
Abstract
Opportunistic central nervous system (CNS) infections are a significant cause of morbidity and mortality in immunocompromized patients, including those undergoing transplantation and receiving immunomodulatory therapy. Particularly in these individuals, the clinical presentation of these infections may have atypical patterns, emphasizing the need to consider various diagnostic possibilities, including noninfectious conditions. Quick and accurate identification, along with prompt treatment, is crucial for improving patient outcomes. Therefore, understanding which pathogens are likely to cause infection based on factors such as timing post-transplantation, specific organ transplant, and the mechanism of action of immunomodulatory medications is essential. This review will provide a detailed description of the types of infections that may arise in the context of transplantation and immunomodulatory therapy.
Introduction
The prevalence of central nervous system (CNS) opportunistic infections in individuals undergoing hematopoietic stem cell transplant (HSCT), solid organ transplant (SOT), and those receiving treatment with immunomodulatory medications is rising significantly. As an increasing number of patients are being exposed to new immunosuppressive or immunomodulatory therapies for a range of autoimmune conditions or to prevent graft rejection in the context of transplantation, opportunistic neuroinfectious diseases are a rising cause of morbidity and mortality to consider among these patients. 1
Clinical presentation of CNS infections observed in these patients may differ from those in immunocompetent individuals. Particularly in this patient population, when suspecting an opportunistic infection, it is crucial to consider noninfectious differential diagnosis that could mimic similar clinical presentations occurring at a similar timing. These include side effects or toxicity from immunosuppressants (e.g., posterior reversible encephalopathy syndrome due to calcineurin inhibitors), posttransplant neurologic complications (e.g., stroke), or a flare of an underlying inflammatory condition (e.g., multiple sclerosis relapse).
Early diagnosis and treatment of opportunistic CNS infections are fundamental for improving prognosis in these patients. A rigorous understanding of the evaluation and management of neurological diseases in the context of transplantation and immunomodulatory medication use is crucial, as unusual clinical presentations, neuroimaging, and laboratory findings may be observed. 2 While laboratory abnormalities typically assist in diagnosing CNS infections in patients with an intact immune system, these may not be reliable in transplant recipients or immunocompromized individuals. Therefore, using multiple comprehensive tools such as neuroimaging in conjunction with a thorough physical examination, as well as newer diagnostic techniques such as metagenomic sequencing, becomes particularly important to achieve prompt diagnosis. 2
Neuroinfectious diseases in the posttransplant population
Transplant recipients undergo complex surgical procedures, which expose them to considerable physiological stress during and after the operation. Subsequently, they are exposed to immunosuppressive therapies aimed at preventing graft rejection, making them more vulnerable to a range of neurological complications that lead to poor outcomes, including death. CNS infections, accounting for up to 10% of transplant-associated complications, 3 may occur at any time post-HSCT or SOT, but more commonly follow specific patterns of timing after transplantation (Figure 1). Critical considerations for assessing CNS infections in these scenarios include timing after transplantation, type and dosage of immunosuppressive therapy, chronicity of presenting symptoms, and the neurological and systemic physical exam.

Timeline of pathogen occurrence following transplantation.
Hematopoietic stem-cell transplant
HSCT has traditionally been the primary treatment for hematopoietic malignancies and bone marrow failure, as well as hematologic disorders. 4 Typically, HSCT recipients first experience a noticeable decline in their immune system, followed by a gradual recovery. This begins with the conditioning regimen administered before the transplant. As the immune system begins to recover, transplant patients may experience specific opportunistic infections at different timepoints post-transplantation. 5
Neurological complications after transplantation occur in at least 20% of HSCT recipients, 6 with a variable incidence of neuroinvasive infections depending on the conditioning regimen, the donor type (allogenic or autologous), and the source of stem cells (peripheral blood, bone marrow, or umbilical cord blood). CNS infections after HSCT often manifest in distinct time frames including within the first month posttransplant, between the second and sixth months, and several years later in the post-transplantation period. 7
During the first month posttransplant, CNS infections that often occur include the reactivation of Cytomegalovirus (CMV), Toxoplasma gondii, and other herpesviruses. 7 Human HerpesVirus-6 (HHV-6) reactivation may occur 2–6 weeks post-transplantation and typically manifests with acute limbic encephalitis. Clinical presentation of limbic encephalitis can include fever, seizures, personality changes, visual hallucinations, anterograde amnesia, or altered mental status. This infection can reactivate from an extrachromosomal circular DNA latency or a chromosomally integrated latency (ciHHV-6), which influences the results of polymerase chain reaction (PCR) diagnostic tests. Droplet digital PCR (ddPCR) and reverse transcriptase PCR (RT-PCR) are valuable tools for distinguishing between ciHHV-6 and active infection, as individuals with ciHHV-6 can exhibit high viral loads even without reactivation.8,9 Moreover, quantitative PCR analysis from various compartments, such as blood, serum, cerebrospinal fluid (CSF), or native tissue, may be necessary to differentiate between latent infection, ciHHV-6 presence, and reactivation. All HSCT recipients with altered mental status and/or seizures should undergo evaluation for HHV-6, even if radiological characteristics of limbic involvement are absent. This is crucial because, in one-third of cases, brain MRI may not reveal typical limbic encephalitis patterns, even in the presence of significant neurological deterioration. 10 For treatment, full-dose therapy with ganciclovir or foscarnet is recommended to manage HHV-6 encephalitis post-HSCT. 11
CMV CNS disease after HSCT can be attributed to patients receiving T-cell-depleted stem-cell grafts or those treated with the T-cell depleting agent anti-thymocyte globulin, as cytotoxic T-cells are crucial for protection against CMV disease. 12 The risk is further increased in recipients with a CMV-seropositive status before transplant or those receiving HSCT from CMV-seropositive donors. 13 In CMV CNS infection, the predominant clinical presentation is meningoencephalitis, diagnosed by identifying CMV DNA in CSF samples or brain tissue. 14 Notably, metagenomic next-generation sequencing could be a useful tool to diagnose or screen patients with suspected CMV encephalitis. 15 The mortality and morbidity of CNS CMV invasion are particularly higher compared to CMV invasion of other organs, mostly due to the low penetration of antiviral drugs into the CNS and antiviral resistance. 12 However, adoptive third-party T-cell transfer is a newer, promising therapy. This treatment involves obtaining CMV-specific T-cells from a healthy donor who has been previously exposed to CMV and has developed immunity against it. The donor’s T-cells are collected, cultured, stimulated to increase in number, and then infused into the patient. The beneficial effects of this therapy are mainly due to its safety and high response rate in reducing viral load and controlling the infection.16,17
CNS infections occurring between the second and sixth months are primarily a result of cellular immunity impairment during this period. Microorganisms such as Aspergillus, CMV, John Cunningham virus (JCV), Epstein Barr virus (EBV), and Varicella-Zoster Virus (VZV) become primary concerns. 18 Specific risk factors such as neutropenia lasting more than 10 days with an absolute neutrophil count less than 500/mm3 represent the most significant risk for developing invasive aspergillosis, 7 which due to its angioinvasive properties, can lead to cerebral aneurysms, vasculitis, or subarachnoid hemorrhage. Neurological involvement of VZV typically arises after the first month of transplantation, with calcineurin inhibitors and chronic glucocorticoid use being the most significant risk factors. For further information regarding clinical presentation, diagnosis, and treatment of Aspergillus and VZV, go to the pathogen section.
