
Abstract
Background:
Vulvovaginal candidiasis and urinary tract infections caused by Candida are common diseases. While the most common causative agent is C. albicans, other species, such as non-C. albicans, can also be responsible. Susceptibility to antifungal drugs varies among Candida species, but there is very limited information available from Vietnam.
Objectives:
To determine the species distribution and antifungal susceptibility patterns of Candida isolated from urine and vaginal samples of patients tested at the Medlatec healthcare system in 2023.
Design:
Cross-sectional study.
Methods:
The study describes a cross-sectional analysis of over 102 Candida isolates obtained from urine and vaginal samples of patients using the testing services at Vietnam Medlatec healthcare system from January to December 2023. Species identification of Candida isolates was performed using germ tube test and Vitek® 2 systems. Antifungal susceptibility testing was carried out using the VITEK® 2 card for yeast fungi. Minimum inhibitory concentrations for these isolates were classified according to the Clinical and Laboratory Standards Institute guidelines (M27-A3 and M27M44S-ED3).
Results:
In this investigation, five different Candida species were identified. Among these isolates, C. albicans (78.43%) was the most frequent, followed by C. tropicalis (11.76%), C. glabrata (4.91%), C. parapsilosis (1.96%), and C. krusei (0.98%). The resistance rates to fluconazole, voriconazole, caspofungin, micafungin, and amphotericin B were 7.7%, 4.2%, 4.0%, 1.0% and 1.0%, respectively.
Conclusion:
The most common species found in this population was C. albicans. Our findings also showed a high frequency of non-albicans Candida species causing fungal urinary tract infections. The resistance rates of isolated Candida strains to echinocandins and amphotericin B were low, while some strains were found to be resistant to fluconazole and voriconazole.
Keywords
Introduction
Candida species are opportunistic fungal pathogens found as part of the microbial normal flora of the urogenital tract. The clinical presentations of infectious diseases caused by these pathogens depend on the site of infection. 1 Among healthy individuals, most cases of fungal urogenital tract infection are asymptomatic, and treatment is infrequently necessary.1–3 In symptomatic individuals, urogenital candidiasis is categorized into four main sections, vulvovaginal candidosis (VVC) in women, balanitis and balanoposthitis in men, and candiduria in both sexes. 1 These diseases occur in both immunocompetent and immunocompromized patients. VVC mostly appears in healthy, reproductive-age women, while candiduria is frequently observed in immunocompromized patients, intensive care unit (ICU) inpatients, or neonates.1,2,4 In the USA, it is estimated that there are more than one million cases of nosocomial urinary tract infections (UTIs) each year, with Candida spp. responsible for 10%–30% of these infections.5–8 Risk factors for VVC and UTI (urogenital candidiasis) include extremes of age, female sex, poorly controlled diabetes, prolonged hospitalization, ICU admission, immunodeficiency states, use of antibiotics, previous surgery (both urological and nonurological), radiation therapy, treatment with glucocorticoids and genetic predispositions, genitourinary tuberculosis, neutropenia, genitourinary tract instrumentation, organ transplantation, congenital or structural abnormalities of the urinary tract and catheterization, among others.1,8–12
Among the Candida species that cause urogenital candidiasis, Candida albicans is the predominant infectious agent. However, there has been an increasing frequency of non-albicans Candida (NAC) species such as C. glabrata, C. tropicalis, C. parapsilosis, and C. krusei reported worldwide.1,3–5 Epidemiological surveys have indicated that the incidence of non-C. albicans strains is gaining prominence in both VVC and candiduria.1,13,14 Previous studies also showed that NAC species are more commonly resistant to antifungal agents than C. albicans, particularly resistant to fluconazole.1,5,12–14 The rise in these NAC species and the development of resistance to antifungal drugs have become significant challenges for clinicians.5,15,16 Therefore, accurate isolation and identification of Candida species causing urogenital candidiasis, as well as antifungal susceptibility testing, are essential for guiding the selection of appropriate antifungal therapy.3,13
There have been many publications regarding the distribution and antifungal susceptibility of Candida causing VVC and candiduria from different countries around the world.3,17–23 However, there is very limited data on the distribution of Candida species causing VVC and UTI in Vietnam, especially among patients with UTI. Moreover, no studies have compared the species composition and antifungal susceptibility patterns of Candida isolates from VVC and UTI patients in Vietnam. Additionally, complicated VVC and UTI cases caused by NAC are often difficult to treat successfully because these species tend to be more resistant to antifungal agents.12,24,25 According to the literature, accurate identification and antifungal susceptibility testing of Candida species are of critical importance for therapeutic success.9,13,25 Therefore, this study aimed to determine the distribution of Candida species isolated from VVC and UTI patients in the Medlatec healthcare system in Hanoi city, Vietnam, as well as their susceptibilities to antifungal agents.
