
Abstract
Background:
Despite the increased frequency of oropharyngeal candidiasis among people living with human immunodeficiency virus (HIV), its management is no longer effective due to empirical treatment and emergence of antifungal resistance (AFR). This study sought to investigate the prevalence of oropharyngeal candidiasis and assess the antifungal susceptibility profile of oropharyngeal Candida species isolated from people living with human immunodeficiency virus. Additionally, we evaluated the correlation between oropharyngeal candidiasis and CD4 T cell as well as viral load counts.
Methods:
A descriptive cross-sectional study was carried out from April to October 2023 in which 384 people living with HIV underwent clinical examination for oral lesions. Oropharyngeal swabs were collected and cultured on Sabouraud Dextrose agar to isolate Candida species which were identified using the matrix assisted laser desorption ionization time of flight mass spectrometry. Additionally, the antifungal susceptibility profile of Candida isolates to six antifungal drugs was determined using VITEK® (Marcy-l’Étoile, France) compact system. Data on viral load were retrieved from records, and CD4 T cell count test was performed using Becton Dickinson Biosciences fluorescent antibody cell sorter presto.
Results:
The prevalence of oropharyngeal candidiasis was 7.6%. Oropharyngeal candidiasis was significantly associated with low CD4 T cell count and high viral load. A total of 35 isolates were obtained out of which Candida albicans comprised of 20 (57.1%) while C. tropicalis and C. glabrata comprised 4 (11.4%) each. C. parapsilosis, C. dubliniensis and C. krusei accounted for 2 (5.7%) each. Additionally, 7 (20%) isolates were resistant to fluconazole, 1 (2.9%) to flucytocine and 0.2 (5.7%) isolates were intermediate to caspofungin. However, specific specie isolates like C. albicans showed 20% (4/20), C. glabrata 50% (2/4) and C. krusei 50% (1/2) resistance to fluconazole. Additionally, C. krusei showed 50% resistance to flucytosine.
Conclusion:
The prevalence of oropharyngeal candidiasis (OPC) among people living with HIV was low, and there was a significant association between OPC and CD4 T cell count as well as viral load. C. albicans was the most frequently isolated oropharyngeal Candida species. C. glabrata and C. krusei exhibited the highest AFR among the non-albicans Candida species. The highest resistance was demonstrated to fluconazole.
Introduction
Oropharyngeal candidiasis (OPC) is the most prevalent opportunistic superficial fungal infection in human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS). 1 The OPC is incident in about 90% of people living with human immunodeficiency virus (PLHIV) whose cell-mediated immune system become severely compromised when the CD4 T lymphocyte levels fall below 200 cells/μL and have increased viral load.2–4 In Uganda, it is approximated that 45,000 HIV/AIDS-related OPC occur per year with its prevalence ranging from 19.4% to 52% making it the most frequent opportunistic fungal infection among this cohort of patients.5–7
In order to improve the quality of life among PLHIV, Uganda rolled out the universal test and treat (UTT) policy in 2017 where PLHIV regardless of HIV clinical stage and CD4 cell count are initiated on lifelong antiretroviral therapy (ART) and patient viral load is used as an indicator for monitoring ART response.8–10 Prior to the inception of UTT, ART initiation was based on CD4 counts below ⩽500 cells/μL from the year 2013 to 2017, ⩽350 cells/μL from 2010 to 2013 and ⩽200 cells/μL from 2004 to 2010.9,10 Although CD4 cell counts have been the immunological predictor for OPC among PLHIV, increased HIV viral load has been reported as an important marker for the development of OPC once viral loads surpass 10,000 copies/ml. 11 However, there are no reports of studies on the evaluation of association between OPC, CD4 T cell count and viral load. Despite Candida albicans being the most causative agent of OPC, emerging non-albicans Candida species (NAC) such as C. kruzei, C. parapsilosis, C. glabrata, C. tropicalis, C. dubliniensis, C. guilliermondi and C. norvegensis have also been isolated from PLHIV.12,13
The rising incidence of OPC among PLHIV has consequently made empirical antifungal treatment the best option by clinicians to manage the infection. However, over dependence on these antifungals has led to increased AFR with noticeable shift towards antifungal-resistant NAC species.14,15 Consequently, the empirical management of OPC faces significant challenges. Accurate species identification and antifungal susceptibility testing are crucial for selecting appropriate treatment options. Therefore, there is a need for accurate identification and antifungal susceptibility profiling of oropharyngeal Candida species among PLHIV in Uganda.7,16 Thus, we conducted a cross-sectional study to determine the prevalence of OPC, its correlation with CD4 T cell and viral load, and antifungal resistance (AFR) profiles of Candida species isolated from PLHIV at the AIDS Support Organization (TASO) clinics in Uganda.