In the later stages following HSCT, the majority of CNS infections occur in the context of graft versus host disease (GVHD), which significantly increases morbidity and mortality in patients who have undergone this type of transplant. 1 GVHD is a risk factor for infection among HSCT recipients due to its association with delayed immunologic recovery and prolonged immunodeficiency, along with the immunosuppressants used to treat GVHD that further increase the vulnerability to opportunistic infections. During this phase, allogeneic HSCT recipients with GVHD have an increased risk of infections due to CMV, VZV, EBV-related Posttransplant lymphoproliferative disorder (PTLD), JCV, community-acquired respiratory viruses, and infections with encapsulated bacteria. 5
JCV reactivation typically occurs approximately 1 year or later, leading to Progressive Multifocal Leukoencephalopathy (PML). PTLD emerges years after HSCT, with a median time of occurrence ranging between 4 and 5 years. However, PTLD onset time may vary based on individual patient conditions.19,20 Factors that contribute to an elevated risk of developing PTLD in HSCT include seroconversion from negative EBV before transplant to positive after the transplant 21 ; pretransplant conditioning regimen with anti-thymocyte globulin in a dose-dependent manner 22 and conditioning with Alemtuzumab, primarily due to T-cell depletion. 23
Solid organ transplant
SOT-related neurological infections often manifest in a temporal pattern similar to HSCT, although certain CNS infections are more common among specific SOT recipients (Figure 1).
Donor-derived CNS infections in SOT recipients are a significant concern in the early transplantation period. 24 These infections may initially present with nonspecific signs such as altered mental status and fever, but specific syndromes such as meningitis or encephalitis that develop shortly after transplantation should raise suspicion of donor-transmitted CNS disease; however, the presentation can vary and may take months to manifest. This suspicion should also arise if multiple organ recipients from a single donor develop similar infectious complications. 25 If suspected, it should be promptly reported to the Organ Procurement and Transplantation Network, leading to immediate investigation and evaluation of other potentially affected recipients to prevent further transmission. 26 It is recommended to avoid transplantation of organs from donors with meningoencephalitis of unknown etiology, as there is a documented risk of transmitting rabies, West Nile Virus (WNV), Lymphocytic Choriomeningitis Virus (LCMV), Cryptococcus gatti, Balamuthia mandrillaris through organ transplant. 27 However, organs from donors with confirmed bacterial meningitis caused by Escherichia coli, Haemophilus influenzae, Streptococcus pneumoniae, or Neisseria meningitidis can be safely used for organ donation if the donor receives appropriate treatment before donation and the recipient undergoes prophylactic treatment for 7–10 days posttransplant with close monitoring. 28
In the initial month following SOT, neurological infections may arise due to pathogens such as LCMV, HHV-6, Aspergillus, and Cryptococcus. 3 LCMV and HHV-6 typically manifest within the first few weeks post-transplantation, with no specific organ association. Transplant recipients may acquire LCMV infection through donor-derived transmission or exposure to wild or infected pet rodents, such as hamsters, mice, or guinea pigs. 29 The majority of reported cases with donor-derived infection present severe disease characterized by coagulopathy, neuroinvasive disease, and dysfunction of the transplanted organ. Diagnosing LCMV infection can be challenging, primarily due to the lack of awareness of the virus among physicians and the limited availability of diagnosticassays to detect LCMV-specific antibodies, which are only offered by a few commercial laboratories. These assays currently lack clear descriptions of sensitivity and specificity. Thus, to enhance the reliability of the diagnostic evaluation, the following tests should be conducted: specific IgM and IgG antibodies testing in cerebrospinal fluid (CSF) and serum; PCR in serum, blood, and CSF; and tissue biopsy with immunohistochemical staining. 29 Unbiased metagenomic deep sequencing has successfully identified LCMV infection in cases where initial testing yielded negative results. According to the guidelines from the American Society of Transplantation Infectious Diseases Community of Practice, the recommended treatment, which enhances survival rates (60% for those treated with ribavirin vs 19% for those without ribavirin), includes lowering immunosuppression, giving intravenous (IV) and oral ribavirin, and administering intravenous immunoglobulin (IVIG). Transplant patients are advised to avoid contact with house mice or wild and pet rodents, especially refraining from cleaning their cages and providing direct handling and care. 29
Among early fungal infections following SOT, Aspergillus, Candida spp, and Cryptococcus neoformans are the primary microorganisms associated with CNS involvement. 3 Notably, lung transplant, although a vital treatment for chronic lung diseases, poses the highest risk for invasive fungal infections among SOT patients, mainly due to the graft’s direct exposure to fungi in the environment. 30 The most common causes of invasive fungal CNS infections post-lung transplant are Aspergillus and Candida spp, and less commonly, Cryptococcus neoformans, Mucorales, Pneumocystis jirovecii, and endemic fungal infections. Aspergillosis, the most frequent cause of brain abscesses in this context, typically manifests at a median time of 24 days post-transplantation. The overall incidence of invasive aspergillosis post-SOT is 8.3%–23.3% in the lung, 3.5%–26.7% in the heart, 1%–4.7% in the liver, and 1.2%–4% in kidney transplant recipients. 31 Invasive aspergillosis in SOT patients increases the overall mortality, with a 3-month rate as high as 15%–25% in non-liver SOT and up to 80%–90% in liver SOT recipients. 32 This high mortality in liver SOT is mainly due to the particular risk of developing disseminated aspergillosis with CNS involvement. For further information regarding clinical presentation, diagnosis, and treatment of aspergillosis, go to the pathogen section.
