
Abstract
Background:
Treponema pallidum and HIV are among the most common public health problems in Ethiopia. These infections are interrelated. Treponema pallidum causes genital ulcer which enhances HIV transmission and complicates HIV by causing severe ulcer among HIV-positive individuals. Although Treponema pallidum and HIV have a similar route of transmission, screening services for Treponema pallidum are not available in most of the voluntary counseling and testing centers.
Objectives:
This study aimed to assess the seroprevalence of Treponema pallidum and sociodemographic factors among HIV-positive and HIV-negative individuals from the voluntary counseling and testing center of St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia.
Methods:
In this research, a cross-sectional study was conducted and a total of 292 consecutive samples were collected from the voluntary counseling and testing center of St. Paul’s Hospital Millennium Medical College. Data were collected using an interviewer-administered questionnaire. A blood specimen was tested for the presence of Treponema pallidum using rapid plasma reagin and a rapid test kit for HIV. The data were entered and analyzed using SPSS version 20.
Results:
The overall prevalence of Treponema pallidum was 5/292 (1.7%). All HIV-positive clients were negative for Treponema pallidum. None of the risk factors were significantly associated with Treponema pallidum.
Conclusion:
In this study, the prevalence of Treponema pallidum was 5/292 (1.7%). None of the study participants were co-infected with Treponema pallidum and HIV.
Recommendation:
There was a lack of association between syphilis and HIV in this study, but still the prevalence of Treponema pallidum among voluntary counseling and testing center clients is a public health problem. Therefore, Treponema pallidum infection control strategies should be designed in parallel with HIV control strategy and actions should be taken to avert the problem, including the provision of better health education and screening services at voluntary counseling and testing centers parallel with HIV.
Introduction
Sexually transmitted infections (STIs) are infections caused by microorganisms, which can be transmitted from one person to another through sexual intercourse. STIs represent major causes of morbidity, public health burden and socioeconomic cost in both developing and developed nations. 1
STIs are major public health problems in sub-Saharan countries, including Ethiopia. 2 Many people suffer from sexually transmitted diseases (STDs) due to lack of access to appropriate health care. 2 STIs are a major cause of acute illness, long-term disability and death, with severe medical and psychological consequences. 3
Most STIs share the common property of inducing inflammation and resulting in what is believed to be a risk for HIV acquisition. 4 Previous data indicated that, during the past decades, STIs enhance the transmission of HIV-1 infection. 5 Different age groups are affected by STIs; especially, adolescents are at higher risk of acquiring STIs, and adolescent girls, in particular, are disproportionately affected. 5
The challenge of dealing with STIs and their sequelae is an increasing concern for medical professionals and public health officials as they struggle to deal with the swelling pandemic. 6 STIs impose an enormous burden of morbidity and mortality in many developing countries, both directly through their impact on reproductive and child health and indirectly through their role in facilitating the sexual transmission of HIV infection. 7 HIV and Treponema pallidum represent a major public health problem in developing countries. These infections can be transmitted from the mother to the fetus and may cause severe morbidities in their offspring. 2 The information generated from this study was expected to help in designing control strategies on HIV/AIDS and T. pallidum at a voluntary counseling and testing (VCT) center in the study area. Syphilis is a systemic disease caused by T. pallidum, which can spread by sexual contact, blood transfusion and vertical transmission. 2 T. pallidum, an STI which seemed to have disappeared or had been controlled over the years, has re-emerged as a major public health problem in many rural, urban and suburban communities. 8 The increasing incidence of the disease is caused by sexual promiscuity, drug abuse, poverty, increased population migration and unemployment. Decreasing government support for public health in developing countries also aggravates this situation. 9
T. pallidum is a global problem, with 12 million people being infected every year. It is endemic in areas of Africa, Asia and Latin America where it was estimated that 11 million of the 12 million new adult cases of syphilis occur annually. 10 Studies conducted at Harar, Jijiga and Gondar among blood donors have shown that the prevalence of syphilis was 1.1%, 0.1% and 1.3%, respectively.11–13 Another study conducted from Gondar Family Guidance Association had shown that 1.9% of the pregnant women were positive for syphilis. 14
Syphilis clinical manifestations are classified into multiple stages as primary, secondary, latent (early and late) and tertiary syphilis. 9 Primary syphilis facilitates the transmission of HIV infection and it can contribute to the spread of HIV infection. 15 During the early part of the 20th century, tertiary syphilis was the cause of illness in about a fifth of patients in institutions for the mentally ill in the United States. 16
In primary syphilis, HIV-infected patients may present with two or more chancre and with larger and deeper lesions. Approximately one-fourth of HIV-infected patients present with concomitant lesions of both primary and secondary stages of syphilis at the time of diagnosis. 15
In Ethiopia, 21% of children of seropositive mothers develop signs of syphilis, while the stillbirth and abortion rate of infected women was almost double than that among the general population. 17
T. pallidum and HIV co-infection
T. pallidum and HIV are both sexually transmitted and a substantial number of people are infected with both agents. HIV has several effects on the presentation, diagnosis, disease progression and therapy of syphilis. Syphilis may increase the risk of HIV transmission by causing genital ulcers. 18 So, T. pallidum is an important infection in contemporary medicine because of the morbidity it causes and its ability to enhance the transmission of HIV. 19 In patients co-infected with HIV and T. pallidum, cutaneous lesions become more severe, symptomatic neuro-syphilis may be more likely to develop, the latency period before the development of meningo-vascular syphilis may be shorter and the efficacy of standard therapy for early syphilis may be reduced. 20 The rate of HIV and T. pallidum co-infection varies depending on the prevalence of both infections in the community or the patient group being studied, along with individual risk factors.