Materials and methods
Participants and study setting
This was a descriptive, quantitative and cross-sectional study carried out from April to October 2023. A total of 384 PLHIV of 18 years and above attending TASO clinics in Uganda including TASO Mulago National Referral Hospital and TASO Mbarara Regional Referral Hospital were recruited into the study. Pre-designed data collection form was used to collect information on demographics, clinical history, treatment and recent HIV viral load results from participants’ medical records.
Inclusion and exclusion criteria
This study included males and females of 18 years and above living with HIV on ART attending TASO Mulago National Referral Hospital and TASO Mbarara Regional Referral Hospital who consented to participate in the study. All participants who were on antifungal treatment within the last 4 weeks for prophylactic or therapeutic purposes were excluded from the study.
Sample size
A standard formula by Kish and Leslie was used to calculate the sample size of 384 for this cross-sectional study based on 52% prevalence of OPC among PLHIV in Southwest Uganda. 5
n = Z2 P(1 − P)/d2
n = study sample size required
Z = critical value associated with 95% confidence interval = 1.96
P = Estimated proportion of PLHIV with OPC
d = margin of error = 0.05
n = 1.962 × 0.52 × (1 − 0.52)/0.052 = 384
Sample collection and processing
The attending clinician did a clinical examination of the oral pharynx for clinical manifestations of OPC using a spatula and light source. Oropharyngeal swabs were collected by swabbing the dorsum of the tongue, palate, buccal mucosa and oropharynx using sterile cotton swabs for asymptomatic participants and OPC lesion sites for the symptomatic participants. The collected oropharyngeal swabs specimens were placed in Amies transport media and packaged in a leak proof zipper locking bags. The specimens were transported to the testing mycology laboratory at the Department of Microbiology, Makerere University within 24 h at a temperature of 2–8°C for analysis. Oropharyngeal candidiasis was defined as presence of oral lesions caused by Candida species isolated from oral cavity. Venous blood samples were collected in ethylene diamine tetra acetic acid vacutainers and CD4 T cell count tests were performed using the fluorescent antibody cell sorter presto (Becton Dickinson, Singapore, BD) Count system at TASO Mulago and Mbarara clinics.
Isolation of Candida species
For yeast isolation, oropharyngeal swab specimens were cultured on sabouraud dextrose agar (SDA) (Oxoid, Basingstoke, UK) supplemented with 50 μg/1 ml gentamicin and then incubated at 37°C for 48–72 h aerobically. The yeast isolates were emulsified in brain heart infusion broth (Oxoid, Basingstoke, UK) containing 10% glycerol and stored at minus 80°C in a deep freezer until further use.
