined medical records of 126 patients, mostly elderly, treated between 2023 and 2024 at a specialized hospital. They compared four different scoring systems: NEWS-2, qSOFA, SOFA, and qPitt. These scores help doctors decide which patients are most at risk and need urgent care. The study found that the NEWS-2 score, particularly when it reached a certain threshold, was better at predicting the risk of death compared to the other scoring tools. This was especially true for older adults with sepsis and underlying heart or brain conditions. The findings suggest that using the NEWS-2 score could improve how quickly and accurately these high-risk patients are identified and treated.
Introduction
Sepsis constitutes a significant global health crisis. Annually, approximately 31 million people suffer sepsis, resulting in approximately 6 million deaths.1–3 Sepsis and septic shock cause millions of deaths worldwide each year and represent a significant global health burden. 3 Early detection and reliable prediction of sepsis-related mortality are crucial, as they facilitate timely intervention protocols.4–7
Several tools exist for activating a rapid response team.8–13 Scoring systems such as the National Early Warning Score (NEWS) 2 and the Pitt bacteremia score, along with its simplified version, qPitt ⩾ 4, have been validated for predicting mortality in sepsis patients.14,15 The most commonly used score is the sequential organ failure assessment (SOFA) score ⩾ 2, and its simplified version, the quick SOFA (qSOFA) ⩾ 2, which have proven to be useful tools in the early recognition and prognosis of these conditions and are recommended in worldwide guidelines.16–20 However, the SOFA and qSOFA scores, validated in 2016 for sepsis outside the ICU, have shown limitations in accurately predicting mortality.17,21 Similarly, the Pitt and qPitt scores were originally designed to predict mortality in bloodstream infections. However, they have since been validated for broader applications in other types of infections, though their accuracy in specific populations may not always be reliable.14,15
Specific clinical variables and their significance in sepsis are crucial, based on their behavior during the development of sepsis and septic shock. 22 The NEWS-2 score includes seven parameters, with more pulmonary variables compared to qSOFA. 23 The NEWS-2 uses a maximum of twenty points, with cut-off values of 0–4, 5–6, and ⩾7 used to indicate low, medium, and high risk, respectively. 24 Specific age groups and associated comorbidities complicate the detection and prognosis of patients with sepsis or septic shock.25,26 This study aims to evaluate and compare the qSOFA, SOFA, qPitt, and NEWS-2 scores for predicting mortality in sepsis patients within a specific population characterized by high complexity due to cardiovascular and neurovascular diseases.
Methods
A retrospective study was conducted involving patients with sepsis or septic shock between 2023 and 2024, hospitalized at the Fundación Clínica Shaio, which specializes in cardio and neurovascular diseases care in Bogotá, Colombia. Baseline sociodemographic and clinical characteristics were assessed, with data extracted from electronic medical records, and participants formed a consecutive series. Included patients were aged 18 years or older, hospitalized for more than 24 h, and met the criteria for sepsis defined as follows: diagnosis of infectious pathology by ICD-10 codes or use of antimicrobials or positive cultures, any organ dysfunction plus evaluation by two different medical services confirming the diagnosis of sepsis. Septic shock was defined as sepsis with persisting hypotension requiring vasopressors to maintain mean arterial pressure > 65 mm Hg and having a serum lactate level>2 mmol/L despite adequate volume resuscitation. Patients who presented with refractory shock upon admission (defined as a high risk of death within 24 h), pregnant patients, end-stage diseases, and those with concomitant acute respiratory distress syndrome (ARDS) were excluded. The scores qSOFA, SOFA, NEWS-2, and qPitt were collected from medical records.
Statistical analysis
Quantitative variables included in the study were described using means and standard deviations if the Shapiro-Wilk test indicated normal distribution. Otherwise, medians and interquartile ranges were reported. Qualitative variables were described using absolute frequencies and percentages.
Sample size was estimated for each score qSOFA, SOFA, NEWS-2, and qPitt, based on sensitivity and specificity, using equation comparison of proportions, 27 retaining the most demanding one. To handle missing data, we targeted an appropriate patient population, employed advanced data collection strategies (Figure 1), and incorporated an estimated level of missing data into the sample size calculation to maintain adequate statistical power despite potential losses of information. A subgroup analysis was performed for patients with cardiovascular diseases. The area under the curve (AUC) analysis was established for each score. The best AUC allowed the classification of subjects into two groups for the prediction of mortality, allowing a multivariate analysis adjusted for confounding factors through logistic regression. All analyses were performed using Stata 15 SE software (StataCorp LP, College Station, Texas, USA), using a two-tailed significance level of 0.05.
