
Abstract
Background:
Hospitals within Nairobi County, Kenya, offer cervical cancer screening services. However, most female sex workers do not seek this service.
Objective:
To determine uptake of cervical cancer screening among female sex workers living with HIV in Nairobi, Kenya.
Design:
A descriptive cross-sectional study.
Methods:
Computerized simple random sampling was used to select 75 study participants who met the inclusion criteria; data were collected using a structured questionnaire. The study was carried out among female sex workers living with HIV in Nairobi, Kenya, attending the Sex Workers Outreach Program.
Results:
40% (n = 30) of respondents were aged 18–25 years. Only 45.3% (34) had been screened for cervical cancer within the last 1 year. 65.3% (n = 49) of respondents knew that cervical cancer affects the cervix but were not aware of what caused the disease. 77.6% (n = 58) found the 8 am–5 pm health facility opening hours a hinderance to seeking services and 66.7% (n = 50) found the screening method uncomfortable. Cultural practices and beliefs fostered stigma in 39.2% (n = 29) of the sex workers; hence, they did not seek out services.
Conclusion:
Lack of information, cultural barriers, and facility operating hours prevent female sex workers living with HIV from getting tested for cervical cancer. These barriers once addressed could improve cervical cancer screening uptake among this high-risk population.
Background
Cervical cancer is a disease of the female gender that causes deterioration of a woman’s health if not diagnosed and treated early. 1 Female sex workers (FSWs) are of public health concern globally because they have multiple sexual partners, 2 and having many sexual partners makes them more exposed to human papilloma virus (HPV) than women from the general population. 3 Moreover, women living with HIV and selling sex have higher chances of progressing to cervical cancer compared to women living without HIV. 4
Although HIV is not a direct cause of cervical cancer, the risk is greatly aggravated among women living with HIV. This risk is compounded by the complex interplay of various factors, including HPV infection, 5 a weakened immune system, progression of cervical pre-cancerous lesions, and the heightened likelihood of engagement in risky sexual behaviors. Specifically, HIV attacks the immune system, thus weakening its ability to clear infections such as HPV and other opportunistic infections. The persistent and prolonged exposure to high-risk HPV strains increases the risk of cervical cancer development. 6 Additionally, HIV may accelerate the progression of pre-cancerous cervical lesions to invasive cancer. These pre-cancerous changes in the cervix can go unnoticed for years in people with healthy immune systems, but they may progress more rapidly in those with HIV. It has been well established that early detection, regular cervical cancer screening, such as pap smears or HPV testing, and treatment of pre-cancerous lesions are essential. FSWs are at risk of contracting both HIV and HPV due to their nature of work, hence the need for frequent cervical cancer screening as per the World Health Organization guidelines. 7
Most countries in Africa criminalize and stigmatize sex work. 8 HIV and cancer are also stigmatized, hence creating a triple burden to FSW living with HIV. 9 In 2020, only 15% of women of reproductive age in Africa were screened for cervical cancer, with no specific data on FSW. 10 As much as FSW remain anonymous during screening, 10 lack of FSW living with HIV specific data collection tools play a major role in missed opportunities to collect the desired data. Poor uptake of cervical cancer screening among women of reproductive age has been associated with ignorance and lack of knowledge. 11
About 39.6% of women of reproductive age are at risk of developing cancer because they harbor HPV. 12 While WHO recommends the use of the simple low-cost inspection methods for cervical cancer screening (visual inspection with acetic acid and visual inspection using Lugol’s iodine and early treatment initiatives), there is limited documented evidence on the uptake of this intervention in sub-Saharan Africa, especially among FSWs living with HIV. In Kenya, it is estimated that only 5% of FSW living with HIV sought screening for cancer of the cervix in 2019. Barriers identified that contribute to the poor uptake include fear of knowing the results, poor knowledge about cervical cancer screening, and fear of the screening procedure according to the International Agency for Research on Cancer Organization. 13
The main study objective was to determine the uptake of cervical cancer screening among FSWs living with HIV in Nairobi, Kenya.
Study methods
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 14
Study settings and population
This study took place from August 2022 to January 2023 and was a cross-sectional descriptive study that used a structured questionnaire with both closed and open-ended questions. The study population was FSW of reproductive age, living with HIV and residents of Nairobi County and its environs, who attended the Sex Workers Outreach Program (SWOP) health facilities for at least a year prior to data collection. SWOP is a network of FSW-friendly health facilities in Nairobi, offering free sexual reproductive health and HIV services that include free cervical cancer screening. It does not cater for FSW’s transport to and from the facility.