Identification of Candida species
Yeast isolates were re-inoculated on SDA (Oxoid, Basingstoke, UK). Due to its higher specificity, sensitivity, cost effectiveness and rapid identification, matrix-assisted laser desorption ionization time of flight mass spectrometry (MALDI-TOF MS) BioTyper 4.1 system (Bruker Daltonics, Bremen, Germany) at the Department of Microbiology, Makerere University was used to identify Candida species as previously described by Bader et al. 17 Briefly, cells of approximately five colonies from SDA plates were suspended in 300 μL of water and inactivated by the addition of 900 μL of 96% ethanol. The cells were spun down, and the pellet was air-dried at room temperature, resuspended in 50 μL of 70% formic acid, and extracted by addition of an equal volume of aceto nitrile and thorough mixing. Cellular debris was removed by centrifugation, and 1 μL of the clear supernatant was spotted onto a polished steel carrier, allowed to dry, overlaid with 1 μL of HCCA (a-Cyano-4-hydroxycinnamic acid) matrix and allowed to dry again. Measurement was performed with the MALDI BioTyper 4.1 and Flex Control software on a Microflex LT20 mass spectrometer, using a yeast test standard (Bruker Daltonics) as a molecular mass standard. Spectra were detected in positive linear mode, with a mass range of 2–20 kDa. The intensity of the laser was controlled by the FlexControl software driven in automatic mode, at the settings recommended by the manufacturer. 19 Species identifications with scores >2.000 were accepted; whole proposed identification at the genus level was rejected. 17
Antifungal susceptibility testing of Candida species
Fresh SDA cultures of Candida species were prepared and incubated at 37°C for 24 h and the antifungal susceptibility (AFS) testing was determined by the automated VITEK® 2 compact systems version 08.01 (Biomerieux, Marcy-l’Étoile, France) using AST-YS08 cards as per the manufacturer’s instruction18,19 at the Department of Microbiology, Kiruddu National Referral Hospital. The VITEK® 2 compact system is an automated machine that is capable of rapidly and accurately evaluating antifungal drug susceptibility profile against Candida species. 20 The Vitek® 2 AST-YS08 yeast susceptibility system reflects Candida species-specific clinical breakpoints (CBPs) as stipulated in the Clinical and Laboratory Standards Institute (CLSI).19,21,23
The six antifungal drugs tested were amphotericin B, fluconazole, voriconazole, caspofungin, micafungin and flucytosine. Generally, inoculum suspensions were standardized to the McFarland scale 2.0 using the DensiChek densitometer of the VITEK® 2 system. The AST-YS08 cards were filled with the prepared inoculum suspension and then incubated at 35.5°C for 18 h using VITEK®-2 machine. Every 15 minutes during the incubation period, data were collected, and the final breakpoint minimum inhibitory concentration (MIC) values for fluconazole, voriconazole, amphotericin B, flucytocine and minimum effective concentration (MEC) values for caspofungin and micafungin were used to categorize each isolate as, susceptible (S), intermediate (I) or resistant (R) based on the Vitek® 2 breakpoint setting. MIC/MEC results were evaluated using advanced expert system software version 08.01 designed to evaluate the results produced by the VITEK® 2 system. Additionally, C. albicans ATCC 10231 control reference strain was used to evaluate VITEK® 2 system performance. The results were automatically read and printed by the Vitek® 2 machine after an incubation period of 18 h.
Data analysis
The raw data from data collection tools and laboratory forms were processed in Microsoft Excel before being imported to Stata (version 17), Stata Corporation, College Station, Texas, USA software for further analysis. Descriptive statistics was used to analyse for frequencies and percentages to present categorical variables; mean, median, standard deviation (SD) and interquartile ranges (IQRs) were used to present count and continuous variables. The cross-tabulations were used to present the distributions of different demographic and clinical characteristics with site of study, and results were presented in the form of tables and figures. To investigate the association between OPC with CD4 cell count and viral load, Pearson’s Chi-Square tests were used. For the distribution of Candida species and AFS profile, frequencies and percentages were used. A p-value of less than 0.05 was considered statistically significant.
Quality control
Clinical and laboratory procedures were performed by trained, competent, licensed clinicians and laboratory scientists to ensure quality results. Study protocols were adhered to, and culture media sterility was assessed before inoculation. C. albicans ATCC 10231 control reference strain was used to evaluate VITEK® 2 system performance. Data was double entered into the Excel spread sheet to ensure accuracy and reliability.
Results
Social demographic and clinical profile of study participants
In this study, a total of 384 participants were enrolled. Of these study participants, 239 (62.2%) and 145 (37.8%) were from Mulago and Mbarara TASO clinics, respectively. Overall, females were 291 (75.8%) as compared to males, 93 (24.2%) with a mean age of 43.5 (SD = 12.5) and median of 43 years (IQR = 34, 53). The biggest number were Catholics, Pentecostals and Protestant religions nominated for the study with a frequency of 128 (33.3%), 108 (28.1%) and 92 (24.0%) respectively. The majority of participants were married (30.2%) and had secondary education 189 (49.2%). A total of 148 (38.5%) and 118 (30.7%) were business people and farmers respectively.
