
Abstract
Background:
The prevalence of sexually transmitted infections (STIs) remains high worldwide. Despite the worldwide increase in the incidence of STIs every year, there are few reports on the frequency of STIs with different pathogens according to age and gender. Accordingly, a study was conducted to determine trends in co-infection with STIs by age and gender in Cheonan, South Korea from 2017 to 2021.
Objectives:
To identify trends by age or sex in co-infection of STIs in this region.
Design:
A retrospective study was conducted on clinical samples examined at Dankook University Hospital from January 2017 to November 2021. A total of 3297 specimens were collected from patients visiting Dankook University Hospital (Cheonan, Korea), and statistical analysis was performed on patients ranging in age from 1 day to 93 years.
Methods:
Multiplex polymerase chain reaction, the most efficient method to diagnose a bacterial infection, was performed using an MJ Research PTC-200 Thermal Cycler (Marshall Scientific, Richmond, VA, USA) and a Seeplex STD Detection Kit (Seegene, Seoul, Republic of Korea). The co-infection rate with STI pathogens was analyzed according to age and sex.
Results:
Of the 3297 clinical samples, 1017 (30.9%) tested positive for sexually transmitted pathogens, ranging from one to six co-infections. Analysis of the co-infection rate by age revealed that the average age gradually decreased as the total number of co-infection pathogens increased. The co-infection percentage and age distribution of STIs differed according to sex. Co-infection was more prevalent in female patients. Furthermore, co-infection in male patients occurred frequently in the 30–39-year-old group, while those in female patients occurred in the 20–29- and 30–39-year-old groups.
Conclusion:
Our statistical analysis showed that STI co-infections were more common among younger than older people. Therefore, it helps in recognizing STIs at a young age and provides possible indicator data to prevent STIs at a young age. In addition, further research is needed on co-infection in other regions.
Keywords
Introduction
Sexually transmitted infections (STIs) affect more than a million people daily worldwide. 1 In general, the pathogens causing STIs are spread through sexual contact, especially through oral, vaginal, or anal sex.2,3 STIs can be caused by a variety of pathogens [bacteria, including Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG), and Treponema pallidum; parasites such as trichomoniasis; fungi; and viruses such as human immunodeficiency virus, herpes simplex virus, and hepatitis B virus].4,5 Co-infection occurs when an individual is infected with two or more STIs concurrently, resulting in symptomatic or asymptomatic infection of the genital tract.5,6 If left untreated, STIs can cause severe health concerns and an increased risk of infertility and reproductive health complications. 6
Cultures or serological tests for specific pathogens are used in the diagnosis of STIs; however, these may be time-consuming and lack sensitivity for STI identification in asymptomatic patients.7,8 Additional difficulties include the culture technique, rate of co-infection with sexually transmitted diseases, and asymptomatic cases. Therefore, nucleic acid amplification-based tests are typically better suited for diagnosing sexually transmitted diseases. 4 Multiplex polymerase chain reaction (mPCR) is a sensitive way for detecting several types of pathogens simultaneously. It has also recently emerged as a popular method for molecular-based detection of sexually transmitted pathogens.4,8
Many outpatients with STIs are co-infected with multiple pathogens. Common causative agents of STIs are CT, Mycoplasma genitalium (MG), M. hominis (MH), NG, Trichomonas vaginalis (TV), and Ureaplasma urealyticum (UU).7,9 A study in Madrid, Spain, reported that TV plays an important part in the possibility of infection with genitourinary pathogens, such as NG and CT. 10 A Croatian study revealed an important relationship among CT and MG infection, and a further significant association between MG and MH infection was also reported. 11
As mentioned above, various co-infections occur and the number of STI patients is increasing worldwide. 12 Despite this global annual trend of the increasing incidence of STIs, there is little information about the prevalence of specific sexually transmitted infections by age and gender. Accordingly, we investigated trends in simultaneous STIs by age and gender in Cheonan, South Korea from 2017 to 2021. Therefore, in this study, mPCR-based STI screening was conducted from 2017 to 2021, and the number of patients in Korea who were co-infected with the pathogen of interest was stratified by age and sex.
Materials and methods
From January 2017 to November 2021, 3297 clinical samples were obtained from outpatients who went to the Dankook University Hospital for STI screening. Statistical analysis was performed on patients aged 1 day to 93 years.
Deoxyribonucleic acid extraction
Gathered clinical samples were kept at −70 °C until Deoxyribonucleic acid (DNA) isolation for mPCR. First, phosphate-buffered saline (PBS) was used to suspend each swab sample. Supernatant was removed after 10 min of centrifugation at 13,000g, and the pellet was then dissolved in PBS. A QIAamp DNA Mini Kit (QIAGEN, Hilden, Germany) was used to isolate DNA for mPCR analysis according to the manufacturer’s instructions. Thereafter, approximately 200 µL of each sample was used as the starting material for DNA isolation. A Thermo Fisher Scientific NanoDrop 1000 spectrophotometer was used to analyze the concentration of DNA extracted from each sample.
