
Abstract
India has the highest number of global deaths of children under 5 years of age. In the year 2015, it was reported that there were 5.9 million deaths of children under 5 years of age globally, of which 1.2 million (20%) occurred in India alone. Currently, India has an under 5 mortality rate of 48 per 1000 live births. Community-acquired pneumonia contributes to about one sixth of this mortality. Fast breathing is the key symptom of community-acquired pneumonia. The World Health Organization recently categorized community-acquired pneumonia in children under 5 years of age into two, pneumonia, and severe pneumonia. Fast breathing with or without chest in-drawing is categorized as pneumonia and fast breathing with any of danger signs as severe pneumonia. Because effective vaccines against two of the common organisms causing community-acquired pneumonia, namely Streptococcus pneumoniae and Haemophilus influenzae type b, are available, there should be urgent and phased introduction into the Indian Universal Immunization Programme. Several preventable risk factors of community-acquired pneumonia such as lack of exclusive breast feeding for first 6 months of life, inappropriate complimentary feeding, iron deficiency anemia, malnutrition, and indoor air pollution should be adequately addressed. The community should be aware about the signs and symptoms of community-acquired pneumonia and its danger signs so that delay in qualified care seeking can be avoided. To achieve the sustainable development goal of ⩽25 under five deaths per 1000 live births by 2030, a multipronged approach is the need of the hour.
Introduction
In the year 2015, it was reported that there were 5.9 million deaths of children under 5 years of age globally, of which 1.2 million (20%) occurred in India alone [Lancet Report, 2015]. Currently, India has an under 5 mortality rate of 48 per 1000 live births [World Bank, 2015]. Community-acquired pneumonia (CAP) contributes to about one sixth of this mortality [United Nations Children’s Emergency Fund (UNICEF) and World Health Organization (WHO), 2006].
CAP is an infective inflammation of lung parenchyma due to bacterial or viral pathogens. The key symptom of CAP is fast breathing. WHO [1994] has defined fast breathing as respiratory rate of >60 per minute for infants less than 2 months, >50 per minute for infants of 2–12 months, and >40 per minute for children more than 12–59 months. Previously, CAP was categorized into three groups by WHO namely pneumonia, severe pneumonia, and very severe disease. Fast breathing alone was categorized as pneumonia, fast breathing with chest in-drawing as severe pneumonia, and fast breathing with chest in-drawing along with any of the danger signs, namely inability to feed, drowsiness or altered consciousness, convulsion, cyanosis, as very severe disease. Recently, however, WHO [2014] categorized CAP in children under 5 years of age into two: pneumonia and severe pneumonia. Fast breathing with or without chest in-drawing is now categorized as pneumonia and fast breathing with any of the danger signs as severe pneumonia.
The rationale of the present review is to assess the current status of management and prevention of CAP with the aim to identify knowledge gaps and implementation inefficiencies. This can help to reduce mortality due to CAP and to achieve the Sustainable Development Goal (SDG) of ⩽25 deaths of children under 5 years of age per 1000 live births by the year 2030 [UNO, 2015].
Methodology
Study design
We adopted the standard methodology of conducting systematic reviews [Mathew et al. 2011]. Secondary data analysis (meta-analysis) was not done. The primary research question was ‘what was the current status of pneumonia management and prevention in India’ and secondary research questions were ‘to assess the burden of pneumonia in children in India’ and ‘to describe the etiology of pneumonia in children in India’.
Inclusion criteria
Types of publications
In this review, articles published in the English language between April 1985 and March 2015 were screened. The lower cut-off year of 1985 was used because WHO launched its acute respiratory infection (ARI) program in this year. All type of study designs, including randomized controlled trials, case control, cohort, and other descriptive studies, were included. Two reviewers, K.K.Y. and S.A., did the search and critically appraised the papers independently for their suitability for inclusion. Disputes were resolved by consensus.
Types of participants
Publications were included where children aged 2–59 months were studied, either alone or as one of the groups.
Outcome variables
The outcome variables included CAP-associated mortality, incidence, etiology, risk factors, and its prevention.
Exclusion criteria
Studies were excluded if pneumonia in the specified age group was either ventilation associated, or hospital acquired or due to immune-compromised status of the host.
Literature search
Two primary databases, PubMed (http://www.pubmed.com) and Google Scholar (https://scholar.google.co.in/) were searched. Additional sites searched were WHO reports (http://www.who.int), documents of the UNICEF (http://www.unicef.org/india/), National Family Health Survey (http://www.nfhsindia.org/), and Ministry of Health and Family Welfare, Government of India (http://www.mohfw.nic.in).