Prevalence of oropharyngeal candidiasis
On the clinical evaluation of 384 participants, the majority were in clinical stages II and I, 247 (64.3%) and 117 (30.5) respectively. Generally, cultures of oropharyngeal swabs from 29 PLHIV with oral lesions were positive for Candida species confirming prevalence of OPC as 7.6% (29/384). Four different clinical forms of OPC were noted on examination, and pseudomembranous candidiasis was the most common clinical presentation of OPC 21 (72.4) (Table 1).
Social demographic and clinical characteristics.

ART, antiretroviral therapy; IQR, interquartile range; OPC, oropharyngeal candidiasis; SDA, sabouraud dextrose agar.
Clinical profile and correlation between OPC with CD4 cell count and HIV viral load
In terms of clinical profile, the median duration from date of HIV diagnosis and ART initiation was 9.6 years (IQR = 3.7, 14.0) and 10.8 years (IQR = 4.6, 15.3) respectively (Table 1). Majority of participants were in clinical stages 11 and I with frequency of 247 (64.3%) and 117 (30.5) respectively (Table 1).
Overall, the mean CD4 cell count among PLHIV was 724.55 (SD = 343.45), and a range of 9 to 2164 cells/mm3 was noted. The majority of PLHIV 279 (72.7%) had CD4 cell count above 500 (Table 2). The average CD4 cell count for 29 PLHIV with OPC was 374.59 (SD = 306.80) and OPC was noted in 14 (48.3%), 3 (10.3%), 3 (10.3%) and 9 (31.0) with CD4 cell counts ⩽200 cells/mm3, 201–350, 351–500 cells/mm3 and more than 500 cells/mm3 respectively. Low CD4 count was statistically associated with OPC (p < 0.001) (Table 2).
The correlation between OPC with CD4 cell count and viral load with OPC and clinical stage and duration on ART.
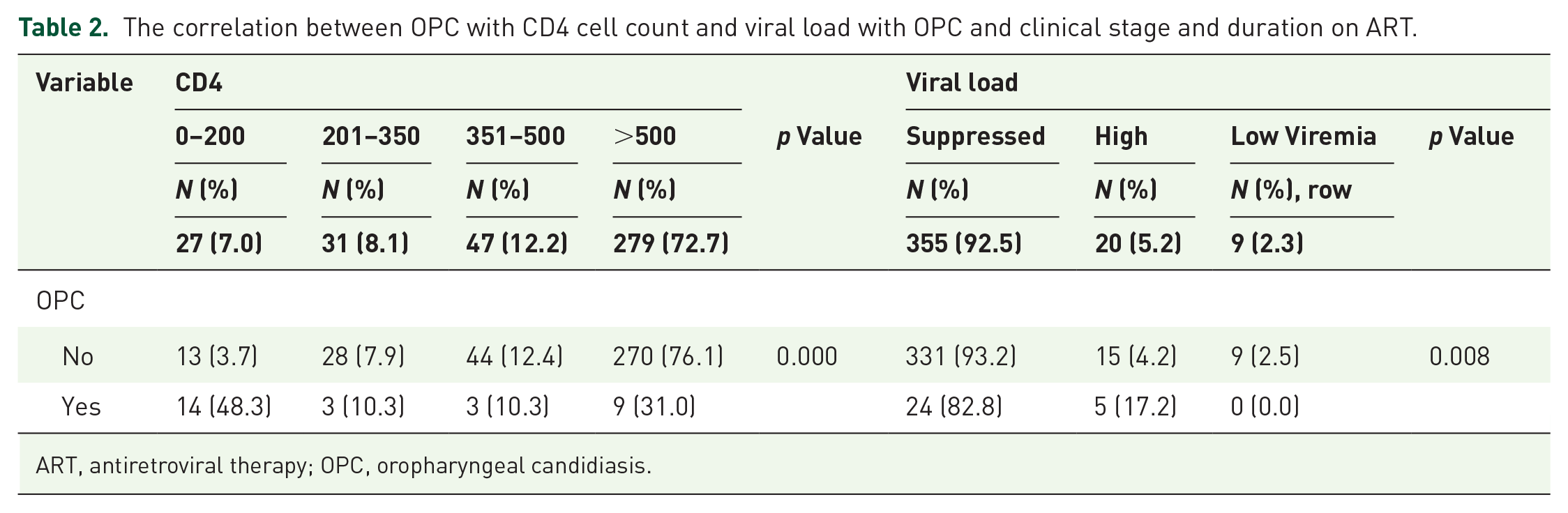
ART, antiretroviral therapy; OPC, oropharyngeal candidiasis.