mPCR
mPCR for STIs was performed using an MJ Research PTC-200 Thermal Cycler (Marshall Scientific, Richmond, VA, USA) and a Seeplex STD Detection Kit (Seegene, Seoul, Republic of Korea), based on the manufacturers’ directions. First, 5 µL of the DNA extract were added to a polymerase chain reaction tube containing 5 µL of a premix and probe combination (Seeplex STD Detection Kit). Next, 10 µL of the mPCR premix were added to each of the six STI pathogens (CT, MG, MH, NG, TV, and UU). Primer combinations specific to each pathogen were used, and detection of all the pathogens was done in the same mPCR assay. The reaction conditions were as follows: 94°C for 15 min; 40 cycles of 94°C for 30 s, 63°C for 90 s, and 72°C for 90 s; and an extension step of 72 °C for 10 min for complete partial polymerization. In each cycle, standardized viral ribonucleic acid solutions and nuclease-free water were incorporated as positive and negative controls, respectively. The Arabidopsis cellulose synthase (CESA3) gene was included to be an inner switch for amplification. An inner control was added to the PCR combination in order to identify the occurrence of PCR inhibitors. Thereafter, PCR products were loaded onto a 2% agarose gel and electrophoretically separated after being stained with ethidium bromide. The separated PCR products were visualized under ultraviolet light.
Statistical analyses
For statistical processing, MedCalc ver. 11.6 (MedCalc Software, Mariakerke, Belgium) was used. DNA sequences from CT, MG, MH, NG, TV, and UU detected using real-time PCR were analyzed retrospectively based on the sex and age of the patients and causative pathogens of STIs. A p < 0.05 was considered statistically significant.
Results
A total of 3297 clinical samples were gathered for STI testing, and patients were screened for co-infection with these six different sexually transmitted pathogens (Table 1).
Number of specimens that tested positive for each type of sexually transmitted pathogen (N = 1017).

Of these, 1017 (30.9%) tested positive for sexually transmitted pathogens, ranging from one to six co-infections (Table 2).
Rates of co-infection with each sexually transmitted pathogen.

CT, Chlamydia trachomatis; MG, Mycoplasma genitalium; MH: Mycoplasma hominis; NG: Neisseria gonorrhoeae; TV, Trichomonas vaginalis; UU, Ureaplasma urealyticum; N/D, Not detected.
Highest percentage.
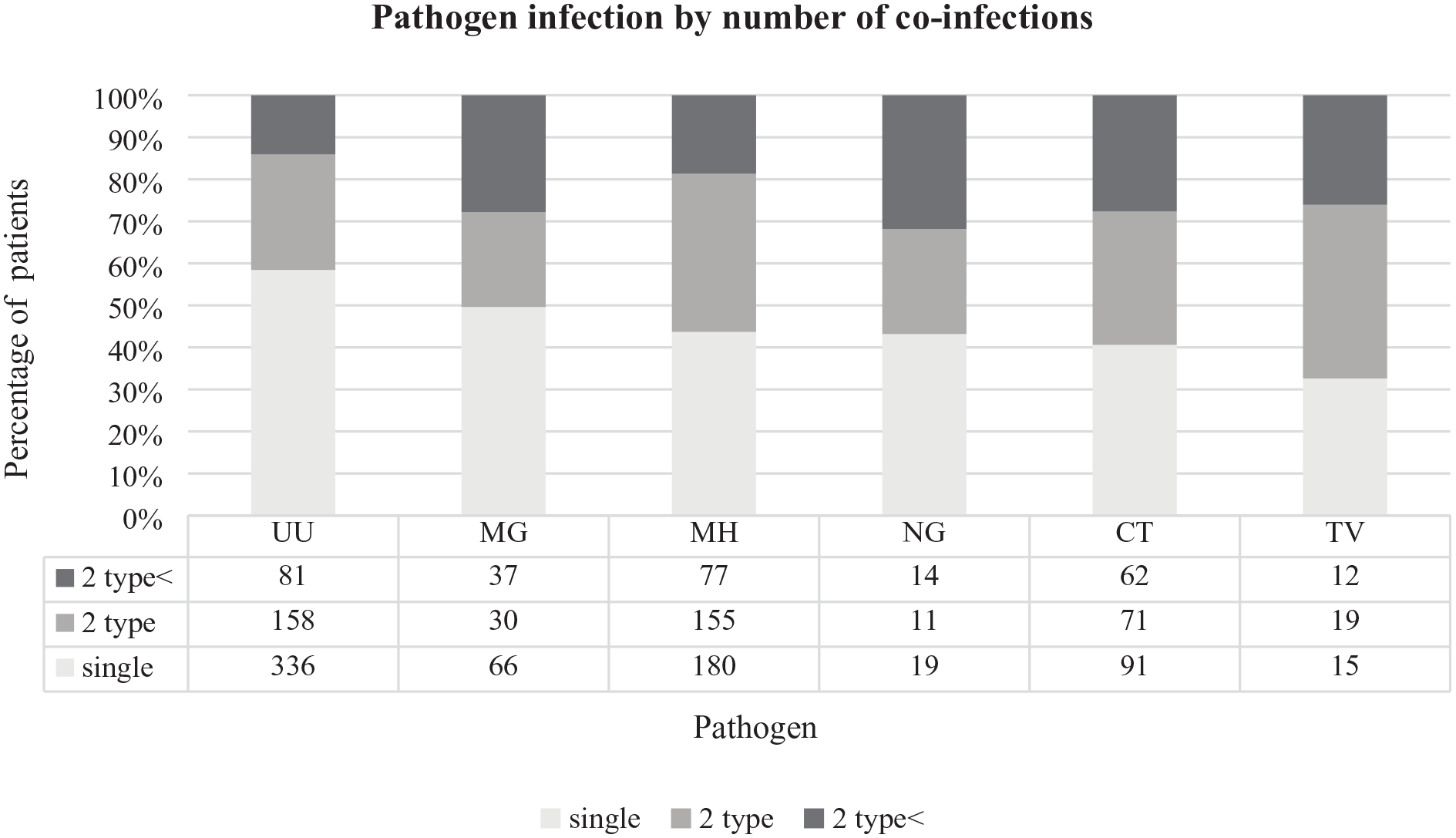
First, the co-infection rate of STI pathogens according to age was analyzed, and it was found that the average age gradually decreased as the number of co-infected pathogens increased. The mean age with the lowest number of co-infections (two co-infections) was 30 years, and that with the highest number of co-infections (five co-infections) was 22 years (Table 3). The occurrence of co-infections differed based on the pathogen type in this study. UU had a high single infection rate, although its rate of co-infection with two or more pathogens was lower, all other sexually transmitted pathogens considered. TV, on the other hand, displayed a low single infection rate and high co-infection rate. For all five pathogens except UU, the rate of co-infection with two or more types was greater than that of any one infection (Figure 1).
Mean age of patients with co-infections with multiple types of sexually transmitted pathogens according to the number of different pathogens detected.

N/D, Not detected.
Differences in sexually transmitted infections according to the pathogen.