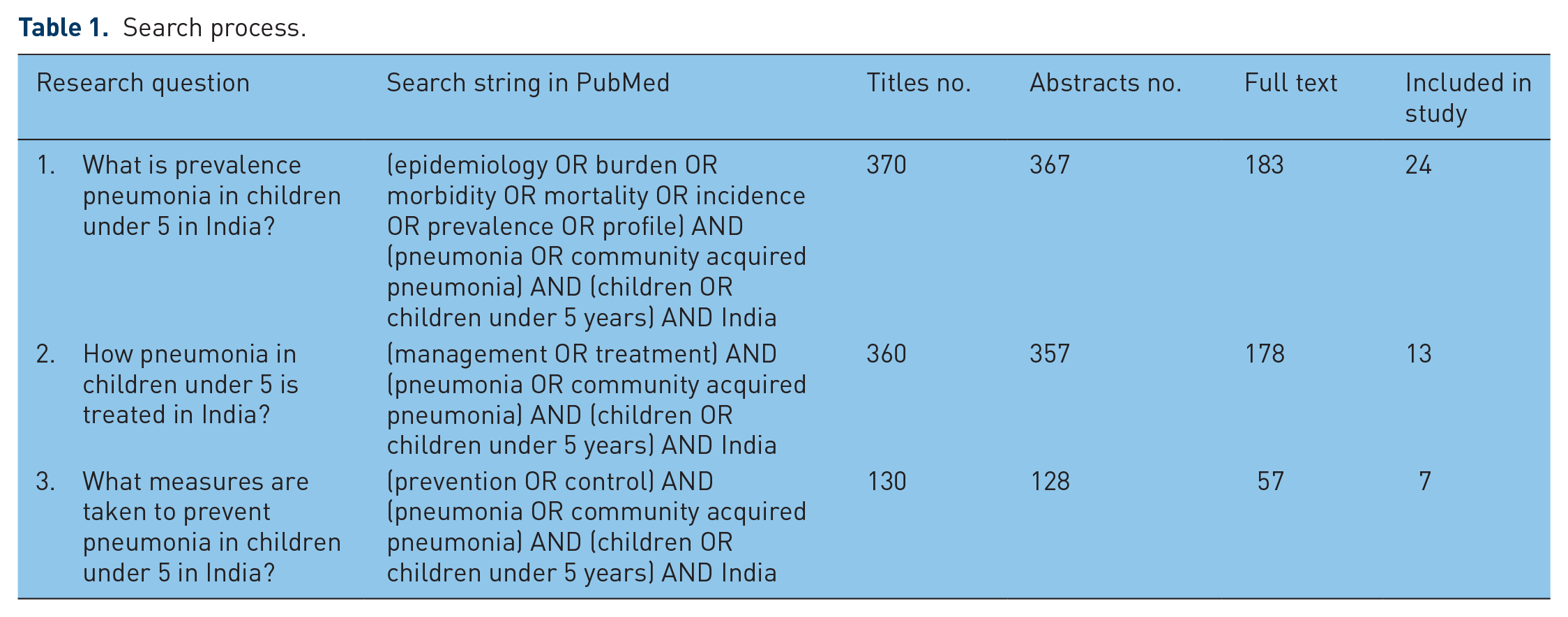
For PubMed the search strings were (1) (epidemiology OR burden OR morbidity OR mortality OR incidence OR prevalence OR profile) AND (pneumonia OR community acquired pneumonia) AND (children OR children under 5 years) AND India (2) (management OR treatment) AND (pneumonia OR community acquired pneumonia) AND (children OR children under 5 years) AND India (3) (prevention OR control) AND (pneumonia OR community acquired pneumonia) AND (children OR children under 5 years) AND India were done (Table 1).
Search process.
Burden of CAP
CAP is one of the major causes of morbidity and mortality in children under 5 years of age [UNICEF and WHO, 2006]. Incidence of CAP in children under 5 years of age was 0.27 [95% confidence interval (CI): 0.14–0.63] episodes per child-year in African region, followed by 0.26 (95% CI: 0.13–0.61) in South East Asian region, 0.23 (95% CI: 0.11–0.53) in Eastern Mediterranean region, 0.11 (95% CI: 0.05–0.24) in Western Pacific region, 0.08 (95% CI: 0.04–0.18) in American region, and 0.03 (95% CI: 0.02–0.04) in European region [Walker et al. 2013]. Annual deaths due to CAP in the same age group was 0.54 million in African region, 0.44 million in South East Asian region, 0.17 million in Eastern Mediterranean region, 0.024 million in American region and 0.018 million in European region [Walker et al. 2013].
In India, annually, 0.35–0.37 million deaths in children under 5 years of age have been reported due to CAP [Bassani et al. 2010; Farooqui et al. 2015], which accounted for 13–16% of total annual mortality in this age group [Smith, 2000; Selvaraj et al. 2014; Bassani et al. 2010]. Other Indian studies reported 3.6–4.0 million episodes of CAP in children under 5 years of age in the year 2010 [Farooqui et al. 2015] with 30.7–32.0 episodes per 1000 child-year of severe pneumonia [Rudan et al. 2013]. Among the Indian states, Uttar Pradesh has the maximum number of CAP cases and deaths (24% cases, 26% deaths) in children under 5 years of age followed by Bihar (16% cases, 22% deaths), Madhya Pradesh (9% cases, 12% deaths) and Rajasthan (8% cases, 11% deaths) [Farooqui et al. 2015]. The case fatality rate (CFR) due to CAP in children under 5 years of age ranged from 2.5% to 11.8% [Ramachandran et al. 2012; Sehgal et al. 1997; Tiewsoh et al. 2009; Agrawal et al. 1995; Rai et al. 2008]. Younger children had greater CFR. Correspondingly, the incidence of severe pneumonia requiring hospitalization gradually decreased with increasing age [Gupta et al. 2010; Ramachandran et al. 2012; Sehgal et al. 1997]. Also, CFR was higher in girls than boys [Bassani et al. 2010; Reddaiah and Kapoor, 1990]. With introduction of vaccines against Haemophilus influenzae and Streptococcus pneumoniae across India shortly, the incidence of CAP and CFR associated with it is likely to change. Hence, there is a need for establishment of a community- and hospital-based surveillance system to capture the change.