Inclusion criteria
FSWs living with HIV, 18–49 years, attending the SWOP in Nairobi, Kenya.
Exclusion criteria
FSWs not meeting the inclusion criteria as above. Those meeting the inclusion criteria but not able to consent on their own will, due to illness or personal choice, were excluded from the study.
Data collection tools and procedure
Data were gathered through a structured questionnaire with both closed and open-ended questions. Two study sites were purposively selected among the ten SWOP facilities. The questionnaire pretesting was done in a SWOP facility that was not one of the study sites. 10% (8) of the questionnaires were pretested and questions adjusted accordingly. The study participants who met the eligibility criteria were subjected to a simple randomization computer generated sequence process using the facility registry. Written informed consent was sought from all participants and questionnaires were administered by trained research assistants. Confidentiality was observed throughout the research processes.
Sample size calculation
The study utilized the Fisher et al., formula, with a 95% confidence level with a margin error set at 0.05. 15 Yamane’s (1967) formula was used because the sample population of FSW living with HIV attending SWOP facilities was less than 10,000; hence, the study sample size was 75. Attrition was done at 5%, which projected the sample to 79; however, the response rate was 75, which translated to 100% in most questions.
Statistical analysis
The quantitative data gathered using the questionnaire were categorized according to the goals and any errors corrected before coding and entry into SPSS (Nairobi, Kenya) version 25 software for analysis. The descriptive statistics were presented in tabular form as frequencies and percentages.
Results
The collected data highlighted lack of knowledge, cultural beliefs, long waiting time at the facility, and opening hours as barriers to cervical cancer screening services uptake among FSWs living with HIV.
Demographic data of the respondents
Most of the respondents—76.0% (n = 57)—were below the age of 30 years, with 40% (n = 30) being young FSW living with HIV aged 18–24 years. 64%(n = 48) of the respondents were single.
Uptake of cervical cancer screening
Of the 75 FSWs living with HIV, only 45.3% (n = 34) reported to have been screened for cervical cancer within the past 1 year.
Knowledge related factors affecting uptake of cervical cancer screening
A significant proportion of the study participants—20% 15 —were not aware what part of the body was affected by cervical cancer. However, 50.6 % (n = 38) of the participants knew that cervical cancer screening was important in promotion of early diagnosis and treatment. 44.0% (n = 33) of respondents knew that regular cervical cancer screening, getting HPV vaccine, using a condom while engaging in sexual intercourse, and having one partner were some of the methods used to protect one from getting cervical cancer or promoting early diagnosis and treatment.
Barriers to cervical cancer screening among FSW living with HIV
Health-facility-related barriers—routine
Inflexible facility opening hours hindered 77.3% (n = 58) of the FSW living with HIV from seeking screening services. 16% (n = 12) said health facilities should open 24 h, while 6.7% (n = 5) preferred weekend facilities. On affordability of the services, only 16% (n = 12) said they were able to financially take up the services (although the initial screening was free of charge). 66.7% (n = 50) were not comfortable taking up screening. On distance covered to the facility offering services, 36.0% (n = 27) traveled more than 10 km, 25.3% (n = 19) traveled 9–10 km, while 16% (n = 12) traveled 2–4 km. Being healthy influenced screening, with 86.7% (n = 65) saying that feeling well made them delay seeking screening services. In addition, 61.3% (n = 46) said those with signs should be screened, while 25.3% (n = 19) said screening should be done under a doctor’s recommendation (Table 1).
Knowledge and barriers of cervical cancer screening among FSW living with HIV.