Second, the co-infection rate and age distribution of STIs differed by sex as follows. Co-infection of male patients occurred frequently in the 30–39-year-old age group, while that of female patients occurred in the younger age groups of 20–29 and 30–39 years. Co-infection was common, mainly in female individuals (Figure 2). Male individuals averaged only two co-infections, whereas female individuals averaged up to five co-infections, depending on age.

Mean age according to sex and the number of co-infections.
Discussion
We investigated the rate of co-infections with six different STIs at a single hospital in the Republic of Korea. Our study revealed that the number of co-infections differed among pathogens. Moreover, most pathogens caused co-infection more frequently than single infection. Female patients tended to have more co-infections than male patients, and the likelihood of co-infection increased with decreasing age.
A study performed in Iran assessing co-infection with sexually transmitted pathogens via mPCR revealed that 10 of 300 (3.3%) outpatients had co-infections, with two, three, and five cases of CT/NG, CT/TV, and NG/TV co-infections, respectively. 8 Among patients with co-infections, those with UU infections had a low co-infection rate, and TV-infected patients had a high pathogen co-infection rate. A study conducted in Beijing, China, considered patients with co-infections. Among them, 60.6% of male patients and 71.4% of female patients were co-infected with UU and CT. 2 A study of hospitals visited by pregnant women in Ghana found co-infection (53%) to be common among women infected with TV. 13 In another study, about 30% of men who had sex with men (MSM) had co-infections. 1
Co-infection occurred mainly in female individuals, and the co-infection rate was high in the younger age group, with higher co-infection rates in younger age groups. In a study in New Mexico, USA, the highest rates of co-infection with MG, CT, and TV were discovered among female individuals aged 20–29 years. 14 A study conducted in China revealed a high rate of STIs in patients aged 20–39 years. 3 In another study in China, MSM were co-infected with more than two STIs. 1 In Reunion Island, common co-infection is CT, especially in female individuals under the age of 25 years. 15 In a study from Copenhagen, Denmark, 53.1% of co-infected patients were male patients and 46.9% were female patients. The co-infected female individuals were, on average, approximately 10 years younger than the co-infected male individuals. 16 In another study, nearly half of the STI cases occurred among participants aged 15–24 years. 17
This study had some limitations. First, it was conducted in only one region of the Republic of Korea, and additional research is needed in other regions and countries. Second, because it was a retrospective study, outcomes were not stratified based on patient’s clinical features.
Data on comorbidity of STIs at university hospitals were gathered and statistically evaluated by age and pathogen types. STIs were shown to be more common among younger adults. STIs that are left untreated can have detrimental effects, including mother-to-child transmission, birth abnormalities, and infertility. 18 Our statistical analysis showed that STI co-infections were more common among younger than older people. Accordingly, it may help to recognize STIs at a young age and provide preventable index data. Infected patients should be monitored for STIs and undergo regular examinations. 18 Some bacterial STIs or viral STDs can be treated with antibiotic therapy, antiviral drugs, or anticancer drugs. 18 To properly treat STIs, antibacterial agents must be taken at the correct dose and duration, and in this regard, additional research related to the treatment of STIs is needed. In addition, further research is needed on co-infection in other regions.