Furthermore, much higher rates of HIV co-infection were detected with the specific risk factors, for example, intravenous drug use (22.5%–70.6%) and gay sex (68%–90%). 21 The relative risk for HIV infection in patients with syphilis and other genital ulcer diseases (GUDs) ranges between 2 and 11, with the strongest evidence to date reported from studies conducted in Africa. 22 For example, one mathematical model has suggested that approximately 1000 additional cases of heterosexual HIV transmission occur annually in the United States as a result of syphilis. 18 In several developed countries, the prevalence of HIV among patients with syphilis has ranged from 15.7% to 43% and as high as 64%–90%.15,23 A study conducted among neuro-syphilis and ocular syphilis cases showed that 36% of the patients were HIV co-infected. 20 Ethiopia, like many African countries, is experiencing a severe HIV/AIDS epidemic and the prevalence of syphilis seroreactivity in Ethiopia was 20%–30% in men and 2%–27% in women measured in different regions of the country. 24
HIV
The 2016 Ethiopian Demographic and Health Survey (DHS) had shown that the prevalence of HIV among women and men aged 15–49 was 0.9% and HIV prevalence was higher among women than men (1.2% vs 0.6%). This survey had also shown that HIV prevalence was seven times higher in urban areas than in rural areas (2.9% vs 0.4%). HIV prevalence between regions ranges from less than 0.1% in Somali to 4.8% in Gambela. The HIV prevalence among young people was 0.3% among young women and 0.1% among young men aged 15–24. 25 A study conducted in northwest Ethiopia had shown that 9.6% of the pregnant women were positive for HIV-1. 26 In 2011, a study among pregnant mothers from rural hospitals in Southern Ethiopia showed that 1.8% of study individuals were positive for HIV. 1 Another study conducted at Gondar University Teaching Hospital had shown that the prevalence of HIV among blood donors was 3.8%. 12
The importance of this study was to determine the prevalence of T. pallidum among HIV-positive and HIV-negative individuals which is very important during therapeutic management. Furthermore, this study would clarify whether prevalence and associated factors of T. pallidum infection differ between HIV-infected and HIV-uninfected individuals. Consequently, in this study, we sought to provide some initial estimates regarding the rate of co-infection between HIV and T. pallidum to contribute additional information to the scientific community on serum status of syphilis among HIV-positive and HIV-negative individuals in the study area.
Methods and materials
Study area
This study was conducted at St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia. This institution provides health care service for approximately 100,000 patients per year to Addis Ababa and the surrounding population and those referred from different parts of the country. The hospital also provides VCT services.
Study design and period
A hospital-based cross-sectional study was conducted among clients who attended St. Paul’s Hospital Millennium Medical College VCT center during the study period from November to December, 2017.
Population
Source population
All voluntary participants who attended the VCT center of St. Paul’s Hospital Millennium Medical College during the study period were selected.
Study population
A total of 292 consecutive study participants were selected from the VCT center of St. Paul’s Hospital Millennium Medical College. All consecutive volunteers were recruited for HIV and T. pallidum testing. The study participants were between the ages of 18 and 75 years.
Selection criteria
Inclusion criteria
All volunteers who gave blood and consent to participate in the study and those who attended the VCT center of St. Paul’s Hospital Millennium Medical College during the study period were included.