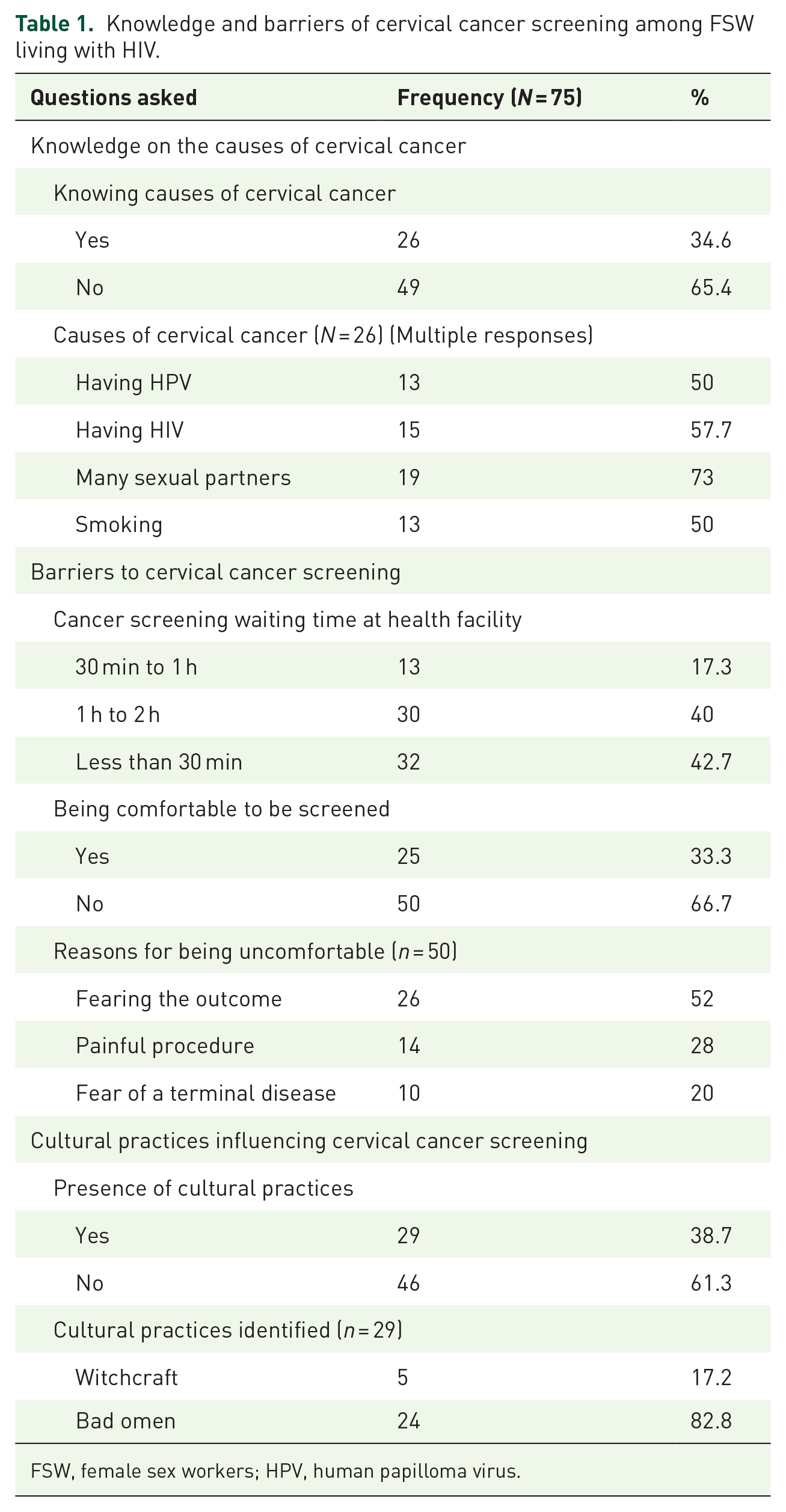
FSW, female sex workers; HPV, human papilloma virus.
Discussion
This study has shown a knowledge gap on the importance of cervical cancer screening and ways to prevent cervical cancer among this population of FSWs living with HIV, of whom the majority were of a young age. Some health facility factors contributed to poor uptake of cervical cancer services, despite free services being available. Culture also was a contributory hindrance to seeking cervical cancer screening services.
The majority (76.0%) of the study respondents were aged below 30 years, with 40% being young FSW. As demonstrated elsewhere, 16 young FSW living with HIV are exposed to a wide range of sexual reproductive health issues, including HPV and subsequent cervical cancer, hence the need for frequent screening. Despite 50.6% of the FSW living with HIV knowing the importance of cervical cancer screening, other factors such as feeling healthy contributed to low levels (45%) of screening uptake in this study, and this was equally demonstrated by a studies done in Kenya 17 and in Ethiopia. 18 Despite women being aware of the benefits of cervical cancer screening, most did not seek the services as prescribed by cancer screening guidelines. However, the Ethiopian study 18 showed that increased knowledge on the importance of cervical cancer screening among women of reproductive health promotes behavior change and increasing uptake of services.