About 355 (92.5%), 20 (5.2%) and 9 (2.3%) PLHIV had suppressed viral load, low viremia and high viremia respectively and OPC was noted in 24 (82.8%) and 5 (17.2%) for suppressed and high viremia respectively. Viral load was statistically associated with OPC (p = 0.008) (Table 2).
Distribution of Candida species
Oropharyngeal swab samples from 29 PLHIV with OPC yielded Candida species out of which 23 (79.3%) carried one type of Candida specie while 6 (20.7%) had two different species (C. albicans and NAC isolates).
Generally, out of 35 obtained Candida isolates, C. albicans and NAC comprised of 20 (57.1%) and 15 (42.9%) respectively. C. tropicalis and C. glabrata comprised 4 (11.4%) each while C. parapsilosis, C. dubliniensis and C. krusei accounted for 2 (5.7%) each and C. lusitaniae and accounted for 1 (2.9%) (Figure 1).

Frequency and distribution of various species of Candida among PLHIV with OPC.
The AFS profile of Candida isolates
The AFS of 35 Candida isolates to the six antifungal drugs fluconazole, voriconazole, caspofungin, micafungin, amphotericin B and flucytocine was determined using Vitek® compact system machine (Figure 2). Of the 35 tested isolates, 27 (77.1%), 35 (100%), 33 (94.4%), 35 (100%), 34 (97.1%) and 33 (94.4%) were susceptible to fluconazole, voriconazole, caspofungin, micafungin, amphotericin B and flucytosine respectively. In addition, 7 (20%) and 1 (2.9%) of isolates were resistant to fluconazole and flucytocine respectively. While each 1 (2.9%) of isolates were intermediate to fluconazole, amphotericin B and flucytosine, 2 (5.7%) of isolates were intermediate to caspofungin (Figure 2).