Methods
Study population
In this investigation, a cross-sectional study was conducted between January 2023 and December 2023 at the Medlatec Laboratory Center, part of the Vietnam Medlatec healthcare system. A total of 102 patients, aged between 18 and 93 years, with urogenital disorders, were selected from the Medlatec healthcare system in Hanoi city, Vietnam. Patients who were unmarried or used any systemic or topical antifungal therapy in the previous 7 days were excluded from the study.
Sampling, phenotypic identification of yeast species
The diagnosis of VVC was made by an obstetrician-gynecologist. A case of VVC was defined based on clinical symptoms such as vaginal discharge and vulvar itching, along with positive results for Candida spp. 17 The diagnosis of UTI was made by a urologist based on clinical symptoms such as dysuria, and pyuria, as well as positive yeast culture results on Sabouraud dextrose agar (SDA) plates supplemented with chloramphenicol (Lavitec Company, Vinh Phuc, Vietnam), with the presence of ⩾103 CFU/mL of yeast cells in urine.16,26,27 Urine and vaginal samples were collected from each participant to isolate yeasts. Trained nurses used sterile disposable collection bottles for urine samples and sterile cotton-tipped swabs for vaginal discharge samples. The collected samples were then shipped to the Medlatec Laboratory Center (Medlatec healthcare system) within 24 h for yeast isolation. Upon arrival, all urine and vaginal specimens were centrifuged to concentrate the urine samples and/or subjected to direct 10% KOH smear examination. They were also inoculated onto SDA plates supplemented with chloramphenicol at 35–37°C for 48 h to determine yeast infection. The SDA plates were examined daily for the presence of yeast. The presence of yeast was confirmed by observing budding yeast in 0.85% saline wet mount. SDA plates showing no growth after 48 h were further incubated for an additional 24 h. All positive yeast isolates were subcultured on SDA for germ tube tests, confirmation of yeast species, and antifungal susceptibility tests.
Differentiation of C. albicans from other yeast using germ tube test
The germ tube test was performed in a 1.5 mL Eppendorf tube containing 500 µL of human serum. Using a sterile inoculation loop, a colony of yeast was touched from the SDA and gently emulsified in the serum. The tube was then incubated at 37°C for 2 to 4 h. In the next step, a drop of the yeast-serum culture was transferred to a glass slide for examination under 10× and 40× magnification. A positive result, determined as C. albicans, was characterized by a short hypha with no nucleus, about half the width, and 3–4 times the length of the yeast cell, extending laterally from the yeast cell with no constriction at the point of origin. For quality control, C. albicans ATCC® 90028 was used as a reference strain.
Species identification of Candida spp. using VITEK 2 compact system
A suspension of the yeast isolate was prepared in 3 mL of sterile saline by picking five to six colonies with approximately 1 mm diameter from the SDA culture plate (24 h) of the Candida spp. species. These suspensions were adjusted to 0.5 McFarland standards at a wavelength of 530 nm and used for the inoculation of YST-21343 identification cards of the automated VITEK 2® compact system (bioMérieux, Marcy-l’Étoile, France) to identify the Candida isolates at the species level.