Cryptococcal extrapulmonary or disseminated disease leads to meningoencephalitis or meningitis, with symptoms developing on average within 2–90 days after transplantation and, more commonly, among lung or liver organ recipients. 33 Cryptococcosis accounts for 8% of invasive fungal infections in SOT recipients, with an overall incidence of 0.2%–5% and a CNS involvement in 50%–75% of these patients. 34 In SOT recipients, the mortality rate is notably higher in those with CNS cryptococcosis, approximately 30%, compared to 7% in those with infection confined to the lungs. 35 In a multicenter cohort study of SOT recipients with Cryptococcosis, an independent association was found between an increased risk of CNS cryptococcosis and serum cryptococcal antigen titers >1:64, fungemia, and infections occurring 2 years post-transplantation. 36 The absence of cryptococcal antibodies at the time of transplantation and the acquisition of infection for the first time posttransplant also increase the risk and severity of CNS cryptococcosis. It is increasingly recognized that CSF analysis should be promptly conducted in all patients diagnosed with Cryptococcosis, particularly those with cryptococcal antigen titers >1:64, fungemia, altered mental status, and development of Cryptococcosis after 2 years of transplantation. 36 Treatment should include fungicidal therapy with liposomal amphotericin B (L-AmB) and 5-flucytosine, followed by a consolidation and maintenance phase with fluconazole. Additionally, slowly reducing immunosuppression while undergoing antifungal therapy will help eradicate infection and preserve allograft function. If the initial CSF pressure is greater than 25 cm or the development of increased intracranial pressure symptoms occurs during induction therapy, serial lumbar punctures should be performed until CSF pressure is reduced by 50%. 34
Between 2 and 6 months post-transplantation, while relatively uncommon, there is a potential risk of Toxoplasma gondii infection, particularly in heart transplant recipients.3,37 Cardiac transplant recipients who are seronegative at transplantation and receive a transplant from a seropositive donor (D+/R−) face the highest risk of infection. 38 Moreover, those cases that develop within the first month after transplant have a significantly higher risk of mortality (100%) compared to those that develop infection after 180 days of transplant (25%). 39 CNS toxoplasmosis typically presents with encephalitis or intracranial mass lesions, although rare cases of meningitis have been reported.1,40 Symptoms may include seizures, headache, altered mental status, fever, cranial nerve palsy, focal neurological deficits, or even abnormal movements if basal ganglia are compromised. Diagnosing CNS toxoplasmosis involves laboratory, imaging, and histological testing. For definite diagnosis, tachyzoites should be identified in brain biopsy or T. gondii DNA in the CSF by nucleic acid amplification assays. 41 CSF PCR to detect T. gondii DNA is specific, but not sensitive, for diagnosing toxoplasmic encephalitis, and lumbar puncture can often be unsafe for those patients with brain mass lesions due to the risk of brain herniation. The gold standard is a brain biopsy, although confirmation of the diagnosis is often achieved through the adequate improvement of clinical symptoms and neuroimaging after treatment. 42 Treatment recommended for acute toxoplasmosis in transplant recipients consists of induction therapy followed by chronic suppressive therapy. Pyrimethamine, sulfadiazine, and leucovorin for at least 6 weeks should be followed by the same medications but at lower doses. 38
In the posttransplant period, it is crucial to recognize that several other CNS infections can present with mass-like lesions, similar to Aspergillus, Cryptococcus, or Toxoplasma gondii. While these are more common pathogens, it is essential to consider other, less common pathogens, such as Nocardia, Rhodococcus, Listeria monocytogenes, and Trypanosoma cruzi (Chagas disease). Nocardia and Rhodococcus primarily cause cerebral abscesses.43–45 However, Nocardia is more frequently associated with lung transplantation, 46 and Rhodococcus is more commonly seen in renal transplantation, followed by heart and liver transplants. 47 Conversely, Listeria and Trypanosoma cruzi primarily present with meningoencephalitis, though cerebral abscesses can also occur in both cases.48,49 The brain abscesses caused by Trypanosoma cruzi, known as cerebral chagomas, are often associated with distinctive Chagas-like symptoms such as fever, anemia, jaundice, and liver function abnormalities. 50 For further information regarding clinical presentation, diagnosis, and treatment of cerebral abscesses in the immunocompromized population, refer to the pathogen section.
In the most recent reviews regarding WNV infection associated with SOT recipients, the average reported time-to-infection was between 14 and 50 months after transplantation.51,52 While WNV typically results in neuroinvasive disease in <1% of immunocompetent individuals, older individuals and those that are immunocompromized, such as SOT recipients and individuals undergoing chemotherapy, exhibit an elevated susceptibility. The reported risk of neuroinvasive disease in transplant recipients with confirmed WNV infection is 40%, 51 with kidney transplant recipients exhibiting the highest prevalence, followed by pancreas, liver, heart, and lung transplant recipients. 52 The mean incubation period is between 7 and 17 days, with a shorter time-to-infection after transplant if the infection was blood or donor-derived and longer if the infection was community-acquired (mosquito bite).
WNV neuroinvasive disease can appear as meningitis, meningoencephalitis, or poliomyelitis-like flaccid paralysis, with up to half of these cases experiencing residual symptoms 1 year after infection. These symptoms may include fatigue, headache, cognitive impairment, or movement disorders. WNV testing typically involves examining serum and CSF for IgM and IgG antibodies and viral nucleic acid testing (NAT). A diagnosis of acute WNV infection may be confirmed if: (1) serum or CSF WNV NAT is positive, irrespective of IgM/IgG status; or (2) serum or CSF IgM tests positive, irrespective of NAT or IgG results. 29 The sensitivity of serum WNV IgM is between 91% and 98%, 51 although in patients with impaired humoral immunity, such as transplant recipients, WNV antibody production may be compromised, leading to persistent viremia. Therefore, in addition to conducting WNV IgM antibody tests on CSF and serum, it is recommended to perform WNV PCR or NAAT testing on serum or whole blood to enhance sensitivity. 29 Treatment of WNV encephalitis involves supportive care and temporary reduction of immunosuppression. There are no clinical trials supporting specific antiviral agents. However, other possible therapies that need further investigation and have been studied in animal models are IVIG containing specific antibodies and Interferon alpha-2b. 29 According to the Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice, ribavirin is not currently recommended for treating WNV infection among SOT recipients, as in the previous case series, it is associated with an increased risk of death.53–55
Patients who have undergone SOT face an increased risk of developing PTLD within two peaks of time: 2 and 5 years post-transplantation.56,57 The likelihood of developing PTLD varies among different organ transplants, with intestine transplantation representing the most significant risk (20%), followed by lung (3%–10%), heart (2%–8%), liver (1%–5%), and kidney (0.8%–2.5%) transplants. 58 The increased risk of PTLD following intestine and lung transplants is primarily attributed to the abundance of lymphocytic tissue containing notable B-cell reservoirs in these organs.