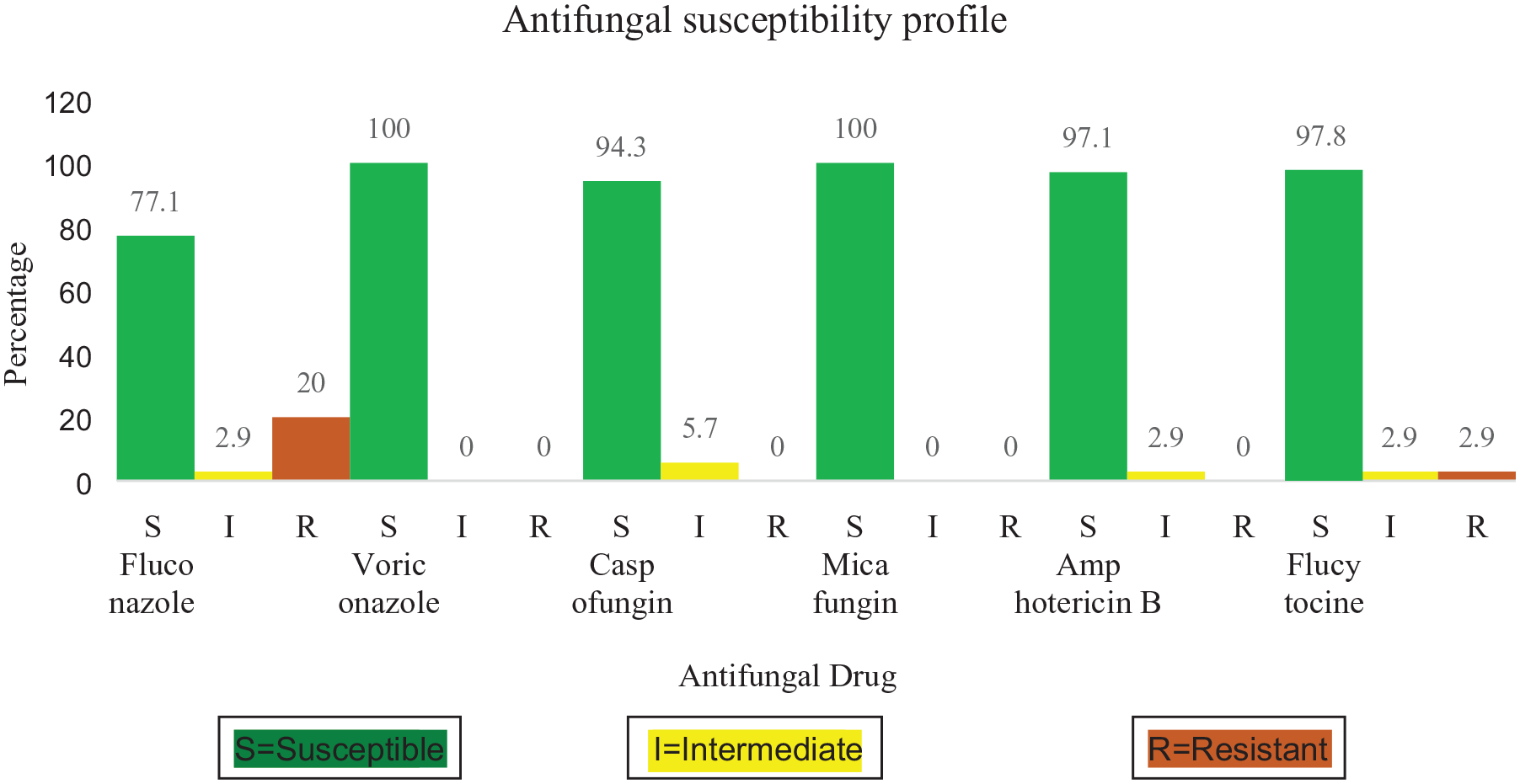
The antifungal susceptibility profile of Candida isolates.
Regarding different specific Candida species antifungal profiles, all isolates of C. tropicalis, C. parapsilosis and C. lusitaniae were 100% sensitive to all the six antifungal drugs. Out of 20 C. albicans, 15 (75%), 1 (5%) and 4 (20%) isolates demonstrated sensitivity, intermediate and resistance to fluconazole respectively and 1 (5%) was intermediate to amphotericin B. While C. glabrata and C. krusei showed 50% resistance to fluconazole each, C. glabrata demonstrated 50% intermediate to caspofungin. C. krusei showed 50% resistant to flucytocine while C. dubliniensis 50% intermediate to the same agent (Table 3).
The antifungal susceptibility profile of Candida species isolated from people living with HIV.

I, intermediate, 0 (0), No intermediate and/or resistant isolate(s) were recorded; R, resistance; S, sensitive.
Generally, the MIC values for fluconazole, voriconazole, amphotericin B, flucytocine and MEC values for caspofungin and micafungin were antifungal drugs against different Candida species were variable. The sensitivity MIC values of fluconazole (⩽0.5–2 μg/ml), voriconazole (⩽0.12–1), amphotericin B (⩽0.12–1 μg/ml), flucytocine (⩽1 μg/ml) and MEC values for caspofungin (⩽0.12–0.25 μg/ml), micafungin (⩽0.06–0.25 μg/ml) were recorded by Vitek® machine as shown in Table 4. The potencies of micafungin (0.06 μg/ml) and voriconazole (⩽0.12 μg/ml) were better than that of caspofungin (⩽0.12 μg/ml) and fluconazole (⩽0.5 μg/ml) respectively (Table 4).