Clinical features
Children with pneumonia usually present with fever along with fast breathing with or without cough. They may also have chest retractions and any or more of WHO danger signs, including irritability or lethargy, inability to feed, cyanosis, convulsion, and respiratory failure.
Irrespective of the underlying etiology, signs of fast breathing and lower chest in-drawing are highly sensitive and reasonable specific for diagnosing CAP [Shann et al. 1984; Palafox et al. 2000; Singhi et al. 1994]. Fast breathing had reported sensitivity of 64–81%, specificity of 54–70%, while lower chest in-drawing had sensitivity of 17–35% and specificity of 82–84% [Mulholland et al.1992]. In several studies, fast breathing was reported as a better predictor of pneumonia compared with auscultatory findings [Campbell et al. 1988; Mulholland et al. 1992; Red et al. 1994].
Wheezing is more likely to be present when the probable etiology of CAP is viral rather than bacterial. However, in a study conducted in Pakistan in the year 1987 [Ghafoor et al. 1990], wheezing was reported in 36% and 44% children admitted with severe CAP with bacteremia due to S. pneumoniae and H. influenzae, respectively. Various other studies have reported that almost 1/3 to 2/3 of cases of nonsevere pneumonia had auscultatory wheeze [Gowraiah et al. 2014; Shah and Gupta, 2010; Hazir et al. 2004]. Likewise, wheezing was reported in approximately 26.8% cases of severe pneumonia from Pakistan [Hazir et al. 2004]. Classical findings of crepitations were reported only in 26–30% of WHO-defined pneumonia [Falade et al. 1995].
Pneumonia due to Mycoplasma or Chlamydia generally present subacute onset of headache, malaise, nonproductive cough, low grade fever, and rhonchi. CAP can also present with local complications like parapneumonic or synpneumonic effusion; empyema; lung abscess or remote complications like meningitis, pyopericardium, septicemia, septic ileus or diarrhea; and osteomyelitis.
Burden of CAP children under 5 years of age in India.
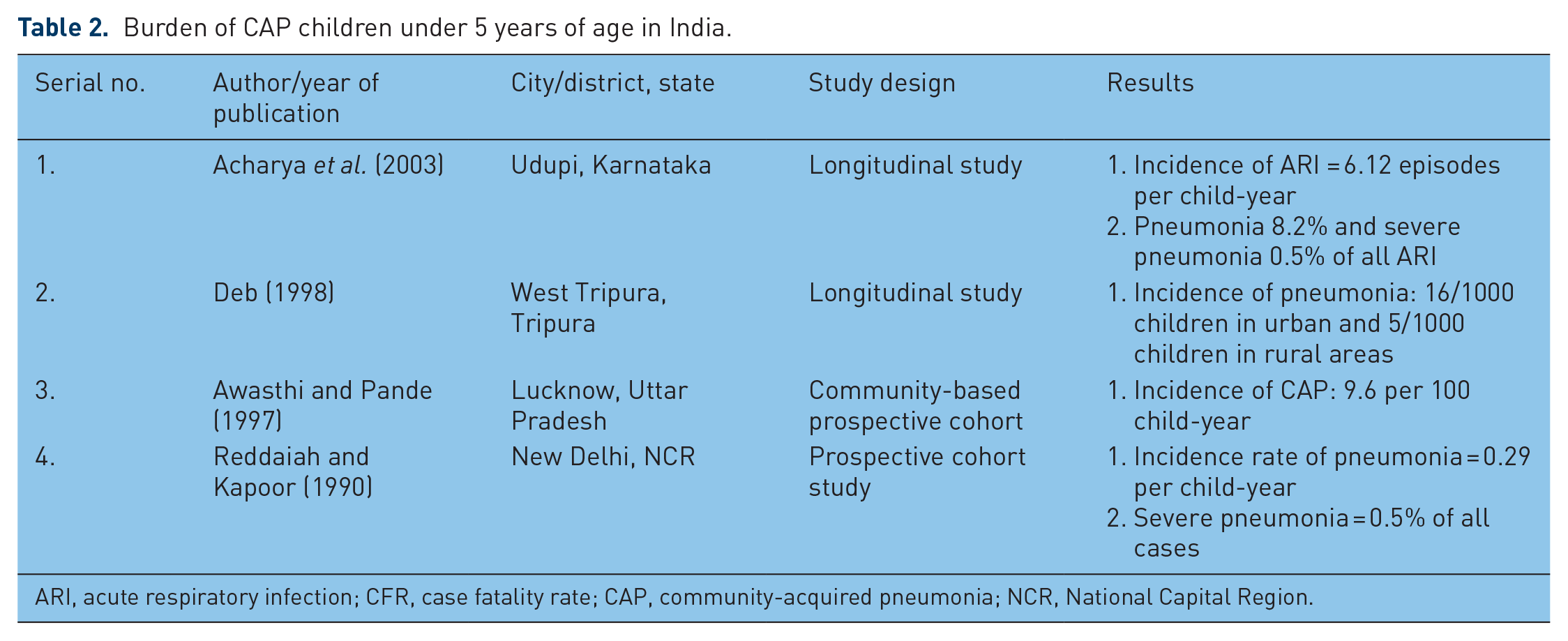
ARI, acute respiratory infection; CFR, case fatality rate; CAP, community-acquired pneumonia; NCR, National Capital Region.