Immunosuppressive and immunomodulatory treatments
Immunosuppressive medications are medications that broadly suppress the immune system and are used to treat malignancies as well as autoimmune conditions. Immunomodulatory therapies have selective effects on the immune system and are increasingly used to treat various autoimmune conditions. Both of these types of therapies are used to treat patients with hematologic malignancies, SOT, and HSCT as well as with various autoimmune disorders, including rheumatologic disorders, autoimmune neurologic disorders, inflammatory bowel diseases, and other systemic inflammatory disorders. 59 Individually each of these conditions isgenerally considered rare, 60 though as a group autoimmune conditions show an increasing prevalence globally, particularly in Europe and North America. 61 The overall prevalence of autoimmune diseases has been estimated at around 10% increasing in the United Kingdom 62 and previously at 3% in the United States. 63 In the United States, there are estimated to be approximately 750,000 individuals with multiple sclerosis, 64 while systemic lupus erythematosus is estimated to affect around 200,000. 65
The type of infections associated with these treatments varies based on the mechanism of action of the drug and also based on the underlying disease being treated. Immunosuppressive therapies with a broad range of actions can predispose individuals to a wide range of infectious agents. For example, corticosteroid poses an increased risk for infections with pyogenic bacteria, atypical bacteria such as Mycobacterium Tuberculosis, viruses such as VZV, fungi such as cryptococcus, as well as various helminthic infections. Immunomodulatory therapies, on the other hand, can increase the risk for certain specific organisms. For example, the use of eculizumab, a complement inhibitor, is associated with an increased risk of development of meningitis due to Neisseria meningitidis. 66 Table 1 lists the various immunomodulatory and immunosuppressive agents, their uses, mechanisms and immunologic effects, and some important associated pathogens. Some listed uses may be off-label. The indications and uses listed are not a comprehensive accounting of all uses that may be encountered in clinical practice.
Immunosuppressive medications and associated pathogens causing neurologic diseases

Table created by the authors.
Not all listed uses are approved indications, and many listed uses may be off-label. Noted indications/uses should not be considered a comprehensive listing of uses that may be encountered in clinical practice.
CMV, Cytomegalovirus; HSV, Herpes Simplex Virus; ITP, Immune Thrombocytopenic Purpura; JCV, JC virus; NMO-SD, Neuromyelitis Optica Spectrum Disorder; SLE, Systemic Lupus erythematosus; TNF-R, Tumor Necrosis Factor Receptor; VZV, Varicella-Zoster virus; WNV, West Nile virus.
Specific pathogens
Neurologic infections are a major cause of morbidity in immunocompromized patients, including recipients of HSCT, SOT, and individuals treated with immunomodulators. While each of these patient groups requires a tailored and individualized approach to evaluation and management, there is the similarity between transplant recipients and those treated with immunomodulators for other conditions. Both populations face shared challenges related to diagnosis and treatment concerning five key conditions: JCV, VZV, fungal infections, atypical neuroinvasive mycobacterial infections, and PTLD.
Progressive multifocal leukoencephalopathy
PML is predominantly diagnosed in patients who have undergone HSCT, patients with HIV infection, receiving biological drugs, and less likely in SOT recipients. JCV infection is commonly acquired in childhood or adolescence, initially affecting lymphatic tissue and eventually remaining dormant in the urinary tract, bone marrow, and CNS. PML results from the reactivation of this latent JCV infection, facilitated by a weakened cellular response and JCV gene recombination, leading to oligodendrocyte destruction and myelin degradation. 67
In the past decades, around 80% of PML cases were related to HIV infection. 68 However, with the use of combined antiretroviral therapy (cART), this trend has shifted toward lower numbers. An increasing number of PML cases are now attributable to a broader range of conditions, such as immunosuppressive medications, malignancies like non-Hodgkin lymphoma or chronic leukemia, transplantation, or rheumatologic diseases.69,70 Among patients with multiple sclerosis, PML is predominantly associated with natalizumab use. Still, it is also important to consider the risk posed by other immunomodulatory drugs, including monoclonal antibodies such as fingolimod.
The clinical presentation and neurological deficits depend on the area of white matter demyelination. Still, common symptoms vary among speech abnormalities, cognitive/behavioral impairment, motor weakness, unsteady gait, limb ataxia, and visual disorders. 69 PML definitive diagnosis is done when clinical presentation and imaging findings are consistent and not better explained by other conditions, along with CSF JCV DNA isolation with PCR. Alternatively, a brain biopsy can confirm the diagnosis, if it shows the specific set of histopathological changes characteristic of PML. 71 In particular, MR imaging patterns may be crucial in differentiating PML, PML-Immune reconstitution inflammatory syndrome (PML-IRIS), and Multiple sclerosis relapse.67,72
Classic PML lesions typically exhibit a subcortical or juxtacortical distribution, often presenting an asymmetric and confluent pattern in the parieto-occipital lobes (see Figure 2). Initially, on T1-weighted imaging, these lesions appear isointense but may become hypointense over time due to a lack of remyelination. On T2-weighted imaging, the affected areas commonly display hyperintense lesions, with smaller punctate lesions surrounding the main area, reflecting the inflammation of perivascular spaces (“Milky Way appearance”). 73 Lesions of classic PML do not have significant mass effects, edema, or enhancement after contrast administration.

Imaging findings of PML on MRI. Axial brain images of a patient presenting with PML lesions, with asymmetric and bilateral hyperintensities on T2 weighted images (T2/FLAIR) in the white matter.