Knowledge of cervical cancer should be a prime factor in promoting screening services. However, this study showed that 65.3% of the study participants were not aware of cervical cancer causes. This was also seen in a study in Bangladesh, 19 which showed that the majority of FSW living with HIV who did not know the causes of cervical cancer did not understand why screening was important. Cervical cancer prevention knowledge was lacking among 56.4% of the FSW living with HIV in this study, similar to other studies 20 where FSW living with HIV who were interviewed did not know measures for preventing cervical cancer. FSW living with HIV with poor knowledge on preventive measures of cervical cancer may not seek cervical cancer screening services, which contribute to low uptake of the service, despite their higher risk.
Regarding the distance to the facility, 62.5% said the facility was more than 8 km away, and this affected their cancer screening uptake. This is similar to study done in the USA 21 where FSW living with HIV who had low access to health centers had poor uptake of cervical cancer screening. Shorter distances to health facilities are likely to promote cancer screening among FSW living with HIV. The longer the distance to the facility, the more the money will be used for transport. Given the distance and the monetary needs, the majority of FSW living with HIV (84%) found cervical cancer screening not affordable, which agrees with a review in Sub-Saharan Africa, 22 where the total cost of accessing screening among FSW living with HIV influenced the uptake of services.
The screening process was reported to be an issue where 61.7% of FSW living with HIV were not comfortable with it; the majority feared the outcome and exaggerated the pain of the procedure. This could easily contribute to poor uptake of the services as reported in a study done by Joshi et al., 23 where FSW refused to take up cervical cancer screening due to fear of the outcome.
This study showed that 39.2% of FSW living with HIV feared accessing cervical cancer screening due to stigma instigated by culture and beliefs of the community pertaining to cancer. This was also reported in a study in Uganda 24 where cultural practices had an effect among FSW, whereby cervical cancer was viewed as a result of promiscuity. Similarly, sex work was considered as a taboo issue, which made FSW shy away from being screened.
The lack of flexible opening hours of the health facility was not favorable to 77.6% of the FSW living with HIV. A study in Hong Kong 25 demonstrated that considering the unpredictability of FSW’s work flexibility of health facility opening hours promoted cervical cancer screening.
Study limitations
The sample size was small due to the population of FSW living with HIV attending SWOP facilities being small. The HIV incidence and prevalence in this population has been reducing over time as a result of successful HIV prevention programing. 26 The study cost implication was also a limiting factor, as the study was not funded.
Conclusion
Lack of knowledge on the causes of cervical cancer, not knowing measures of preventing cervical cancer, long waiting time and distance to the facility, non-flexible facility opening hours, and uncomfortable screening procedure contributed to poor uptake of cervical cancer screening among FSWs living with HIV.
Recommendations
The study recommends that strategic health messages should be targeted toward all FSW living with HIV, especially the young, to increase uptake of cervical cancer screening. Policy makers at each level should consider flexible facility opening hours that work for FSW living with HIV and should also consider opening more friendly FSW living with HIV facilities across the country and ensure that cervical cancer screening is offered among other services. More studies need to be done on cervical cancer friendly screening procedures to enhance uptake.
Supplemental Material
sj-doc-1-tai-10.1177_20499361241284238 – Supplemental material for Uptake of cervical cancer screening among sex workers living with HIV in Nairobi, Kenya: a cross-sectional study
Supplemental material, sj-doc-1-tai-10.1177_20499361241284238 for Uptake of cervical cancer screening among sex workers living with HIV in Nairobi, Kenya: a cross-sectional study by Maureen Akolo, Lawrence Gelmon, Horatius Musembi, Benard Mutwiri, Isabel Kambo, Joshua Kimani and Christopher Akolo in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-docx-2-tai-10.1177_20499361241284238 – Supplemental material for Uptake of cervical cancer screening among sex workers living with HIV in Nairobi, Kenya: a cross-sectional study
Supplemental material, sj-docx-2-tai-10.1177_20499361241284238 for Uptake of cervical cancer screening among sex workers living with HIV in Nairobi, Kenya: a cross-sectional study by Maureen Akolo, Lawrence Gelmon, Horatius Musembi, Benard Mutwiri, Isabel Kambo, Joshua Kimani and Christopher Akolo in Therapeutic Advances in Infectious Disease
Footnotes
Acknowledgements
Sex Workers Outreach Program. Aga Khan University-School of Nursing and Midwifery. INTEREST Conference 2023. Dr Baluku for mentorship in writing of this article. Female sex workers from the Sex Workers Outreach Program, Nairobi, Kenya.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.