Diagnosis
Diagnosis of CAP is largely clinical. Peripheral blood smear usually showed leucocytosis with neutrophilic predominance. Among the commonly studied biomarkers, levels of acute phase reactants, C-reactive protein (CRP) and procalcitonin (PCT) were found to be increased [Don et al. 2005; Yadav et al. 2015]. PCT was found to be a better predictor of severity of CAP in children than CRP [Yadav et al. 2015]. X-ray of the chest is not routinely required for diagnosing CAP but needed when there is a doubt in the diagnosis, persisting symptoms, suspicion of complications like pleural effusion, pneumothorax, and so on [Harris et al. 2011]. To decrease intra- and interobserver variation, WHO [2001] classified X-ray chest findings found in CAP into non-end point infiltrates, end point consolidation, and pleural effusion. In various studies [Harris et al. 2011; Kabra et al. 2004; Swinger and Zwarenstein, 2000], X-ray chest performed poorly in differentiating viral from bacterial pneumonia. However, according to the WHO [2001] radiological findings of end point consolidation and pleural effusion were likely to be bacterial etiology, mainly S. pneumoniae.
Identification of possible etiological organism of CAP can be done by blood culture. Reported yield of blood culture ranged between 2% and 27% in Indian studies (Table 3) [Mathew et al. 2015; Bahl et al. 1995; Tiewsoh et al. 2009; Kabra et al. 2003; Capoor et al. 2006]. Lung puncture aspirate (LPA) gives a greater yield and can be specific. But LPA is an invasive procedure and associated with serious side effects, including pneumothorax and pulmonary hemorrhage. Hence, it is rarely performed in CAP.
Isolation of bacteria in children under 5 years of age with CAP in India.

ALRTI, acute lower respiratory tract infection; CAP, community-acquired pneumonia; CSF, cerebrospinal fluid; IPD, invasive pneumococcal disease; NCR, National Capital Region; NPA, nasopharyngeal aspirates; PCR, polymerase chain reaction; RSV, respiratory syncytial virus.
Not restricted to children under five.
A relatively newer method of blood culture namely Bact T/ALERT 3D system gave nearly four times higher yield than conventional blood culture [Capoor et al. 2006]. Because of low yield and long reporting time, traditional blood culture is not very useful as a diagnostic tool. Therefore, researchers have used nasopharyngeal aspirate (NPA) to assess possible etiology. However, the NPA reflects the organism present in nasopharynx and does not necessarily reflect the causative organism of CAP [Chaudhary et al. 1998; Pandey et al. 2000; Maitreyi et al. 2000]. Immune assays of serum for presence of specific antibodies have also been used, mainly for diagnosing Mycoplasma and Chlamydia infections, as these organisms require live tissue culture media. However, the antibodies against these organisms appeared 2–3 weeks after primary infection and persisted for up to 2–6 months, complicating the interpretation of seropositivity [Kuo et al. 1995]. Urine assays for antigens of specific bacteria like S. pneumoniae and H. influenzae have been also used but have not gained wide acceptability as there was kit-to-kit variation on detection rates.
Polymerase chain reaction (PCR) is a rapid and sensitive method for detection of bacteria, including atypical ones and viruses causing CAP, but it requires high start-up cost of equipment as well as trained personnel. Multiplex PCR platforms have been developed that can identify viral and bacterial etiology using whole blood or NPA samples [Picot et al. 2014; Levine et al. 2012]. Also, serotyping of certain bacteria has been attempted by PCR method [Picot et al. 2014].
Etiology
From cases of WHO defined CAP in children bacteria, viruses, and atypical bacteria have been isolated in different studies (Tables 3–5). The rate of isolation of organism was different in various studies and age groups. Unlike the developed countries where viruses were responsible for most cases of pneumonia in children between 2 months and 5 years, bacterial infections contributed maximum number of cases in developing countries [Berman, 1991].
Isolation of virus in children under 5 years of age with CAP in India.