Although PML primarily affects the white matter, JCV may also invade cortical and deep gray neurons, leading to leukocortical or intracortical lesions resembling those seen in multiple sclerosis. PML-associated gray matter lesions are most commonly identified in the thalamus, occurring in 5%–31% of the cases. 74 Less commonly, T2/FLAIR sequences may reveal distinctive patterns such as the “shrimp sign,” characterized by a crescent-shaped lesion that extends from the middle cerebellar peduncles into the adjacent cerebellar white matter while sparing the dentate nuclei. Notably, the radiological shrimp sign, aligned with the corresponding clinical presentation, represents an excellent sensitivity and specificity for cerebellar PML. 75 The “barbell sign” has also been reported, indicating signal abnormalities in the parieto-occipital region extending across the splenium. Gadolinium enhancement is unusual, but most reported cases tend to be associated with PML-IRIS, accounting for 31% of PML-IRIS cases compared to 2.6% of PML without IRIS. 76
In the case of PML-IRIS, which is an inflammatory response triggered by immune system recovery, there is a paradoxical worsening of neurological symptoms and signs. For transplant recipients or patients undergoing immunosuppressive therapy with known PML, suspicion of PML-IRIS arises when symptoms worsen after reducing or changing immunosuppressants. 77 In these cases, the inflammatory response can result in atypical clinical and radiological presentations of PML. MRI findings might show inflammatory changes, considered rare in classic PML, contrast enhancement within the lesion, edema, and mass effect. 69
Managing PML presents a difficult challenge since the most described effective treatment involves reducing immunosuppression to facilitate immune reconstitution. However, this approach carries a high risk of graft failure or exacerbation of certain diseases, such as multiple sclerosis, which accounts for the complexity of treating this infection in these clinical scenarios. Attempts have been made to target the virus directly with antiviral medications such as cytarabine and cidofovir, as well as with the antimalarial agent mefloquine. However, these strategies have not demonstrated improved survival or reduced neurological disability in clinical trials; instead, many studies have been terminated prematurely due to severe medication toxicity and lack of efficacy.69,78
There have been reported cases of successful novel therapies, such as the IV infusion of JCV-targeted specific cytotoxic T-cells, which has proven to be a safe and feasible treatment strategy, especially in vulnerable populations not amenable to immunosuppressant drug modulation.79–81 This treatment consists of collecting lymphocytes from an Human Leukocyte Antigen (HLA) haploidentical family donor, followed by their stimulation with JCV-specific peptides, such as viral capsid one protein (VP1) and large T proteins (LT). This stimulation lasts approximately 12 days, after which the recovered cells are replated and re-pulsed with JCV peptide mixes in the presence of interleukin-2 for an additional 12–14 days. The obtained cells undergo vigorous quality control testing, including assessment of sterility, alloreactivity, and potency using ELISPOT assays and standard Cr release assays. 82 The specific T-cells successfully generated are then intravenously infused into patients.
Immune checkpoint inhibitors (ICIs), which have been primarily used in cancer treatment, have been explored to treat PML. In some cases, medications like nivolumab and pembrolizumab, have shown a beneficial immune response leading to clearance of JCV from the CSF along with improvement of symptoms.83–85 However, it is controversial, as its efficacy varies and has limited benefits, particularly in patients with severe immunosuppression. 86 Despite successfully treating isolated cases, larger studies are needed to identify which patients are more likely to benefit from ICIs, considering their potential adverse effects and limited efficacy compared to other therapeutic options.
Varicella-Zoster virus
Primary infection with VZV is responsible for chickenpox, commonly seen in children. Subsequently, the virus remains latent in various ganglia in the nervous system. Reactivation of VZV results in zoster and can cause various neurologic complications, including vasculopathy, meningoencephalitis, myelitis, and cranial neuropathies. Immunocompromized states such as transplant recipients, patients with hematologic malignancies, and those on immunosuppressive medications, including corticosteroids, are known risk factors for developing complications of VZV. 87
Zoster (Shingles)
VZV reactivation is characterized by the development of rash and pain in a dermatomal distribution. Zoster can develop anywhere in the body as the virus can be latent in the dorsal root, cranial nerve, or autonomic ganglia. 88 In immunocompromized states, recurrent zoster, as well as multidermatomal involvement with zoster, is well-known. 89
Cranial neuropathies secondary to VZV
Any cranial nerve can be involved with VZV. The most well-known is the facial nerve’s involvement, known as Ramsay Hunt syndrome. This is characterized by lower motor neuron facial weakness in association with vesicles in the ipsilateral external auditory canal. However, other cranial neuropathies, including optic neuropathy, oculomotor neuropathy, trigeminal neuropathy, vestibular neuropathy, and hypoglossal neuropathy, are described. 88 Immunocompromized patients often develop multiple cranial neuritis. 90
Zoster paresis
Following a zoster rash, individuals can develop motor weakness involving the limb, abdominal wall, or diaphragm. This represents the spread of VZV from the dorsal root ganglia to the motor neuron. 91
VZV meningitis
VZV can manifest as meningitis, meningoencephalitis, meningoradiculitis, or cerebellitis, even without the presence of a rash. An MRI may reveal meningeal enhancement. The diagnosis is established by identifying VZV DNA or VZV IgG antibodies in the CSF. 88
VZV vasculopathy
VZV vasculopathy occurs when the virus invades the vessel wall, potentially affecting both small and large cerebral arteries. This primarily presents as ischemic or hemorrhagic infarcts in the brain or spinal cord. It can rarely cause arterial dissection, aneurysm formation, secondary subarachnoid hemorrhage, and peripheral arterial disease. 92 Enhancing lesions in the gray-white matter junction and involvement of multiple vascular territories offer clues to the diagnosis of VZV on MRI. CSF analysis demonstrates mononuclear pleocytosis in most patients. About a third of patients do not have preceding zoster or CSF pleocytosis, which can make this diagnosis challenging. 93 Diagnosis is established by the detection of VZV DNA by PCR in CSF or by demonstrating VZV IgG antibodies in the CSF, with an increased CSF to serum ratio. While VZV DNA PCR is specific, it is detected in only 30% of cases of VZV vasculopathy. 94
VZV myelitis