Antifungal susceptibility testing
After identifying the species, Candida isolates were assessed for susceptibility to five antifungal agents, including fluconazole (FCZ), voriconazole (VCZ), caspofungin (CAS), micafungin (MFG), and amphotericin B (AMB), using the AST-YS08 Vitek 2 cards, following the manufacturer’s instructions. The minimum inhibitory concentration (MIC) values of isolated Candida were determined after 24 and 48 h for all antifungal agents. MICs for these isolates were classified as susceptible (S), intermediate/susceptible dose-dependent (I/SDD), or resistant (R) according to species-specific clinical breakpoints established by the M27-A3 (for AMB) and Clinical and Laboratory Standards Institute (CLSI) M27M44S-ED3 (for azoles and echinocandins) documents. For AMB, Candida spp. isolates with MIC ⩽ 1 μg/mL and MIC ⩾ 2 μg/mL were classified as susceptible and resistant, respectively. 28 For FCZ, C. albicans, C. tropicalis, and C. parapsilosis isolates were considered susceptible (S), intermediate/susceptible dose-dependent (I/SDD), and resistant (R) at MIC ⩽ 2, MIC = 4, and MIC ⩾ 8 μg/mL, respectively. C. glabrata isolates were considered I/SDD and R at MIC ⩽ 32 and MIC ⩾ 64 μg/mL. C. krusei isolates were classified as R to fluconazole. For VCZ, C. albicans, C. tropicalis, and C. parapsilosis isolates were categorized as S, I/SDD, and R at MIC ⩽ 0.12, MIC = 0.25–0.5, and MIC ⩾ 1 μg/mL, respectively. C. krusei isolates were considered S, I/SDD, and R at MIC ⩽ 0.5, MIC = 1, and MIC ⩾ 2 μg/mL, while C. glabrata isolates were not classified. For CAS and MFG, isolates of C. albicans, C. tropicalis, and C. krusei with MIC ⩽ 0.25 μg/mL were considered S, those with MIC = 0.5 μg/mL were considered I/SDD, and those with MIC ⩾ 1 μg/mL were considered R. C. glabrata isolates were considered S, I/SDD, and R at 0.12, 0.25, and 0.5 μg/mL, respectively, while C. parapsilosis was classified as S, I/SDD, and R at MIC ⩽ 2, MIC = 4, and MIC ⩾ 8 μg/mL. 29 For quality control, C. krusei ATCC® 6258 was used as a reference strain for all experiments.
Statistical analysis
All data from the study were analyzed using IBM SPSS Statistics for Microsoft Windows, version 20.0 (IBM Corp., Armonk, NY, USA). All values in the tables were presented as case numbers (n) and percentages. Rates of susceptible, intermediate, and resistance were not analyzed for the isolates that lacked clinical breakpoints.
Results
A total of 102 isolates of yeast species were obtained from the urine and vaginal discharge of patients visiting the Medlatec healthcare system. Of these, 74 isolates (72.55%) were isolated from vaginal discharge and 28 (27.45%) from voided urine. All isolates were identified to the species based on yeast growth and metabolic changes through the automated VITEK 2 compact system. The results showed that five yeast species were identified. The most common yeast was C. albicans (80 isolates, 78.43%), followed by C. tropicalis (12 isolates, 11.76%), C. glabrata (5 isolates, 4.91%), C. parapsilosis (2 isolates, 1.96%), C. krusei (1 isolate, 0.98%). Two remaining isolates could not be accurately identified at the species level. The results also indicated that urinary tract candidiasis was more frequently caused by NAC species (57.14%) as compared to C. albicans (42.86%), whereas vulvovaginal candidiasis exhibited the opposite trend (8.11% and 91.89%) (Figures 1 and 2).

Distribution of Candida species isolated from patients with VVC and UTI.

Result of germ tube test.
The overall in vitro antifungal susceptibility pattern of Candida species to the five tested antifungal agents is summarized in Tables 1 and 2. The observed susceptibility rates of C. albicans isolates to FCZ, VCZ, CAS, MFG, and AMB were 96.10% (74 isolates), 83.75% (67 isolates), 96.25% (77 isolates), 98.75% (79 isolates), and 98.75% (79 isolates), respectively. Some drug-resistant isolates were found. This yeast showed 3.90%, 3.75%, and 2.50% resistance to the FCZ, VCZ, and CAS, respectively. The resistance rates of C. albicans to MFG and AMB were 1.25%. The highest overall resistance rate among Candida species was found against FCZ (7.7%), followed by VCZ (4.2%), CAS (4.0%), MFG (1.0%), and AMB (1.0%).
The in vitro antifungal susceptibility pattern of each kind of Candida spp. species.

I/SDD, Intermediate/susceptible dose-dependent; R, Resistant; S, susceptible.
Antifungal susceptibility patterns of Candida spp. isolated from patients with VVC and UTI.