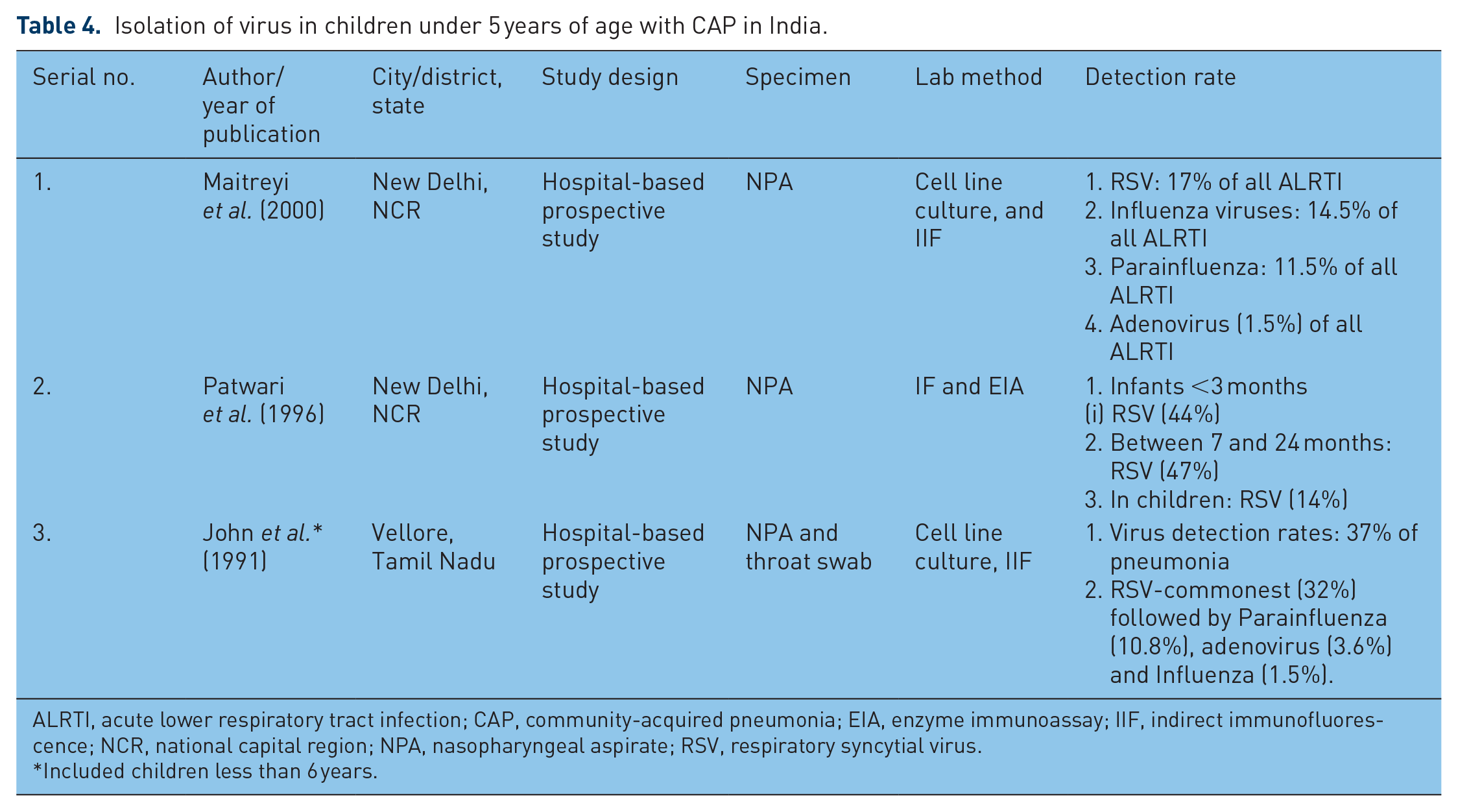
ALRTI, acute lower respiratory tract infection; CAP, community-acquired pneumonia; EIA, enzyme immunoassay; IIF, indirect immunofluorescence; NCR, national capital region; NPA, nasopharyngeal aspirate; RSV, respiratory syncytial virus.
Included children less than 6 years.
Detection of atypical bacteria in children under 5 years of age with CAP in India.

ALRTI, acute lower respiratory tract infection; EIA, enzyme immune assay; IF, mmunofluorescence; IIF, indirect immunofluorescence; MAT, microparticle agglutination test; MIF, microimmunofluorescence.
Several studies showed that S. pneumoniae was most common organism (30–50%) [Capoor et al. 2006; Farooqui et al. 2015; Rudan et al. 2013; Mathew et al. 2015; Tiewsoh et al. 2009; Awasthi and Pande, 1997; Pandey et al. 2000; Bahl et al.1995] followed by H. influenzae type b in 8.8% [Capoor et al. 2006] and Staphylococcus aureus 7–23% [Capoor et al. 2006; Tiewsoh et al. 2009; Pandey et al. 2000]. In Indian children, different serotypes of S. pneumoniae were isolated with serotypes 1 and 5 being most prevalent followed by 4, 6A and 6B, 7, 12, 14, 15, 19F, 23, and 45 [Nisarga et al. 2015; Balaji et al. 2015; John et al. 1996; Kurien et al. 1999; Kanungo and Rajalakshmi, 2001].
Other organisms had also been isolated like Acinetobacter in 20% [Capoor et al. 2006] and Klebsiella pneumoniae in 3.3–20.5% [Capoor et al. 2006; Tiewsoh et al. 2009; Mathew et al. 2015]. In the Severe Pneumonia Evaluation Antimicrobial Research (SPEAR) study [Rai et al. 2008] and the CAPES study [Nisarga et al. 2015], S. aureus was the commonest organism isolated from severe cases of pneumonia in children under 5 years of age.
There is a relative dearth of studies on viral etiology of CAP. This may be because viral isolation is difficult as compared with bacterial isolation, resulting in an underestimation of viral contribution to CAP [Weber et al. 1998]. Table 4 shows that studies have reported variable proportions (37–44.5%) of viruses isolated from cases of CAP [Maitreyi et al. 2000; John et al. 1996]. The most common virus isolated was respiratory syncytial virus (RSV) (17–32%) followed by influenza virus (1.5–14.5%), parainfluenza virus (10.8–11.5%), and adenovirus (1.5–3.6%) [Maitreyi et al. 2000; John et al. 1996].