Exclusion criteria
Those individuals who did not give consent and with age less than 18 years were excluded from this study.
Sample size determination and sampling techniques
Sample size
The sample size was determined using the single-population proportion formula considering the following assumptions: proportion (prevalence) of HIV = 25.3%, 27 level of significance = 0.05 as used in previous studies, degree of accuracy desired (d) = 5% and non-response rate = 10%. The sample size n is calculated by

where Zα/2 is the Z score at 95% confidence interval, the value of which is 1.96.
Sampling technique
Study participants who had VCT service during the study period were recruited from St. Paul’s Hospital Millennium Medical College using a consecutive sampling technique.
Data collection
Interviewer-administered questionnaire adopted from different kinds of studies was employed to gather information on sociodemographic and associated factors. The questionnaire was initially prepared in English, then translated into Amharic and translated back into English to maintain its consistency. The questionnaire data and serum samples were collected by health professionals (nurses, midwifery and doctors).
After pre-test counseling, 4 mL of venous blood was aseptically collected from each of the study participants. Then the blood sample was used for HIV and syphilis testing. The hospital routinely uses commercial HIV test kits according to the national algorithm. These rapid test kits are KHB, STAT-PAK and Uni-Gold which detects the serum anti-HIV antibody (see Appendix 2). Moreover, serum samples were tested for the presence of non-treponemal antibodies using the rapid plasma reagin (RPR; Wampole Laboratories, Princeton, NJ, USA) test following manufacturer’s instructions. The positive samples were further confirmed by Treponema pallidum hemagglutination (TPHA) test.
Quality assurance
Data collectors were trained on the data collection procedure for this particular study to attain standardization and maximize interviewer reliability. Data collected using the questionnaire were checked for completeness at the end of each day. Data collectors were regularly monitored by the supervisor for proper data collection. Standard operating procedures were followed in every step of the sample processing.
Statistical analysis
The data were entered into SPSS version 20.0 (IBM Corp., Armonk, NY, USA) for statistical analysis. Descriptive statistics were used to describe sociodemographic characteristics. Bivariate analysis was done and a 95% confidence interval was calculated.
Ethical consideration