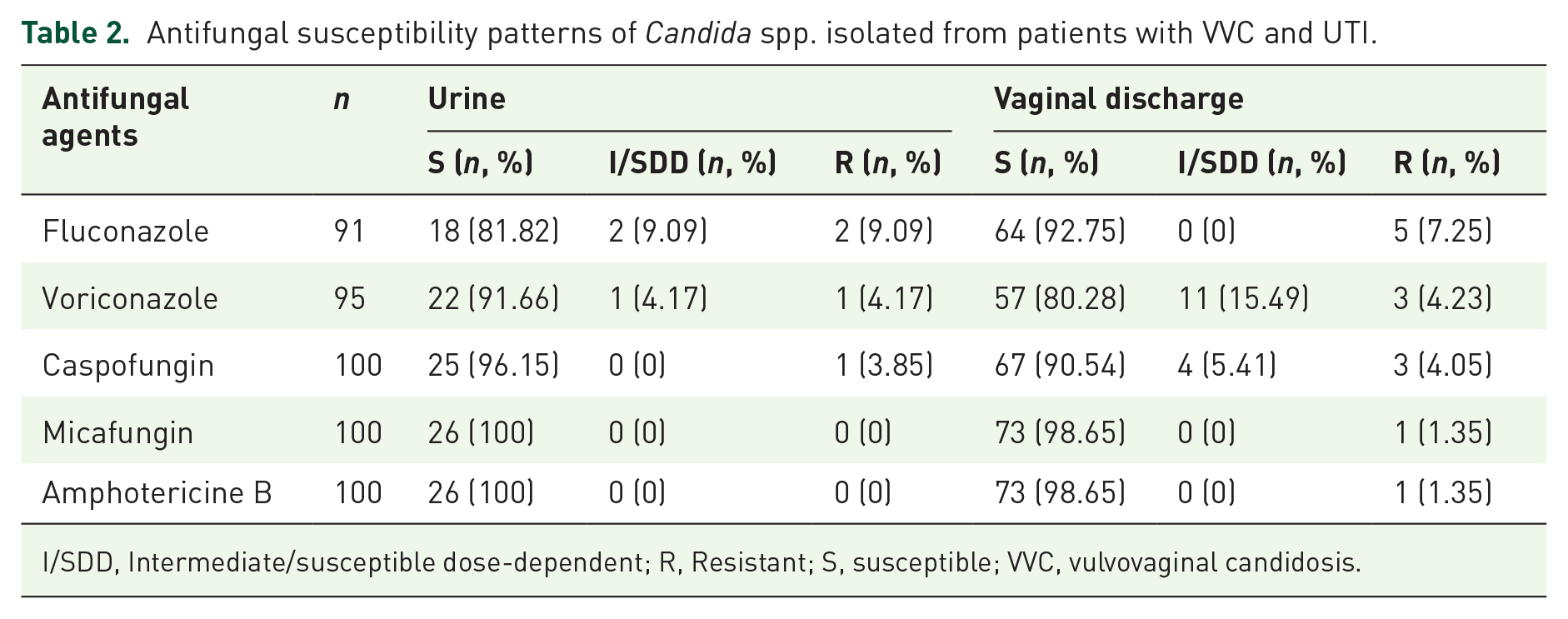
I/SDD, Intermediate/susceptible dose-dependent; R, Resistant; S, susceptible; VVC, vulvovaginal candidosis.
C. non-albicans isolates exhibited 100% susceptibility to MFG and AMB. Among the isolates, 3% (3 isolates), including two C. glabrata isolates and one C. tropicalis isolates, showed susceptibility dose-dependent to CAS, while two C. glabrata isolates were resistant. Regarding VCZ, 75.0% of the 12 C. tropicalis isolates were sensitive, 16.67% were intermediate/susceptibility dose-dependent, and 8.33% were resistant. Other Candida isolates (C. parapsilosis and C. krusei) showed 100% susceptibility to FCZ, VCZ, and CAS.