Atypical bacteria were reported as an important cause of CAP in children under 5 years of age against previous conception that they were mainly responsible for the disease in older children. Chlamydia pneumoniae contributed to 1–20% [Jain et al. 2007; Mathew et al. 2015; Kabra et al. 2003; Chaudhary et al. 1998; Pandey et al. 2000, 2005] and Mycoplasma pneumoniae to 4–30% [Mathew et al. 2015; Kabra et al. 2003; Chaudhary et al. 1998; Pandey et al. 2000] cases of CAP in children under 5 years of age (Table 5).
It has to be noted that most of the studies were hospital based and therefore included severe cases only. There are limited studies that have done concomitant investigation for bacterial and viral etiology of CAP and their clinical correlates; hence, more work is needed.
Antimicrobial resistance pattern in India
Cotrimoxazole and amoxicillin are the two antibiotics that are commonly recommended in the case management of CAP. Variable levels of resistance against these antibiotics have been reported in S. pneumoniae and H. influenzae type b (Table 6).
Antimicrobial resistance pattern in Streptococcus pneumoniae and Haemophilus influenzae in India.
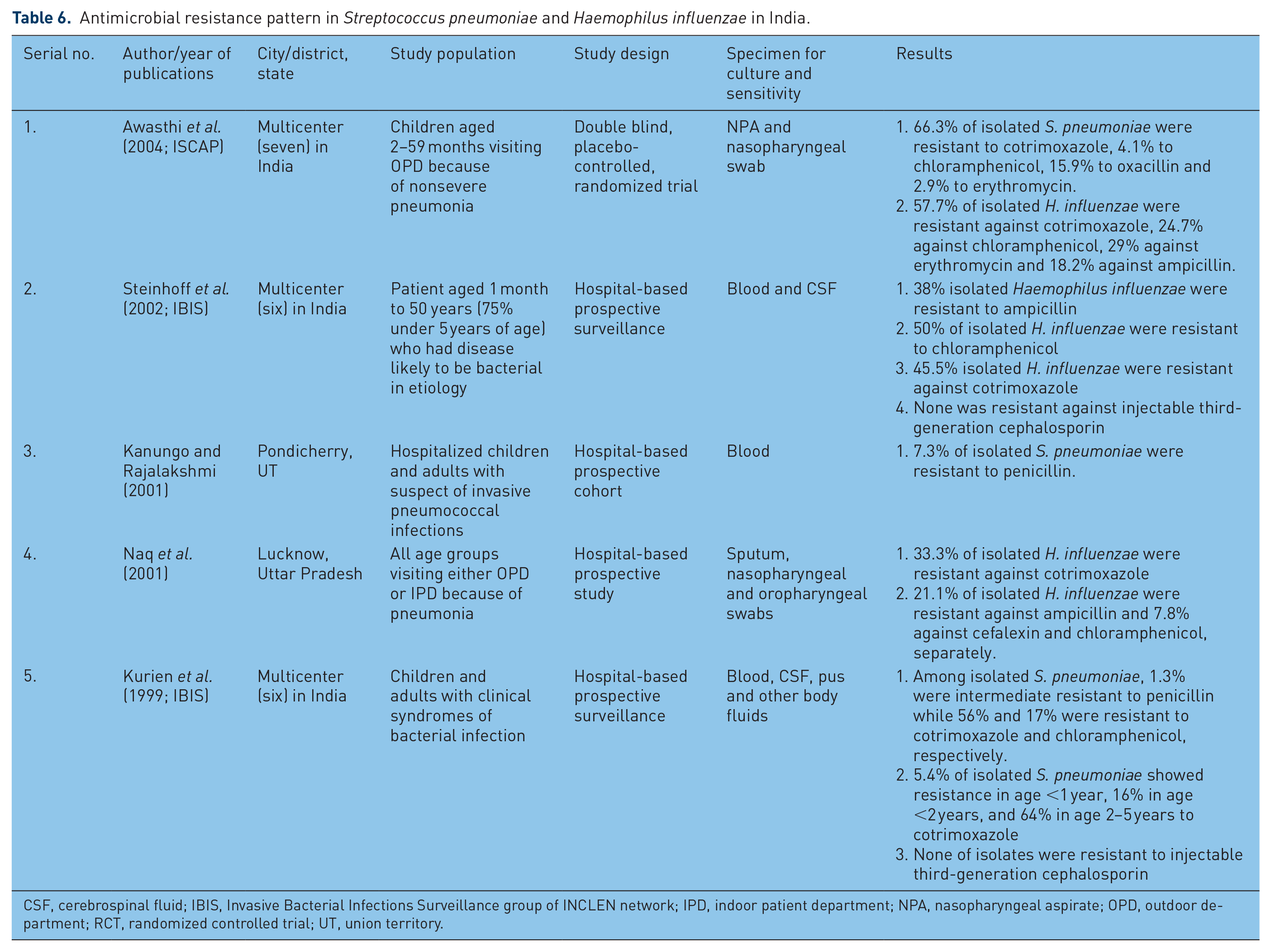
CSF, cerebrospinal fluid; IBIS, Invasive Bacterial Infections Surveillance group of INCLEN network; IPD, indoor patient department; NPA, nasopharyngeal aspirate; OPD, outdoor department; RCT, randomized controlled trial; UT, union territory.