Breakpoints of different antifungal drugs against Candida isolates as per results from the Vitek® machine.

I, Intermediate; R, Resistant; S, Sensitive; MEC, minimum effective concentration; MIC, minimum inhibitory concentration; −, No intermediate and/or resistant isolate detected and therefore no MIC values for fluconazole, voriconazole, amphotericin B, flucytocine and no MEC values for caspofungin and micafungin were recorded.
Discussion
Definitive aetiological and AFS profiling is vital in the management of OPC among PLHIV. 23 Here, we highlight the prevalence and profile of corresponding aetiology and antifungals susceptibility among PLHIV. We further examine the correlation between OPC, CD4 T cell count and HIV viral load. Specifically, the prevalence of OPC in this patient cohort was determined to be 7.6%. This is lower than that 52%, 75.3%, 34%, 37.5% and 42% previously reported in South western Uganda, Ghana, Chad and Ethiopia and Cameroon respectively.5,24–27 However, it was slightly higher than 4.9% determined in a Nigerian Tertiary Hospital. 28 but similar to 9.7% in Senegal, 29 12% in Tanzania 30 and 12.5% in Nigeria. 31 Generally, the low prevalence of OPC in our study could be due to effects of test and treat policy since all our participants were on highly active antiretroviral therapy (HAART) and were mostly in Stage I and II of HIV infection. Previous studies have reported that OPC is less frequent among PLHIV who are on ARVS (Antiretroviral drugs) as compared to ARVs naive patients.2–4,32 Highly active ARV therapy may improve immunity through immune reconstitution leading to elevation of CD4 cells and reduction of viral load. The reduction of OPC following HAART is attributed to immune reconstitution, as measured by the elevation of circulating CD4 cells and the reduction of the viral load. 33 Differences in diagnostic techniques, oral hygiene and geographic differences could be other factors responsible for variations in the prevalence of OPC as well.
Both CD4 count and viral load were associated with OPC which is in agreement with previous studies reporting a significant association between CD4 and incident of OPC,7,34–36 high viral loads, and increased frequency of OPC among PLHIV.11,37–39 The CD4 cell count is inversely proportional to oral Candida counts and this predisposes PLHIV with low CD4 to eventually develop OPC. 40 Highly active ARV therapy may improve immunity through immune reconstitution leading to elevation of CD4 cells and reduced viral load.1,41 In addition, HAART inhibits secretory aspartyl proteinase enzymes needed for the growth of Candida species, thus reducing OPC incidences.42,43
In regards to the distribution of Candida species, 35 Candida isolates were obtained from 29 PLHIV with OPC, C. albicans was the most frequent aetiology of OPC as compared to NAC. In addition, C. tropicalis, and C. glabrata were the most common NAC species. The predominance of C. albicans may be related to its increased ability to switch from yeast to hyphal form, production of hydrolytic enzymes, biofilms and adhesion factors necessary for tissue invasion. 36 and shift towards NAC species among PLHIV may be due to substantial immunosuppression promoting the growth of NAC species.36,44,45 Our finding was consistent with previous study conducted in Ethiopia 46 and lower than what was determined in Cameroon by Miguel et al., 47 in South Africa by Owotade and Patel 48 and in Ghana by Kwamin et al. 24 However, Enwuru 49 and Anbesa et al. 50 reported low prevalence of C. albicans 49 as compared to our study. In addition, Agwu et al., 5 Taverne-Ghadwal et al., 25 and Berberi et al. 51 reported higher C. albicans and low NAC isolates in South western Uganda, Chad and Lebanon respectively underlining the shifting trend of OPC and oropharyngeal Candida towards NAC species. The contradictions in the distribution of Candida species could be due to the differences in the studied population in terms of geographical locations, demographics, clinical characteristics, immunological status, use of ART and antifungal therapy.1,27 Additionally, variances in sampling, diagnostic methods, oral hygiene, lifestyle, use of dentures, smoking and co-morbidities of studied populations could have attributed to differences in diversity of Candida species.52,53 Furthermore, fluconazole being the first line antifungal drug of choice for prophylactic prevention and management of candidiasis among PLHIV in Uganda may have enhanced the selection pressure of resistant Candida species by shifting OPC to more intrinsically antifungal-resistant C. krusei and C. glabrata. 54
Of the 35 tested isolates, 27 (77.1%), 35 (100%), 33 (94.4%), 35 (100%), 34 (97.1%) and 33 (94.4%) were susceptible to fluconazole, voriconazole, caspofungin, micafungin, amphotericin B and flucytosine respectively. In addition, 7 (20%) and 1 (2.9%) of isolates were resistant to fluconazole and flucytocine respectively. While each of 1 (2.9%) of isolates were intermediate to fluconazole, amphotericin B and flucytosine, 2 (5.7%) of isolates were intermediate to caspofungin.