In immunosuppressed patients, VZV can invade the spinal cord and present as an insidious, progressive myelopathy. MRI demonstrates longitudinal enhancing lesions. 95 VZV myelitis can present without a rash. CSF analysis is characterized by mononuclear pleocytosis, normal or slightly elevated protein, and the presence of VZV IgG or VZV DNA. 91
These syndromes can present without a zoster rash in about 35% of cases, which can make the diagnosis challenging. 93 While MR imaging is useful for pattern recognition, diagnostic testing for CNS complications of VZV is usually accomplished by either PCR testing or by detection of intrathecally produced IgG or IgM antibodies against VZV in CSF. VZV antibodies in the CSF have been shown to have more sensitivity than CSF PCR testing, especially for VZV vasculopathy. 92 Thus, it is recommended to test for both VZV PCR and VZV antibodies in the CSF. 88 Serum antibodies are generally not helpful in the diagnosis of VZV reactivation. Zoster is treated with the use of oral antiviral agents like famciclovir (500 mg three times a day), valacyclovir (1 g three times a day), or acyclovir (800 mg five times a day) given for 7–10 days. In immunosuppressed patients, if the rash does not begin to fade within 1 week of treatment, IV Acyclovir is recommended. 88 Treatment for CNS complications includes IV Acyclovir 10–15 mg/kg three times daily. Additionally, a short course of oral prednisone is recommended for patients with VZV Vasculopathy based on a small study where 12 patients were treated with steroids. 93 With the above treatment, mortality with VZV in immunosuppressed patients remains low at 3% and 71% of patients can have complete neurologic recovery. 90
Intracranial abscesses
Fungal infections in the brain are a common cause of brain abscesses in patients who are immunocompromized. Intracranial abscesses with typical bacterial organisms are rare in this population. In one study of liver transplant recipients, 18% of all CNS lesions were due to brain abscesses and all brain abscesses were fungal abscesses. 96 In another study of SOT recipients, all brain abscesses were caused by a fungus, Nocardia, or Toxoplasma. 97 Common fungal pathogens include Aspergillus, Mucor, Candida, and Cryptococcus. 87 Infections with M. Tuberculosis and Nocardia can also occur in these patients. Infections with endemic mycoses such as Blastomycosis, Coccidioidomycosis, and Histoplasmosis should be considered in these patients based on the geographic location. Invasive scedosporiosis is of increasing concern in immunocompromized patients due to high mortality rates with CNS involvement and secondary to resistance to antifungal treatment. 98
Aspergillus
Aspergillus Fumigatus is an angioinvasive fungus that causes CNS disease almost exclusively in immunocompromized patients. Vasculitis, infarctions, hemorrhage, and multiple intracranial abscesses can result due to invasion of elastin of the vessel wall. Aspergillosis may present as chronic meningitis as well. 7 Imaging findings often demonstrate the involvement of the basal ganglia and thalami. Diagnosis can be challenging as fungal cultures and Aspergillus antigen detection in CSF have poor sensitivity. CSF Galactomannan Antigen test has a sensitivity of 88.2% and specificity of 96.3% in diagnosing cerebral aspergillosis. 99 CSF Aspergillus PCR testing can be useful with a sensitivity and specificity of 75% and 98.3%, respectively. 100 Treatment involves using voriconazole, reducing immunosuppressants, and possible neurosurgical interventions. Previously, CNS Aspergillosis had a poor prognosis with a case fatality rate of around 90%. 101 With the recent availability of isavuconazole, survival for CNS Aspergillosis has improved with one study demonstrating 62.5% survival at day 84. 102
Mucormycosis
Cerebral mucormycosis often results from the contiguous spread of sinonasal disease. It can rarely result from the hematologic spread of fungemia. Like Aspergillus, mucor is also an angioinvasive fungus and frequently affects basal ganglia, causing abscesses, infarcts, and hemorrhage. Diagnosis is often established by biopsy of the affected tissue. Surgical excision and early use of L-AmB are needed to reduce mortality and morbidity in these patients. 87
Candida
CNS candidiasis is quite rare but a severe infection. It is mainly seen as a complication of disseminated systemic candidiasis but can occur as localized CNS infection secondary to neurosurgical procedures. It can present as chronic meningitis, multiple small abscesses, or infarcts. Diagnosis is usually established by identifying systemic candida infection. CSF may show elevated levels of 1,3-β-
Posttransplant lymphoproliferative disorder
PTLD is a rare and serious complication, with an estimated occurrence of 2% in individuals undergoing allogeneic HSCT and between 10% and 15% in SOT recipients. 19 It can manifest in two distinct forms: EBV-positive and EBV-negative, with early and late presentations in the posttransplant period, respectively. Moreover, high-intensity immunosuppression during the peri-transplant induction phase is associated with early PTLD manifestation, while chronic immunosuppression is more commonly linked to late-onset PTLD. 104
Approximately 90% of adults and 50% of children carry latent EBV in their B-cells, primarily controlled by T lymphocytes and NK cells. 105 Following the acute phase of EBV infection, the immune system generates memory B-cells, and EBV enters a latent phase, remaining dormant for life. However, in cases of profound immunosuppression, such as during the posttransplant period, EBV can reactivate and lead to PTLD development.
PTLD localized in the CNS represents only 5%–30% of all PTLD cases, 20 and individuals with this form tend to have poorer outcomes compared to patients with PTLD outside of the CNS. While some cases have been reported to appear as early as 6 weeks posttransplantation, they most commonly manifest years after transplantation and the initiation of immunosuppression. 20 Neurological symptoms can be nonspecific and vary according to the location of the CNS lesions. Among these, headaches, altered mental status, and seizures are the most common ones. Seizures, in particular, might be accompanied by focal symptoms such as motor, sensory, and visual impairments, which may suggest the location of the lesions.
Diagnosis of CNS-PTLD can involve CSF analysis, neuroimaging, and, biopsy for a definitive diagnosis. CSF analysis, with PCR for EBV and flow cytometry alone, may possibly make the diagnosis, but studies such as MRI or CT scans are often needed to identify characteristic patterns of CNS-PTLD. The detection of EBV PCR in CSF should be interpreted cautiously, as it may be nonspecific. 106 It has been determined that its presence could be incidental rather than causative, as patients with positive EBV PCR results could also have other identifiable pathogens. It may result from increased blood-brain barrier permeability or B-cells carrying EBV entering the CSF during neuroinflammatory processes, rather than a direct infection of the CNS by EBV.106,107 Therefore, it is important to integrate further studies, such as imaging, and if possible, biopsy, to achieve a more accurate diagnosis.