Discussion
Urogenital candidiasis is recognized as a common fungal infection worldwide, necessitating a comprehensive understanding.1,2,4,14 Recent studies suggest that the distribution of Candida species causing urogenital candidiasis varies among different geographic regions and study populations.1,23,30 In the current study, five yeast species were isolated, including C. albicans, C. tropicalis, C. glabrata, C. parapsilosis, and C. krusei, with two isolates classified as uncommon yeast species. Notably, C. albicans was the predominant species isolated from vaginal specimens, whereas the NAC species accounted for over 50% of urine samples, particularly C. tropicalis (39.29%). Many previous studies on Candida isolation from urine samples of urinary tract infection patients have reported findings similar to those of the present study, including Ozhak-Baysan et al., 3 Pramodhini et al., 12 De Oliviera et al., 31 and Kobayashi et al. 32 Previous studies have indicated an increasing trend of NAC species causing candiduria and VVC in various regions, with these species are often displaying higher resistance to antifungal agents.12,13,33 Therefore, the identification of Candida species and antifungal susceptibility testing are essential steps in selecting the appropriate treatment drugs.3,13,25
The results of this study indicated that the majority of Candida isolates were susceptible to FCZ, VCZ, CAS, MFG, and AMB, with susceptibility rates exceeding 83%. The highest resistance rates were observed for FCZ, affecting 7.7% of Candida isolates, primarily C. albicans, C. tropicalis, and C. krusei. In contrast, the resistance rates to VCZ, CAS, MFG, and AMB were lower, at 4.2%, 4.0%, 1.0%, and 1.0%, respectively. Notably, C. tropicalis exhibited decreased susceptibility to both FCZ and VCZ. These findings are consistent with those of Pramodhini et al., 12 Schmalreck et al. 34 and Osawa et al. 21 who also reported reduced susceptibility to FCZ and VCZ in C. tropicalis isolates.
Previously, limited information was available regarding the antifungal susceptibility of Candida causing VVC and UTI in Vietnam. In a previous study conducted by Anh et al. on 46 isolates of C. albicans from VVC patients in Vietnam, the resistance rates to FCZ, VCZ, and AMB were 4.35%, 4.35%, and 4.35%, 25 respectively, which were higher than those observed in the current study. In addition, the resistance of C. albicans to CAS and MFG was not reported by Anh et al., 25 but it was detected in our study. Our findings represent one of the initial studies on this issue in Vietnam. Therefore, further investigations are required to determine the distribution and antifungal susceptibility of Candida species causing VVC and candiduria in our country.
Fluconazole is commonly selected for the treatment of candiduria due to its safety profile. However, in cases where yeasts are resistant to fluconazole, voriconazole is often prescribed because it generally exhibits lower resistance rates compared to fluconazole and itraconazole.14,35–37 In the current study, some isolates resistant to voriconazole may have experienced cross-resistance, likely due to their similar chemical structure of these drugs and the limited use of voriconazole in Vietnam. Additionally, flucytosine and low-dose amphotericin B are viable options for treating azole-resistant Candida species.3,16 In the current investigation, low resistance rates to echinocandins and amphotericin B were observed across all Candida species. According to a study conducted by Sobel et al., 38 caspofungin was found at a lower concentration in blood plasma compared to urine. Nevertheless, the role of this drug, along with other echinocandins, in the treatment of Candida UTIs remains unclear.3,16
There are several limitations in this investigation. First, as a retrospective study, there is a lack of comprehensive clinical information to analyze associations with pathological outcomes. Second, the number of certain drugs does not match with the total count, as the Vitek® 2 system is unable to report the MIC for some strains during the analysis. Additionally, the number of NAC isolates is small, which may not be sufficient to draw definitive conclusions. Finally, our findings are from a single center and may not be applicable to other general hospitals. Therefore, further studies are needed to address these limitations in the future.
Conclusion
The most common yeast species found in this population was C. albicans. The frequency of NAC species isolated from patients with UTIs was notably high. Resistance rates among urogenital Candida isolates to antifungal agents were generally low, although some strains exhibited resistance to these drugs. Therefore, routine species identification and antifungal susceptibility testing of Candida isolates causing urogenital candidiasis should be conducted to guide appropriate screening and treatment protocols.
Footnotes
Acknowledgements
We are also indebted to the Department of Medical Microbiology (Medlatec Healthcare System) for providing the equipment used to identify species distribution and antifungal susceptibility patterns of the samples. The authors are also grateful to Assoc. Prof. Hoang Van Tong for revising the English text.
Declarations
Abbreviations
AMB Amphotericin B
ATCC American Type Culture Collection
CAS Caspofungin
CLSI Clinical and Laboratory Standards Institute
FCZ Fluconazole
ICU intensive care unit
MFG Micafungin
MIC Minimal Inhibitory Concentration
NAC non-albicans Candida
SDA Sabouraud Dextrose Agar
SDD Susceptible dose dependent
VVC Vulvovaginal candidiasis
VCZ Voriconazole