Generally, 91.2%, 100%, 97.8%, 100%, 98.9% and 97.8% were susceptible to fluconazole, voriconazole, caspofungin, micafungin, amphotericin B and flucytocine respectively.
About 20% of isolates were resistant to fluconazole. This finding is slightly similar to 24.6% reported in Ghana 27 but higher than 5.5% in Tanzania, 55 1% in Brazil, 56 12.2% and 11.8% reported in Ethiopia and Nigeria respectively.26,49,57 Besides fluconazole resistance, Candida susceptibility of 98.9% to amphotericin B, 97.8% to flucytosine, 97.8% to caspofungin and 100% to micafungin and voriconazole is in agreement with previous study done in Cameroon and South Africa. 47 In other studies, including a study by Khedri and colleagues reported 100% susceptibility to caspofungin and amphotericin B, 58 Seyoum et al. 54 reported 99.4% of Candida isolates being susceptible to voriconazole. However, Moges et al. 59 reported lower susceptibility to voriconazole in their study. The possible reasons for the difference in resistance prevalence could be due to differences in previous drug usage, regional variations, diagnostic methods, immune status and intrinsic resistance of Candida species. 27 For instance, frequent use of fluconazole has been linked to overexpression of drug efflux pumps and consequently to development of fluconazole resistance.26,55 In Ugandan clinical guidelines, fluconazole is considered as antifungal of choice for the prophylactic prevention and treatment of fungal infections in PLHIV and it is frequently administered to this cohort of patients. 60 This may be the reasons behind 50% C. krusei, 50% C. glabrata and 20% C. albicans resistance to fluconazole. In addition, this could be due to increased selection pressure of resistant Candida species shifting to more intrinsically antifungal resistant C. krusei and C. glabrata 54 as a result of over dependence on fluconazole for prophylactic prevention and management of candidiasis among PLHIV in Uganda. 60 Low resistance in caspofungin, amphotericin B and flucytosine may be due to increased cost, limited access and non-consideration of these drugs as an option for treatment of OPC in most HIV/AIDS treatment clinics in Uganda and thus its reduced selection pressure and resistance. 60
Limitations of the study
The AFS testing was performed using the Vitek® compact system. This system has known limitations including under estimation of AFR. Considering alternative methods such as the CLSI broth microdilution method alongside the Vitek 2 AFS results would strengthen the study.
Conclusion
The prevalence of OPC among PLHIV was low, and there was a significant association between OPC and CD4 T cell count as well as viral load. C. albicans was the most frequently isolated oropharyngeal Candida species. C. glabrata and C. krusei exhibited the highest AFR among the NAC species. Fluconazole demonstrated the highest resistance among antifungal drugs.
Footnotes
Acknowledgements
We acknowledge TASO Mulago and Mbarara clinical team for participating in the clinical evaluation of our study participants. We appreciate the microbiology laboratory team of Makerere University for analyzing samples. We are grateful to the government of Uganda through MakRIF for financing this study.
Declarations
Abbreviations
AIDS Acquired Immuno Deficiency Syndrome.
AFR Antifungal Resistance.
AFST Antifungal Sensitivity Test.
CLSI Clinical Laboratory Standards Institute.
HIV Human immunodeficiency virus.
NAC non albicans Candida species.
OPC Oropharyngeal candidiasis.
PLHIV People Living with Human Immunodeficiency Virus.
TASO The Aids Support Organization.