In imaging, multifocal lesions are more common than unifocal ones, primarily appearing in the lobar regions, followed by basal ganglia.20,108 Less typically, lesions can manifest in the periventricular areas, brainstem, cerebellum, or corpus callosum. 109 MRI lesions are typically reported as highly cellular tumors, which, due to their high risk of hemorrhage, often present with cystic and necrotic changes with surrounding edema. T1-weighted imaging predominantly demonstrates iso- or hypointense lesions, with a few reported cases having hyperintense or heterogeneous T1 signals. Given the mixture of solid areas with cystic and necrotic changes, the T2-weighted (T2W) imaging varies in appearance and might present with hypo-, iso-, or hyperintense lesions. T2W images reflect the surrounding edema, which ranges from mild to extensive depending on the size of the lesions.3,20 See Figure 3 as an example of MRI lesions in a patient with CNS-PTLD.
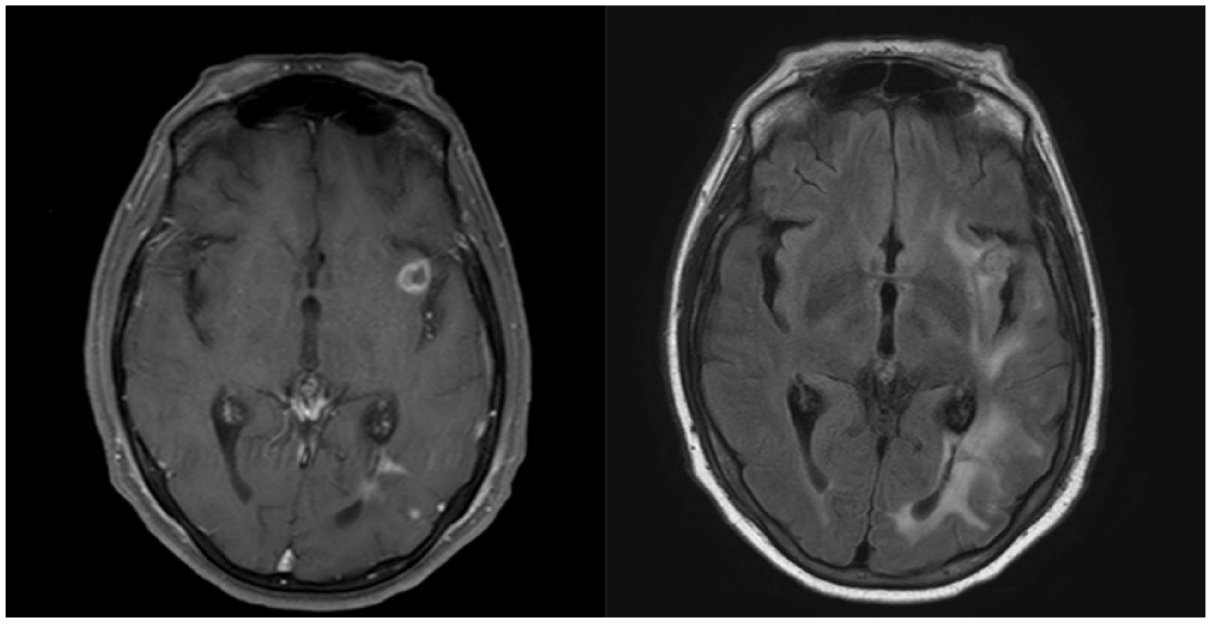
Imaging findings of PTLD on MRI. Axial brain images of a patient presenting with CNS-PTLD. (a) T1-weighted post-gadolinium image shows a focal ring enhancing lesion in the left sub-insular region. (b) T2 weighted image (T2/FLAIR) with perilesional edema compromising the left hemisphere.
For more than 30 years, the primary approach to PTLD treatment has been the reduction of immunosuppressive therapy. However, in transplant recipients, this strategy can increase the risk of GVHD or graft rejection and may have limited efficacy, resulting in complete resolution in only around 10% of patients after 3–6 weeks. 110 In most cases, specific treatments are required, and the choice may depend on the type of PTLD. For CNS-localized PTLD, in addition to immunosuppression reduction, optional therapies described are IV rituximab as monotherapy, or in combination with other chemotherapeutic medications. 111 In early PTLD, acyclovir and ganciclovir antivirals may be used. However, the effectiveness and impact of these anti-EBV medications remain uncertain, as they are typically used in combination with reduction of immunosuppression and anti-CD20 therapy.57,112
Other treatment options for CNS-PTLD, aligned with protocols used for primary CNS lymphoma, include high-dose methotrexate, cytarabine, and whole-brain radiation therapy.3,113 However, these intensive approaches are associated with significant toxicity and secondary effects that may increase mortality. 114 A multicenter study, the largest published to date, reported the effectiveness of combining whole-brain radiation therapy with IV rituximab for treating CNS-PTLD. All patients treated experienced no relapse afterward. However, despite the treatment’s efficacy, its toxicity was associated with an increased risk of infections, leading to the death of six patients. 115
Alternatively, some studies have explored alternative treatments. For instance, Dugan et al. reported 13 patients with EBV-positive CNS-PTLD treated with zidovudine, ganciclovir, dexamethasone, and IV rituximab, with an overall response rate and estimated 2-year survival of 92% and 76.9%, respectively. 116 Other therapeutic options with higher efficacy and minimal toxic effects are still being experimented on and must be evaluated in clinical trials. 58
Neuroinvasive presentations of classical M. tuberculosis infection
Among all forms of TB infection, CNS is involved in 10% of the overall cases and 20% of immunocompromized patients, causing the highest mortality out of all types of presentations.117,118 Typically, it occurs due to the spread of infection through the bloodstream from distant sites, often originating from the lungs or, in rare instances, as a result of direct spread from the paranasal sinuses, mastoid sinuses, or orbits. Once it enters the CNS, it provokes a strong granulomatous response, leading to a spectrum of presentations due to intracranial invasion. There are two primary manifestations of CNS tuberculosis: meningitis and parenchymal tuberculosis, which may co-occur. Meningitis, the most prevalent presentation, can manifest as leptomeningitis or pachymeningitis. In parenchymal tuberculosis, tuberculomas represent the second most common form of intracranial tuberculosis. However, other less common pathologies, considered atypical due to their low prevalence, include miliary tuberculosis, cerebritis, pseudo abscesses, encephalopathy, rhombencephalitis, and sellar-suprasellar tuberculosis.