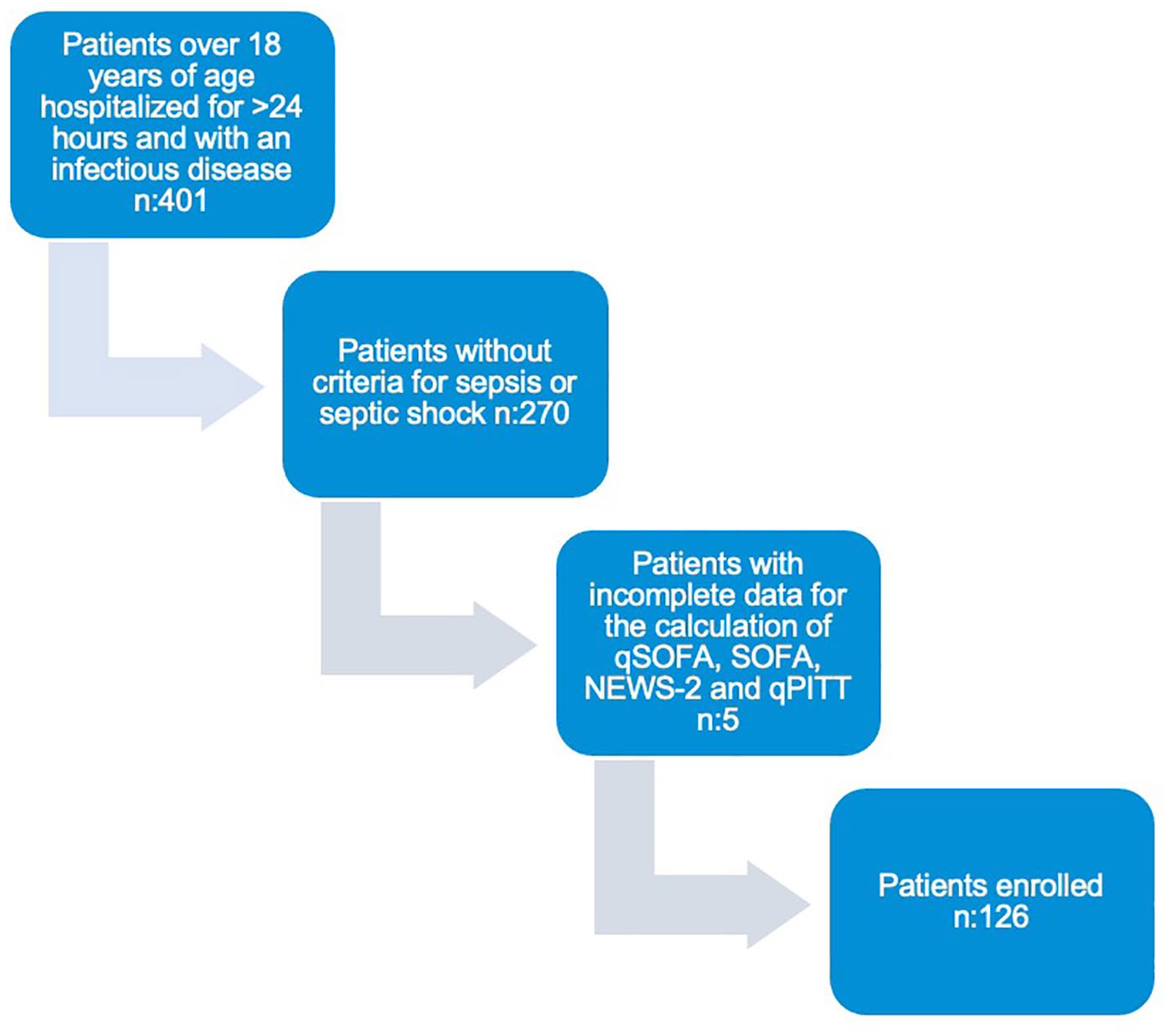
Flow diagram summarizing the patients eligible for the study.
Results
Out of 401 patients over 18 years of age hospitalized for more than 24 h with an infectious disease, 270 did not meet the criteria for sepsis or septic shock, and 5 had incomplete data for the calculation of qSOFA, SOFA, NEWS-2, and qPitt, resulting in a total of 126 patients enrolled (Figure 1).
Table 1 summarizes the sociodemographic and clinical characteristics of the study participants. The median age of the participants was 72 years (IQR: 59–81), with 76 participants (60.32%) being men. Over 60% of the participants had hypertension, 47.6% had heart failure, 32.5% had a history of myocardial infarction, and 11.9% had experienced an ischemic stroke or a transient ischemic attack. Analysis of clinical variables revealed significant associations with hospital mortality. These included low pulse oximetry saturation (SpO₂) (p = 0.001), the need for supplemental oxygen (p = 0.040), altered consciousness (p < 0.001), an average Glasgow Coma Scale score of 11 points (p = 0.003), the requirement for vasopressor support (p = 0.001), and the need for renal replacement therapy (RRT) (p = 0.043).
