
Abstract
Background:
Recently recognized by the World Health Organization as a neglected tropical disease, Noma, an acute and destructive gangrenous disease affecting the gums and facial structures within the oral cavity, has a high mortality rate if untreated.
Objectives:
To investigate the prevalence and impact of Noma among internally displaced populations in Northeastern Nigeria.
Design:
A retrospective study.
Methods:
This retrospective study investigates the prevalence and impact of Noma among internally displaced populations in Northeastern Nigeria. Noma is endemic in Northern Nigeria, Africa, and its occurrence has been linked to extreme poverty, malnutrition, poor hygiene, and inadequate healthcare – conditions exacerbated by the ongoing Boko Haram conflict.
Results:
The retrospective descriptive cross-sectional analysis of 17 cases reveals a median age of 8 years, with most of the patients being children who suffer significant social stigmas, such as difficulties in speaking, eating, and social integration, including reduced school attendance and marital prospects.
Conclusion:
The study highlights the urgent need for comprehensive research into the etiology of Noma and its socio-economic impact. It emphasizes the necessity for early and effective intervention strategies, particularly in conflict-stricken areas with limited healthcare access.
Keywords
Introduction
Noma, also known as Cancrum oris, a severe and aggressive gangrenous periodontal disease that mainly affects the oral cavity and face, 1 was added to the World Health Organization (WHO) list of neglected tropical diseases (NTDs) on 15 December 2023.2,3 The disease has six progression stages: Stage 0 – Simple gingivitis; Stage 1 – Acute necrotizing gingivitis; Stage 2 – Edema; Stage 3 – Gangrene; Stage 4 – Scarring; and Stage 5 – Sequelae. The advanced stage of the disease is characterized by extensive and severe maxillofacial tissue destruction, leaving infected persons severely disfigured (Figure 1(a) and (b)). Early intervention is crucial as Noma is highly fatal (80–90%) if left untreated, 4 with a disability-adjusted life year (DALY) of about one to ten million and a global incidence of about 30,000 to 40,000 cases annually. 5

A patient diagnosed with Noma, (a) pre-surgery, (b–d) post-surgeries, and (e) a map illustrating the migration patterns of displaced individuals into Adamawa State, Nigeria, with arrows indicating the primary routes from neighboring Borno States and LGAs. LGA, local government area.