The incidence of CNS tuberculosis cases is on the rise, marked by increasingly complex and atypical presentations, attributed in part to an increasing multidrug-resistant TB. 118 Notably, atypical patterns of neurotuberculosis are more likely to manifest in patients with immunosuppression, such as those with HIV/AIDS, posttransplant recipients, and individuals using immunosuppressants as the primary treatment for various diseases. Traditional diagnostic approaches, including serological techniques and tissue biopsy, can be time-consuming and may result in diagnostic delays. Hence, it becomes crucial to be familiar with the distinct radiological features that characterize typical and atypical presentations of CNS tuberculosis. 119 Recognizing intracranial TB is particularly challenging, given its potential to mimic other pathologies such as tumors, stroke, or encephalitis from other causes. Therefore, it is essential to consider diagnostic alternatives carefully and remain vigilant for atypical presentations in these cases.
Miliary tuberculosis is a rare and lethal presentation that is more likely to present in immunocompromized and malnourished patients. It constitutes up to 2% of all TB cases and is occasionally associated with tuberculous meningitis. 120 The clinical course can be either subacute or chronic, characterized by subtle neurological signs and symptoms that range from nonspecific behavioral/cognitive changes to focal neurological abnormalities. On MRI, these lesions exhibit features of multiple nodular structures measuring less than 2 mm, predominantly located in the cortico-medullary junction and distributed through the territory of perforating vessels. 118 They might appear similar to intracranial metastases on MRI scans, but advanced imaging techniques such as dynamic-susceptibility contrast MR perfusion can help distinguish them. Metastases typically exhibit higher cerebral blood volume and cerebral blood flow than tuberculomas. Another method for differentiation is diffusion tensor imaging, which should reveal a higher fractional anisotropy value in tuberculomas compared to metastases, suggesting more significant damage to the microstructure of white matter fibers. 121
Tuberculous cerebritis is a focal infection of the cerebral cortex caused by tuberculous bacilli that may occur in isolation or in conjunction with meningitis. 117 It was first described in 1988 by Jinkins, who reported five cases characterized by symptoms such as headaches, seizures, and, in one case, focal neurological deficits. 122 This condition is a singular clinicoradiological entity with characteristic features, though these features are not exclusive to CNS tubercular infection. On MRI, a gyriform hypointensity is observed on T1W, and a gyriform hyperintensity on T2W imaging. Contrast administration reveals focal patchy enhancement in the affected area of the cerebral cortex. 121
Tuberculous encephalopathy, a rare pathology, was initially documented in 1966 by Udani, who reported 20 cases either isolated or associated with meningitis or hemorrhage. 123 The condition is primarily characterized by diffuse cerebral damage, and since its first description, various theories regarding its pathophysiology have emerged. It was initially believed to be linked to a post-infectious delayed type IV hypersensitivity reaction due to a cell-mediated immunological response to tuberculous protein. 124 However, alternative theories propose a connection to hypoxia-ischemia or secondary to anti-tuberculous agent toxicity. 124 Its clinical presentation can vary between cognitive dysfunction, seizures, and/or altered mental status (stupor or coma). 118 Signs of meningeal irritation are usually absent unless it is related to tuberculous meningitis. On MR imaging, tuberculous encephalopathy reveals hyperintense white matter lesions on T2W imaging due to severe edema and demyelination. Also, diffuse post-contrast enhancement in the affected areas might be seen.117,118,121 On MT imaging, there is a characteristic reduction in the MT ratio in the white matter. 118
Typically, CNS tuberculosis is diagnosed on the basis of clinical findings, CSF culture/staining, and neuroimaging. However, given the atypical clinical presentations in immunocompromized patients, the poor sensitivity, and lack of efficiency in detecting M. tuberculosis infection, alternative diagnostic techniques should be considered. CSF Adenosine Deaminase (ADA) has emerged as a promising diagnostic tool for tuberculous CNS infection in adults, demonstrating a sensitivity of 0.85, specificity of 0.90, and diagnostic odds ratio of 48. 125 Another alternative to CSF culture, is the GeneXpert MTB/RIF assay, which provides rapid results (in less than 2 h) and is characterized by a sensitivity of 36.36% and specificity of 96.63%. 126 Other newer diagnostic techniques including a new lipoarabinomannan test (FujiLAM), transcriptomics, and CRISPR technology to help diagnose CNS tuberculosis have also been evaluated. 127 Additionally, ongoing studies are exploring advanced imaging techniques such as 3-D magnetization rapid gradient-echo and phase-contrast MRI to assess altered CSF flow dynamics in CNS tuberculosis. 128
Treatment for CNS tuberculosis consists of 9–12 months of the standard anti-tuberculous therapy for pulmonary forms. Adjuvant corticosteroid therapy should be implemented in all types of CNS tuberculosis, and when necessary, additional treatment for complications should be warranted (acetazolamide, osmotic diuretics, or shunt surgery for hydrocephalus). 129 Rifampin, Isoniazid, Pyrazinamide, and ethambutol should be given for 2 months, followed by a minimum of 7 months of rifampin, isoniazid, and ethambutol. If patients have compromised vision or cannot have regular follow-ups, ethambutol might be replaced by streptomycin, levofloxacin, or ethionamide. Although streptomycin should be avoided in pregnancy, hearing loss, or renal disease.
Conclusion
Patients who have undergone transplantation or are receiving immunosuppressive or immunomodulatory treatments for autoimmune or inflammatory conditions face an increased risk of CNS infections. This significantly raises their morbidity and mortality, highlighting the need for a thorough assessment of each patient. Critical considerations in these patients include the timing of infection, especially post-transplantation, existing comorbidities, medication regimens (immunosuppressive or immunomodulatory), and their specific effects on the immune system. It is crucial to recognize typical and atypical clinical presentations, consider various diagnostic tests suitable for immunocompromized patients, and establish treatment according to each individualized context after evaluating the mentioned variables. Further studies are required to optimize diagnostic evaluation and treatment approaches in these complex conditions.