Sociodemographic and clinical characteristics of people with sepsis or septic shock.

Differences calculated using the Wilcoxon rank-sum test.
Differences calculated using Pearson’s χ2 test.
Differences calculated using Fisher’s exact test.
Differences calculated using Pearson’s χ2 test.
BMI, body mass index; CCI, Charlson Comorbidity Index; COPD, chronic obstructive pulmonary disease; IQR, interquartile range; RRT, renal replacement therapy; SpO2, peripheral oxygen saturation; TIA, transient ischemic attack.
The overall mortality rate in the population was 19.8%, with 84% of deaths occurring in males. Septic shock developed in 67 patients (53.1%), and the mortality rate among these patients was 32.8%. Statistically significant differences in variables such as heart failure, mild liver disease, and atrial fibrillation were observed between the groups (p < 0.05).
The most commonly used vasopressor was Noradrenaline at 68%, with Vasopressin as the second-line option at 22% (p = 0.001). Secondary outcomes, including length of hospital and ICU stay, ICU admission and readmission, use of invasive mechanical ventilation, and bleeding complications, are provided in Supplemental Data 1. Additional details, such as laboratory test results, etiology of shock, and cultures, are also provided in Supplemental Data 2 and 3. Mortality and its characteristics are shown in Supplemental Data 4 and 5.
Regarding the scores, a median NEWS-2 score of 8 (IQR 7–10) in the mortality group versus 6 (IQR 4–7) in the survivor group (p = 0.0001) better discriminates mortality in septic patients with statistical significance. In contrast, other scores such as qSOFA, with a median score of 2 (IQR 2–2) in both groups (p = 0.1268), SOFA with a median score of 6 (IQR 5–9) versus 5 (IQR 3–7) (p = 0.006) and qPitt with a median score of 3 (IQR 2–3) versus 2 (IQR 2–3) (p = 0.0013), did not show clinical or significant differences (Table 2).
Scores tested in sepsis and septic shock patients.

Differences calculated using the Wilcoxon rank-sum test.
IQR, interquartile range; NEWS, National Early Warning Score; qPITT, quick Pitt bacteremia score; qSOFA, quick Sepsis-Related Organ Failure Assessment; SOFA, Sepsis-Related Organ Failure Assessment.
The NEWS-2 score with a cut-off point of ⩾8 showed a significant association with mortality (p = 0.0001). In the multivariate model, adjusted for potential confounding variables such as sex, history of heart failure, RRT, and PaO2/FiO2 ratio, the NEWS-2 score had an odds ratio (OR) of 10.14 (CI: 2.92–35.17) (p = 0.0001) (see Table 3).
Association between the NEWS-2 score and mortality in sepsis or septic shock patients.

Adjusted for the variables: sex, history of heart failure, requirement for renal replacement therapy, and PaO2/FiO2.
OR, odds ratio.
The AUROC for NEWS-2 was 0.800 (95% CI, 0.7170–0.884). The AUROC for the other scores showed lower performance: qPitt with an AUROC of 0.6960 (95% CI, 0.601–0.790), SOFA with an AUROC of 0.6776 (95% CI, 0.562–0.792), and finally qSOFA AUROC of 0.5868 (95% CI, 0.478–0.694) (χ2 = 16.60, Prob > χ2 = 0.0009) (Figure 2).

Comparison of the area under the curve for NEWS-2, qSOFA, and SOFA in predicting mortality in adults diagnosed with sepsis.
Discussion
In this study, the NEWS-2 demonstrated superior predictive ability for mortality in sepsis and septic shock among elderly patients with cardiovascular and neurovascular diseases, outperforming qSOFA, SOFA, and qPitt. Specifically, the association between the NEWS-2 score ⩾8 and mortality in adults with sepsis was significant. Mortality in the group with NEWS-2 scores ⩾8 was 8.25 times higher compared to those with scores < 8. After adjusting for confounding variables, mortality risk was 10.14 times higher for scores ⩾8.