In the Invasive Bacterial Infection Surveillance (IBIS) study [Kurien et al. 1999], only 5.4% of isolated S. pneumoniae were resistant to cotrimoxazole in age group <1 year that increased to 16% in age group <2 years and 64% in age group 2–5 years. Similar findings of increasing resistance to cotrimoxazole with increasing age among isolated S. pneumoniae were also reported by other Indian studies [Jebaraj et al. 1999; Coles et al. 2002]. Similarly, 66.3% of isolated S. pneumoniae from NPA of children under 5 years of age visiting ambulatory health care with WHO-defined nonsevere pneumonia were resistant to cotrimoxazole [Intensive Statin Therapy for Chinese Patients with Coronary Artery Disease Undergoing Percutaneous Coronary Intervention (ISCAP) study, Awasthi et al. 2004]. Not only India but also Bangladesh has reported a high prevalence (64.1%) of resistance in isolated S. pneumoniae to cotrimoxazole [Saha et al. 1999]. Resistance against penicillin was reportedly low in all age groups and none of the isolates were resistant to injectable third-generation cephalosporin [Kanungo and Rajalakshmi, 2001; Jebaraj et al. 1999; Kurien et al. 1999]. Therefore, WHO [2014] has recommended the use of amoxicillin for management of CAP in children under 5 years of age.
Like S. pneumoniae, there is increasing resistance in H. influenzae against commonly used antibiotics in India. In the IBIS study [Steinhoff et al. 2002], 50% of isolated H. influenzae were resistant to chloramphenicol, 38% to ampicillin, and 45.5% to cotrimoxazole, while none were resistant to third-generation injectable cephalosporin. The ISCAP study [Awasthi et al. 2004] reported that 57.6% of NPA isolates of H. influenzae were resistant to cotrimoxazole and 24.7% to chloramphenicol.
Management
Early diagnosis and appropriate use of antibiotics are the best strategies to reduce CAP-related mortality in children. Non-severe pneumonia can be managed at home with oral antibiotics, but monitoring, timely and appropriate referral and follow-up are crucial. Both oral cotrimoxazole and amoxicillin were used extensively in home-based treatment of CAP. There is growing evidence of development of in vitro resistance in S. pneumoniae and H. influenzae against cotrimoxazole in Indian children [Kurien et al. 1999; Awasthi et al. 2004; Steinhoff et al. 2002; Saha et al. 1999]. Therefore, oral amoxicillin is the next alternative choice of antibiotic for treatment of CAP. A randomized trial study [Rajesh and Singhal, 2013] on children under 5 years of age reported higher treatment failure in oral cotrimoxazole group (39.1%) than oral amoxicillin group (8.1%). A systematic review done earlier [Kabra et al. 2006] also reported better efficacy of amoxicillin over cotrimoxazole in management of CAP. The British Thoracic Society [Harris et al. 2011] and Indian Academy of Pediatrics [Agarwal et al. 2007] recommended oral amoxicillin as the antibiotic of first choice for nonsevere pneumonia. Now, the WHO [2014] also recommends domiciliary treatment with oral amoxicillin (40 mg/kg/dose) two times in a day for 3 days for pneumonia without chest in-drawing and 5 days for pneumonia with chest in-drawing. A study [Awasthi et al. 2004] clearly showed that 3 days of oral amoxicillin was equally effective as 5 days treatment in cases of nonsevere pneumonia. If there is no improvement in 48 h, amoxicillin should be replaced with co-amoxiclav [Dekate et al. 2011].
In hospitalized children with severe CAP, injectable chloramphenicol was found to be inferior to injectable ampicillin plus gentamicin [Rai et al. 2008; Kabra et al. 2006]. Injectable ampicillin plus gentamicin is now first choice for hospital-based treatment of severe CAP [WHO, 2014]. In absence of satisfactory improvement in next 48 h, antibiotics should be changed to ceftriaxone [WHO, 2014]. Addition of cloxacillin is recommended, if features of S. aureus infection like boils in skin or abscesses anywhere in the body, rapidly progressive or deteriorating pneumonia, post measles pneumonia, and complications like empyema, pneumatoceles, and pneumothorax are present [Dekate et al. 2011].
Apart from antibiotic therapy, children need supportive care, including oxygen therapy. Because clinical signs and symptoms have poor diagnostic accuracy for predicting hypoxemia [Lodha et al. 2004; Basnet et al. 2006], as far as possible, pulse oximetry should be use for early detection. Pulse oximetry has shown promising results in reduction of mortality due to CAP by early detection and therefore treatment of hypoxemia [Duke et al. 2009]. WHO [2005] recommends oxygen therapy where pulse oximetry is not feasible in very severe or severe pneumonia and SpO2 less than 90% at room air.
Risk factors and prevention
Preventable risk factors for CAP can be classified into nutritional, environmental and social and behavioral. Nutritional risk factors for CAP were lack of exclusive breast feeding for first 6 months of life [Tiewsoh et al. 2009; UNICEF and WHO, 2006], inappropriate timing and content of complimentary feeding [Bhat and Manjunath 2013; Shah et al. 1994], iron deficiency anemia [Hussain et al. 2014; Bhat and Manjunath 2013; Ramakrishnan and Harish, 2006] and malnutrition [Bhat and Manjunath 2013; Broor et al. 2001; Deb, 1998] (Table 7). The most important nutritional risk factor for CAP was lack of exclusive breast feeding for first 6 months of life. This can increase the risk of CAP up to 1.5–2.6 times [Acharya et al. 2003; Shah et al. 1994; Mihrshahi et al. 2008]. This can also translate into 30–42% increased incidence of respiratory infections in children in underdeveloped countries [Ladomenou et al. 2010]. Therefore, the WHO and UNICEF advocate exclusive breast feeding in first 6 months of life in their global action plan to prevent pneumonia (GAPP). Despite these, in India, only 46.4% children were exclusively breast fed for their first 6 months [NFHS III 2007].