The MSc research project proposal was ethically cleared by the Department of Research and Ethical Review Committee (DREC) and approved by Department of Microbiology, Immunology and Parasitology. Written informed consent was obtained from study participants and letter of permission to conduct the study was obtained from St. Paul’s Hospital Millennium Medical College.
Results
Study participants
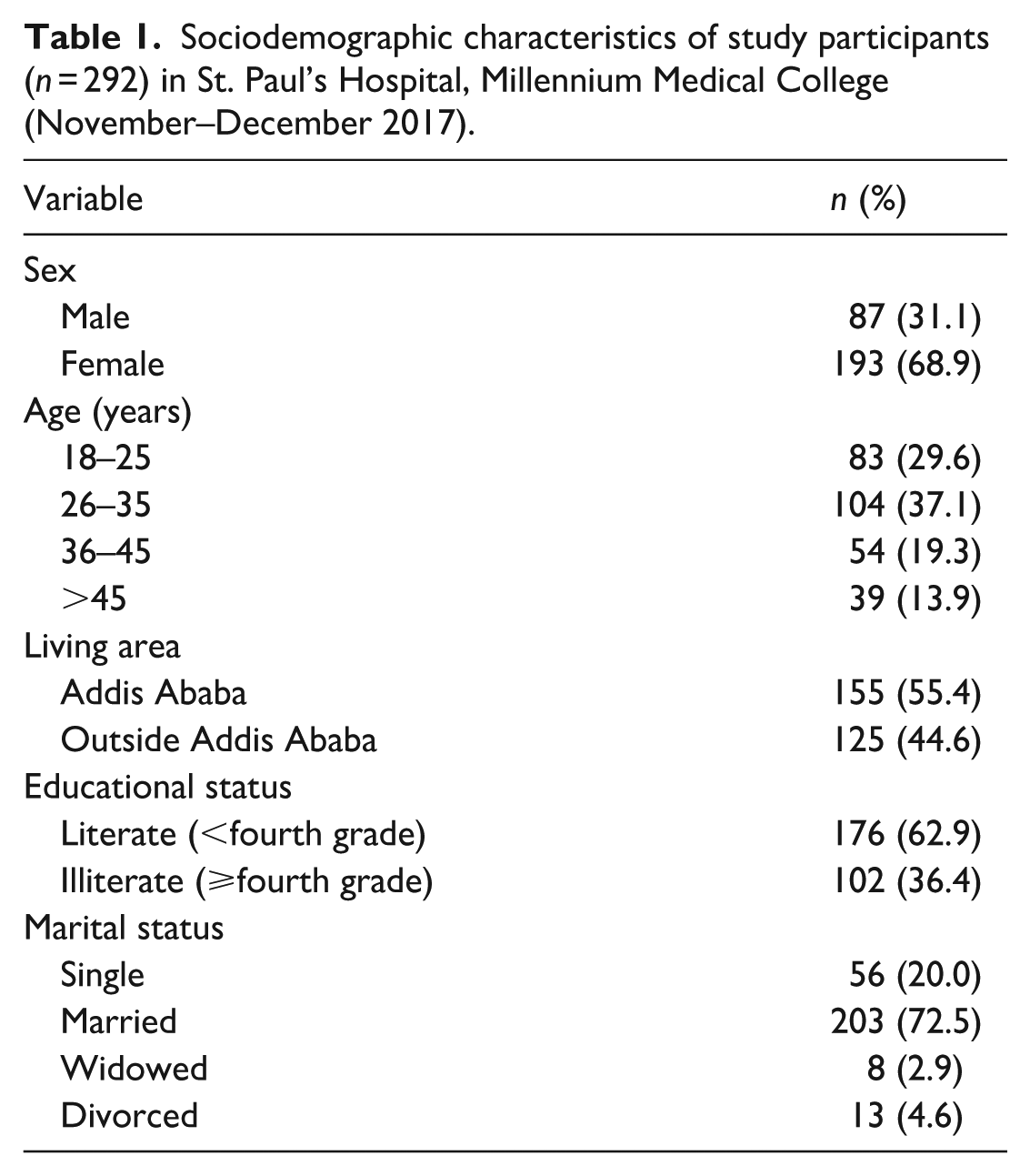
The sociodemographic characteristics of the study participants showed that 31.5% of the study participants were male and 68.5% of the study participants were female. The mean age of the study participants was 33 years and the highest age category was between 26 and 35 years (37.7%) followed by <26 years of age (87/292; 30.0%). The residence of the study participants showed that 55% of the study participants were from Addis Ababa and 45% were from outside Addis Ababa. Most (72.3%) of the study participants were married, 20.4% single, 4.7% divorced and a few of them were widowed (2.86%). Regarding the educational status, 63.7% of the study participants were literate and 36.4% were illiterate (Table 1).
Sociodemographic characteristics of study participants (n = 292) in St. Paul’s Hospital, Millennium Medical College (November–December 2017).
HIV status
The overall prevalence of HIV infection in this study was 2.86%. Around 3.45% of the males and 2.59% of the females were positive for HIV infection and the analysis of HIV infection by age group revealed a slight increase with age and the highest HIV infection was among the 26–35 age group (4.81%; 5/104) (Table 2).
Prevalence of HIV among the study subjects attending the VCT center at St. Paul’s Hospital, Millennium Medical College, Addis Ababa, Ethiopia (November–December 2017).

VCT: voluntary counseling and testing.
Syphilis
The prevalence of syphilis among 292 study participants was 1.7% (5/292) and the prevalence among males and females was 2.2% (2/92) and 1.5% (3/200), respectively. Syphilis was most prevalent among the 36–45 age group (3.7%; 2/54) (Table 3).
Prevalence of syphilis among the study subjects attending the VCT center at St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia (November–December 2017).

VCT: voluntary counseling and testing.
Syphilis and HIV co-infection
All the HIV-positive clients were negative for syphilis and among the HIV-negative patients 1.76% (5/284) were positive for syphilis (Table 4).
Prevalence of syphilis among HIV-positive and HIV-negative individuals among the study subjects attending the VCT center at St. Paul’s Hospital, Millennium Medical College, Addis Ababa, Ethiopia (November–December 2017).