In this population of elderly patients with specific comorbidities, the NEWS-2 score which includes more, easily measurable, and key physiological parameters compared to the other scores,28–30 demonstrates superior prognostic performance, moving us closer to precision medicine. In sepsis, the immune response triggers cytokine release, initiating an inflammatory cascade.31,32 This response is adaptive and aids in infection control. However, sepsis disrupts the balance between pro-inflammatory and anti-inflammatory mechanisms, leading to microvascular and organ dysfunction.31,32 This dysfunction manifests as changes in macro variables such as respiratory rate, low oxygen saturation (SaO2), systemic vasodilation, and capillary leakage, ultimately impacting blood pressure and perfusion. 33
Our findings showed that the pulmonary and brain systems are the most involved in sepsis patients, represented in the low SpO2 and the need for supplemental oxygen, the alteration of consciousness, or low Glasgow score as significant variables associated with mortality. In our population with cardiovascular and neurovascular diseases, the imbalance in oxygen delivery (DO2) and oxygen consumption (VO2) leads to loss of hemodynamic and respiratory coherence, clinically manifested as altered consciousness and desaturation. These variables were the most affected in patients who died, in contrast to hemodynamic variables found in other studies.34,35 In cardiovascular and elderly patients, fluid redistribution causes congestion and increases the renin-angiotensin system, resulting in high blood pressure.28,29 In addition, this population may have chronically low arterial pressure. 28 Therefore, systolic and mean arterial pressure might not be good variables for early detection and prognosis in sepsis or septic shock for this population.
Among the parameters evaluated in the qSOFA score, only the variable (altered mental status) showed significant differences between the two groups. In contrast, the SOFA score, which includes two respiratory parameters (PaO2/FiO2 ratio and the use of mechanical ventilation) and one central nervous system (CNS) parameter (Glasgow Coma Scale), demonstrated moderate predictive performance. The qPITT score, which incorporates one respiratory parameter (respiratory failure) and one CNS parameter (altered mental status), outperformed both the qSOFA and SOFA scores. Meanwhile, the NEWS 2 score, which encompasses three respiratory variables (respiratory rate, hypercapnic respiratory failure, and the need for supplemental oxygen) and one CNS-related variable (level of consciousness), demonstrated the most comprehensive assessment.
Considering that pulmonary and CNS dysfunction were the most significantly affected systems predicting mortality in our study, it is plausible that NEWS 2, by offering a broader assessment of these organ systems, demonstrates superior predictive performance.
Furthermore, disease progression to septic shock led to microcirculatory complications identified by classic markers of hypoperfusion,36,37 such as hyperlactatemia and acidosis, which were associated with increased mortality in this study. Shock, defined as an imbalance between DO2 and VO2, is likely in this population with brain and lung compromise.
Previous studies have highlighted the superiority of NEWS-2 in the early identification of sepsis patients and mortality prediction,18,35,38–41 and this study suggests it specifically for the cardiovascular and neurovascular populations. However, after the Third International Consensus Definition for Sepsis and Septic Shock (Sepsis-3) in 2016, qSOFA and SOFA remain used for the general population.5,17 Our findings highlight the need for precision medicine and the use of scores tailored to specific conditions and populations.
When interpreting this study, it is important to consider its limitations. These results must be validated prospectively in a larger cohort of patients. As a retrospective study, it relies on data available in electronic medical records, which may introduce biases. Another significant limitation is that it was conducted at a single hospital center, potentially restricting the generalizability of the findings to other populations or clinical settings. Applying scoring systems for early sepsis prognostication challenges sensitivity and specificity, limiting individual and dynamic adaptability. In the near future, biomarkers and genetics may be integrated to enhance prognostic accuracy in precision medicine.
Conclusion
NEWS-2 exhibits better performance in predicting mortality among elderly adults with cardiovascular and neurovascular diseases suffering from sepsis or septic shock, compared to the qPitt, SOFA, and qSOFA scores. These findings suggest that neither qSOFA nor SOFA should replace early warning scores based on clinically accessible parameters like NEWS-2 in this patient population.
Supplemental Material
sj-docx-1-tai-10.1177_20499361251323207 – Supplemental material for Prediction of mortality in cardio-neurovascular patients with sepsis and septic shock: is NEWS-2 better than qSOFA, SOFA, and qPitt? An observational study
Supplemental material, sj-docx-1-tai-10.1177_20499361251323207 for Prediction of mortality in cardio-neurovascular patients with sepsis and septic shock: is NEWS-2 better than qSOFA, SOFA, and qPitt? An observational study by Julian Orlando Casallas-Barrera, Darlyng Aireth Zabala-Muñoz, Carol Viviana Aponte-Carrascal, Angie Marcela Ochoa-Ricardo, Edgar Felipe Quintero-Varela, Juan Nicolas Quiñones-Romero, Jenny Paola Garzón-Ruiz, Edwin Silva-Monsalve and Ricardo Buitrago-Bernal in Therapeutic Advances in Infectious Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.