Noma is endemic in some parts of Africa, particularly sub-Saharan Africa, the ‘Noma belt’,6,7 where the prevalence is high. In Nigeria, the disease is endemic in Northern region of the country, and its occurrence has been linked to extreme poverty, malnutrition, poor hygiene, and inadequate healthcare – conditions exacerbated by the ongoing Boko Haram conflict.8,9 internally displaced persons (IDPs), especially children, have become vulnerable to hunger and malnutrition, which, aided by the weakened healthcare system, makes the displaced persons susceptible to diseases such as Noma.
This study aims to investigate the demographic and clinical profiles of Noma patients within IDPs in Northeastern Nigeria, to uncover key factors that could inform effective health interventions. Understanding the interplay between conflict, displacement, and health is crucial for tackling Noma. Therefore, this study offers unique insight into how socio-political instability influences disease dynamics and patient outcomes. By evaluating pre- and post-surgical outcomes, we highlight the critical demand for targeted healthcare interventions and specialized health services and contribute to the broader global health to control and eliminate Noma.
Methods
A retrospective descriptive cross-sectional study was conducted at a tertiary institution in Borno, Northeastern Nigeria, from March 2021 to March 2022. The study cohort comprised a total of 17 Noma cases among IDPs (Figure 1). Cases were identified through hospital records, and a Noma case was confirmed diagnosis by a medical specialist. Socio-demographic and clinical data were collected pre-surgery and a post-surgery survey for consented individuals who underwent intervention.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 10
Results
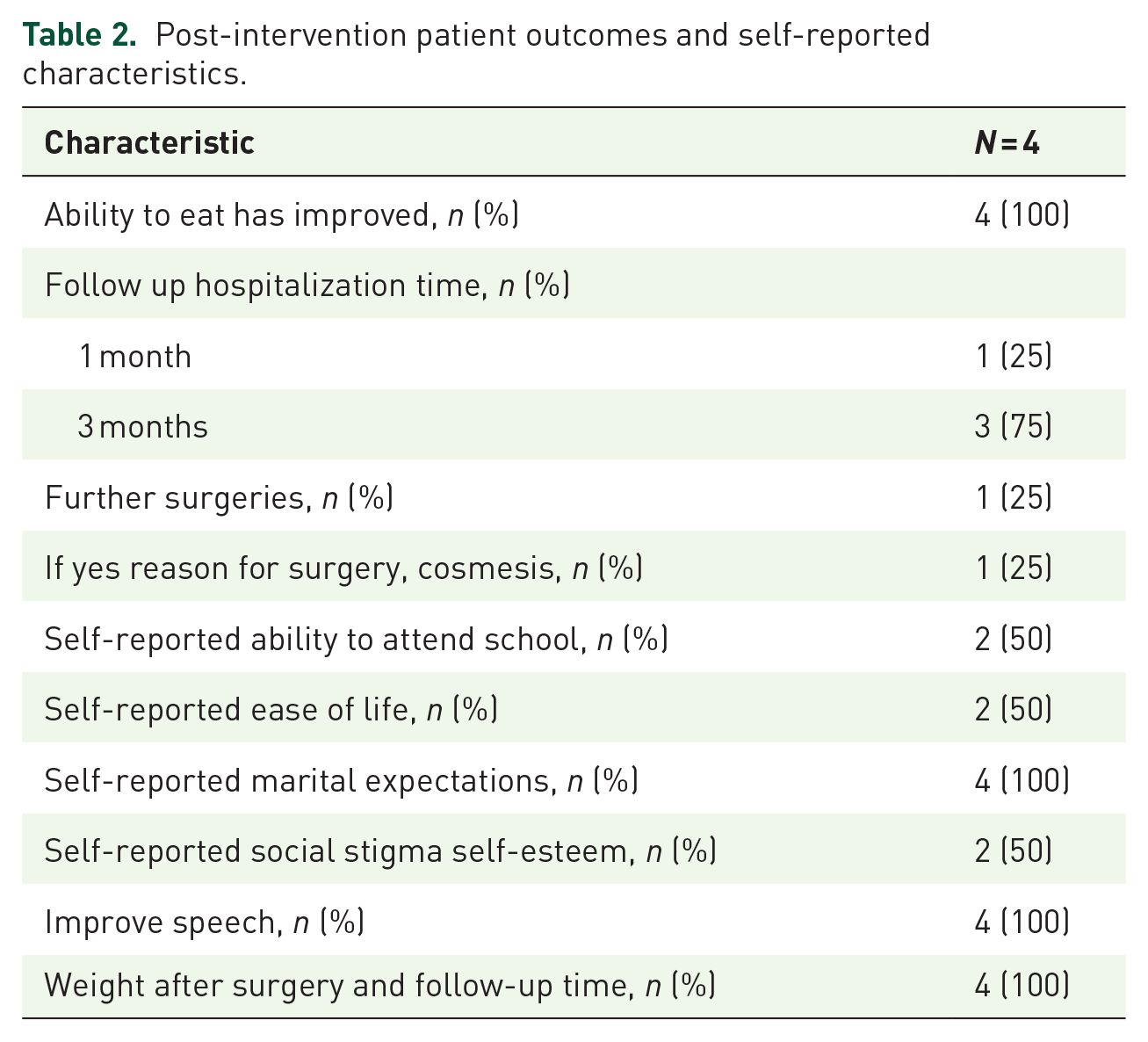
The pre-surgery socio-demographic and clinical characteristics of the 17 cases are presented in Table 1, and the post-surgery survey for four consented individuals who underwent intervention is presented in Table 2. The median age of the study cohort is eight years, with males accounting for 53% of the total patients. Children under five accounted for 41% of the cases. Moreover, the social impact of Noma was notable, with 41% being unable to attend school and 24% unable to marry due to the disease. Clinically, the manifestations of Noma were profound, with 29% presented severely limiting jaw movement (ankylosis), 82% experienced difficulties in speaking, and 65% reported eating challenges. Facial disfigurements, a particularly distressing outcome, and socially stigmatizing effects of the disease were evident in this study, with a high level of disfigurement in 35% of patients, medium in 35%, and low in 29%. Most patients had undergone one surgical intervention (59%), with nearly half of the patients having lived with the disease for up to 2 years before receiving treatment.
Pre-surgery patient demographic and clinical characteristics.