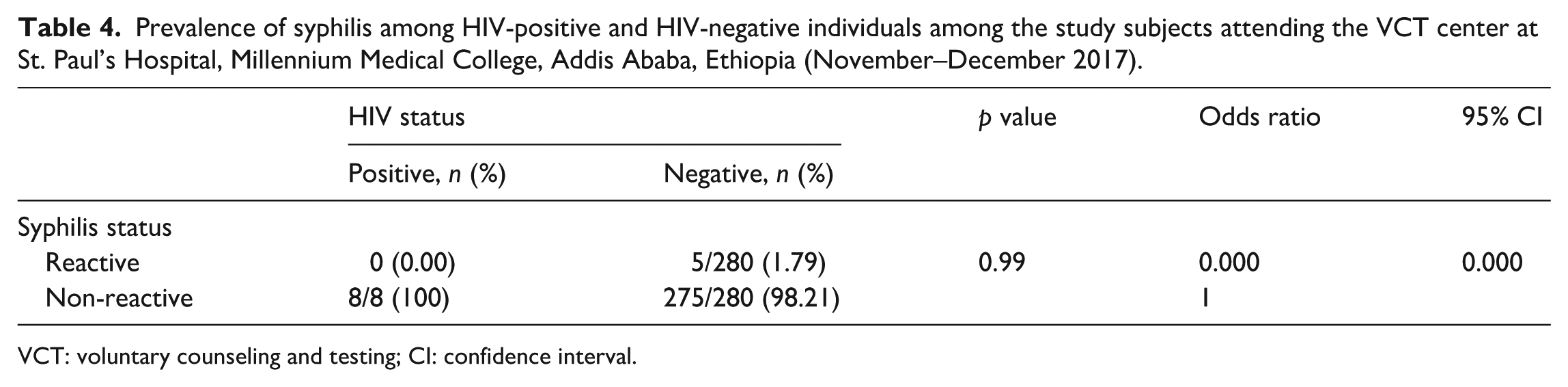
VCT: voluntary counseling and testing; CI: confidence interval.
Associated factors and T. pallidum infection
No associated factors were significantly related to the prevalence of syphilis (Table 5).
Significance of risk factors in syphilis prevalence among the study subjects attending the VCT center at St. Paul’s Hospital, Millennium Medical College, Addis Ababa, Ethiopia (November–December 2017).

VCT: voluntary counseling and testing; RPR: rapid plasma reagin; OR: odds ratio; CI: confidence interval.
p < 0.05 represents statistical significance.
Discussion
STIs represent major public health problems globally. STIs were a major global cause of acute illness, infertility, long-term disability and death, with severe medical and psychological consequences for millions of men, women and infants. Because HIV and T. pallidum are predominantly transmitted sexually, co-infection is very common. 28 These infections were endemic and constitute huge health and economic burden in sub-Saharan countries including Ethiopia. 29
Previous epidemiologic studies conducted among VCT clients, assessed individual infections of HIV and T. pallidum. 30 But this study had tried to ascertain the association of HIV infection with T. pallidum among VCT clients. The results of this study showed the prevalence of HIV and T. pallidum among HIV-positive and HIV-negative individuals from the VCT center in St. Paul’s Hospital Millennium Medical College. Besides, this cross-sectional study provided an important opportunity to assess the status of the HIV infection among clients from Addis Ababa and outside Addis Ababa, since this study institution was a referral hospital.
The finding of HIV in this study was higher than that reported in the 2016 DHS data which was estimated to be 0.9% among the 15–49 age group. 31 Similar findings were found in antenatal care surveillance in rural areas from Ethiopia that showed 2.6% seroprevalence, 2 however lower than the value found in a study conducted in Bahir Dar among pregnant women (6.6%). 32 The higher value reported in this study as compared to the DHS data might be because this study was mainly focused on VCT clients and HIV might be higher in this group than the general population.
Results from these data contrast with a study conducted in urban areas of Ethiopia that showed a high seroprevalence of HIV (12.6%).2,31 This higher prevalence in previous studies might be because the studies were mainly focused on high-risk groups like street dwellers. In this study, HIV-1 seroprevalence from clients outside Addis Ababa was 2.31%. This was in agreement with recent antenatal care surveillance in rural areas from Ethiopia that showed 2.2% seroprevalence. 33 In contrast, based on data from rural areas of Ethiopia, a relatively low seroprevalence of HIV-1 infection was found (1.8%). These data contrast with a recent study conducted among pregnant women from rural sites in the Northwest of Ethiopia that showed a high seroprevalence of HIV (9.4%). 34 These variations of HIV prevalence outside Addis Ababa in different parts of Ethiopia might be due to the norms and cultural differences among the different ethnic groups that might enhance or limit HIV transmission in these areas.
There was no association between gender and HIV infection in this study. The proportion of females seropositive for HIV infection (5/200; 2.5%) was lower than that of males (3/92; 3.3%). This was in line with the study conducted among blood donors. 35 In contrast, a previous study conducted in Gondar showed that the prevalence of HIV among adult women was double that of men. 2 Another study indicated that HIV prevalence was higher among female blood donors (4.19%) compared to males (3.43%). 36 This difference could be due to the different study population used.