Risk factors for mortality and morbidity of CAP in children under 5 years of age in India.

ALRTI, acute lower respiratory tract infection; ARI, acute respiratory infection; CAP, community-acquired pneumonia; LPG- liquid petroleum gas; RCT, randomized controlled trial; SES, socioeconomic status; URTI, upper respiratory tract infection.
Various studies [Hussain et al. 2014; Bhat and Manjunath 2013; Ramakrishnan and Harish, 2006] reported 5–7 times increased risk of CAP in children with anemia. Because in India, 69.5% of children are anemic [NFHS III 2007], the CAP-related mortality is high. Undernutrition is an independent risk factor for mortality in children under 5 years of age. In India, 42.5% of children are undernourished [NFHS III 2007]. Hence, effective strategies for prevention of anemia and malnutrition in children have to be implemented.
Among the environmental risk factors of CAP, indoor air pollution due to use of biomass fuel for cooking has been extensively studied. Ambient air pollution resulted in two- to fourfold increased risk of CAP [Bhat and Manjunath 2013 Broor et al. 2001; Mahalanabis et al. 2002]. Still in rural India, 61.7–65.4% of households use coal and wood as source of fuel for cooking [NFHS III 2007; DLHS III 2010]. Other important environmental risk factors are overcrowding [Tiewsoh et al. 2009; Shah et al. 1994], upper or lower respiratory infection in a family member [Broor et al. 2001 Bhat and Manjunath 2013], poor housing and indoor or parental smoking [Acharya et al. 2003] (Table 7). Despite statutory warning against tobacco, smoking by parents is prevalent in India.
Among the social and behavioral risk factors of CAP, hand washing is the most important, because this is simple and can reduce the incidence of CAP by 24% [Wiley Online Library, 2006]. At community level, there is delay in recognition of CAP as fast breathing is not commonly recognized by community and grass root health-care workers [Awasthi et al. 2015]. There is delay in qualified care seeking for CAP as the preferred health-care provider is the village-based unqualified doctor [Awasthi et al. 2015; May et al. 2014]. Home remedies and self-medication further delay care seeking [Awasthi et al. 2015; Kumar et al. 2008; Mohan et al. 2008]. There is a distrust in the public health system, and in most cases, children reach a government tertiary care center when they have been ill for a week or so and have been treated by two to three health-care providers [Awasthi et al. 2015; Srivastva et al. 2009; Deshmukh et al. 2009].
Prevention of CAP by immunization
Immunization is a major step to prevent CAP in children. In 1978, India introduced six childhood vaccines (BCG, TT, DPT, DT, Polio, and Typhoid) in its extended program of immunization (EPI). Measles vaccine was added much later, in 1985, when the Indian government launched the Universal Immunization Programme (UIP). A WHO review reports that a 31–46% relative reduction in childhood mortality can be brought about by more than 80% coverage of measles vaccine. In India, District Level Household and Facility Survey III (DLHS III) reported 69.1% coverage of measles vaccine in first 2 years of life. Vaccine against H. influenzae type b was not included in UIP; however, recently, a pentavalent vaccine (Pentavac by M/s Serum Institute of India) was introduced in Kerala and Tamil Nadu in year 2011 and later in the states of Goa, Pondicherry, Karnataka, Haryana, Jammu and Kashmir, Gujarat and Delhi. At present, this vaccine has been introduced in rest of the Indian states also.
Because the magnitude of invasive pneumococcal diseases in children in India is high, prevention through vaccination is desirable. In India, two types of pneumococcal vaccines are available. One is unconjugated pneumococcal polysaccharide vaccine 23 valent (PPSV23), which cannot be used before 2 years of age. For use in children less than 2 years, pneumococcal conjugate vaccines (PCV 10 and PCV 13) are available. PCV 10 covers 64% and PCV13 covers 73.3% of invasive pneumococcal strains [Manoharan et al. 2013]. Efforts are being made to include PCV into UIP. An Indian company with active support of Department of Biotechnology, Government of India, is developing 15-valent vaccine containing two additional serotypes, 2 and 12F to existing PCV 13.
Conclusion
CAP in children is a major contributor to mortality in children under 5 years of age. There is sufficient data to show that S. pneumoniae and H. influenzae contribute to >50% cases of CAP. Because effective vaccines against both of them are available, there should be urgent and phased introduction into the UIP. Several preventable risk factors of CAP like lack of exclusive breast feeding for the first 6 months of life, inappropriate complimentary feeding, iron deficiency anemia, malnutrition, and indoor air pollution should be adequately addressed. The community should be aware of the signs and symptoms of CAP and its danger signs so that delay in qualified care seeking can be avoided. To achieve the SDG, a multipronged approach is need of the hour.
Footnotes
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.