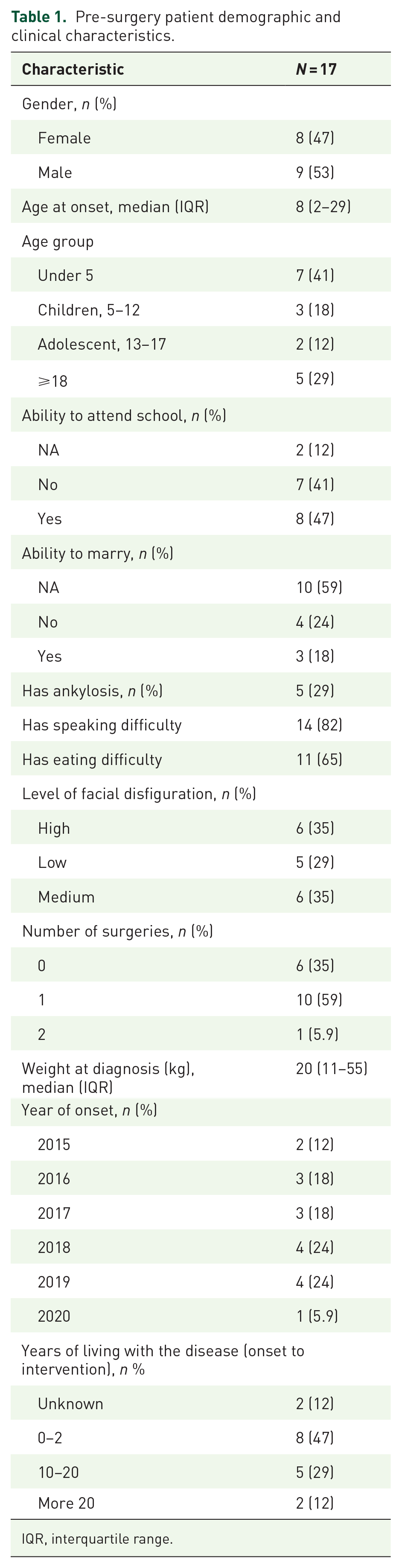
IQR, interquartile range.
Post-intervention patient outcomes and self-reported characteristics.
Discussion
Our study shows that Noma predominantly affects children, which confirms existing research; however, the children in this study are IDPs due to Boko Haram insurgency. These IDP camps are often overcrowded, unhygienic, and lack access to food and essential healthcare. 11 These poor living conditions predisposed the population to diseases like Noma. 11 Noma is associated with extreme poverty, poor hygiene, malnutrition, and poor living conditions. 9 Poverty results in food insecurity, which leads to malnutrition and undernutrition.8,12 Noma mostly affects the most marginalized groups globally. 13 The vulnerability of these communities to Noma is further exacerbated by factors such as internal displacement and war. In Northeast Nigeria, the Boko Haram conflict, which began in 2009, has resulted in a humanitarian crisis that led to the collapse of the already dilapidated and ineffective healthcare system in the region. 14
Based on a recommendation from the Strategic and Technical Advisory Group for NTDs, Noma has recently been included in the World Health Organization’s list of NTDs that are being targeted for control and eradication by 2030.3,6 The potential for conflict and displacement to worsen the Noma vulnerability cannot be overlooked. Identifying additional risk factors could enable us to predict an individual’s risk of contracting the disease, and further research is needed in these areas.
In addition, the functional and social impacts of Noma were evident in the study and are cause for significant concern. Survivors reported a limited range of jaw movement, speaking and eating difficulties, inability to marry due to stigma, and discontinuation of education, reflecting the extensive social stigma and disruption caused by the disease. Furthermore, the high proportion of facial disfigurement reported underscores the need for comprehensive care that includes not only medical but also psychological and social support.
Most patients undergoing only one surgical intervention point to the necessity for ongoing medical care. With nearly half of the patients enduring the disease for up to 2 years before treatment, our study calls attention to the urgent requirement for early detection and intervention. Post-surgery outcomes indicate improvements in eating ability and speech, suggesting that surgical intervention positively impacts quality of life, consistent with previous studies in Sokoto, Nigeria. 15 However, the enduring social stigma, as reported by half of the patients post-intervention, signals the need for broader societal engagement and education to mitigate the prejudice associated with Noma. This is particularly critical since, in certain societies, the disease is often linked to bad omens or spirits, resulting in the ostracization of patients and their subsequent reluctance to seek or accept medical help. 16
Conclusion
In summary, our findings indicate that more research investigating the etiology, psychosocial, and economic impact of Noma, especially among high-risk populations, is required. The clinical burden of Noma, as demonstrated in this study, extends beyond its immediate health implications. It also underscores the critical need for early intervention and comprehensive care for affected individuals, particularly in conflict-affected areas where access to healthcare is often compromised.
Supplemental Material
sj-docx-1-tai-10.1177_20499361241261269 – Supplemental material for Noma disease among internally displaced persons in Northeast Nigeria: a retrospective descriptive study
Supplemental material, sj-docx-1-tai-10.1177_20499361241261269 for Noma disease among internally displaced persons in Northeast Nigeria: a retrospective descriptive study by Mohammed A. S. Abdullahi, Muhammad R. Balarabe, Jennifer A. Tyndall, Faith O. Alele, Abdulrazaq G. Habib and Oyelola A. Adegboye in Therapeutic Advances in Infectious Disease
Footnotes
Acknowledgements
We extend our heartfelt thanks to all the participants for their invaluable contributions and cooperation throughout this study. In addition, we express our profound gratitude to the University of Maiduguri Teaching Hospital, Maiduguri, Nigeria, for their unwavering support and facilitation of our research endeavors.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.