In this study, age-specific HIV prevalence was particularly high in the age group of 26–35 years. This was in line with reports from rural Ethiopia which showed a higher prevalence of HIV in this age group. 2 This result was different from national reports which showed that the peak age for HIV infection started from as early as the 15–19 age range in females and 20–24 in males. 37
The overall prevalence rate of syphilis in this study was 1.7% with the highest infection being observed in the age group of 36–45 years, but there was no significant difference between the age groups. In contrast, studies among pregnant mothers showed that the highest prevalence of syphilis was observed in the age group of 21–30. 38
The 1.7% prevalence of syphilis in this study was lower than that in Gondar (10.9%), 2 reports on blood donors in Gondar (4.8%), 35 and 28.8% prevalence among factory workers in Ethiopia. 39 This relatively low cases of syphilis (1.7%) found in this study may be due to the marked declining trend observed in the prevalence of T. pallidum in the last decade among VCT as well as in the general population. This fall was probably due to the use of antibiotics for minor complaints and the more easy availability of drugs among the population. 40
In this study, no cases of HIV–T. pallidum co-infection were found. This supports the marked declining trend observed in the prevalence of T. pallidum in the last decade among VCT clients as well as in the general population. In contrast to this study, an estimated 16% of all patients and 28% of men infected with T. pallidum had co-infection with HIV in the United States. 41
In a study conducted in an HIV clinic in Israel, a significant increase in T. pallidum/HIV co-infection (15.2%) was observed, which was quite different from this study where there were no cases found with HIV/T. pallidum co-infection. 42 This might be due to extensive prevention programs to HIV and the wide use of penicillin and its derivatives which decreased the prevalence of syphilis. 41 But in studies from the Gondar University Teaching Hospital, a statistically significant association was observed between T. pallidum and HIV infection. 12
Results from this study showed that no significant association was found between HIV and T. pallidum, and associated factors. Based on data from a previous study, the prevalence of HIV and T. pallidum infections correlated with the number of sexual partners where all HIV-positive cases except one and 84.1% of all participants who were seropositive for T. pallidum had a history of multiple sexual partners, which was contrary to this study. 2
Conclusion
Results from this study indicated that the prevalence of HIV and T. pallidum was 2.86% and 1.7%, respectively. None of the study participants were co-infected with T. pallidum and HIV. The low seroprevalence of HIV-1/2 and T. pallidum in VCT clients observed in this study might be associated with the expansion of health programs that Ethiopia had implemented in the last decade.
Recommendation
T. pallidum and HIV prevalence in this study were low as compared to previous studies, but their prevalence was above 1% and they are still an important public health problem. Therefore, control strategies and interventions should be comprehensive and should include T. pallidum screening along with HIV testing in VCT centers.
Limitations
This study used the consecutive sampling technique rather than the simple random sampling technique, and the two populations were not matched. The limitations of the majority of serological tests, especially the antibody detection in HIV and the cardiolipin test (RPR) in syphilis, may show false-positive results and these limitations should be considered in this study. The questionnaire was neither validated nor pilot studied. In this study, we took 25.3% of the prevalence of HIV in a previous study to calculate the sample size, but it is better to calculate the sample size for each dependent variable.
Footnotes
Acknowledgements
H.W.H. would like to thank Dr D.A., Professor (MD, MSc, PhD), and Dr Y.W., Associate Professor (MD, MSc, PhD), Department of Microbiology, Immunology and Parasitology Faculty of Medicine, Addis Ababa University for their unreserved support during the writing of this research paper. H.W.H. wishes to thank Dr Tola Bayisa (MD, Internist, Assistant Professor) and Dr Liya Tadesse (V. Provost. Medical Services) for their grateful support. H.W.H. would also like to thank all study participants for their cooperation. H.W.H. is grateful to Addis Ababa University for funding this research project.
Author contributions
H.W.H. initiated the idea of this work and selected the title. All authors provided necessary information for the design, proposal development and supervision during data collection, data analysis and writing of the manuscript.
Availability of data and materials
The data sets used and/or analyzed during the current study were available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
This MSc research project proposal was ethically cleared by the Department of Research and Ethical Review Committee (DREC) and approved by Department of Microbiology, Immunology and Parasitology of Addis Ababa University.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Addis Ababa University. The funder had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Informed consent
Written informed consent was obtained from study participants and letter of permission from St. Paul’s Hospital Millennium Medical College.