
Abstract
Background:
Schistosomiasis contributes to 2.5 million disability-adjusted life years globally. Acute and chronic respiratory morbidity of Schistosoma mansoni (S. mansoni) is poorly documented in the literature. We conducted a rapid literature review of the burden of respiratory symptoms and lung function abnormalities among patients with S. mansoni. We also report the immunologic and lung imaging findings from the studies reviewed.
Methods:
We carried out a comprehensive literature search in Embase and MEDLINE from the inception of the databases to 13th March 2023.
Results:
A total of 2243 patients with S. mansoni were reported from 24 case reports, 11 cross-sectional studies, 7 case series, 2 cohort studies and 2 randomized controlled trials. The prevalence of any respiratory symptom was 13.3–63.3% (total number of patients studied, n = 149). The prevalence of the individual symptoms among patients with S. mansoni in whom respiratory symptoms were sought for was as follows: cough (8.3–80.6%, n = 338), dyspnea (1.7–100.0%, n = 200), chest pain (9.0–57.1%, n = 86), sputum production (20.0–23.3%, n = 30) and wheezing (0.0 – 20.0%, n = 1396). The frequency of the symptoms tended to be higher in acute schistosomiasis. Restrictive lung disease was prevalent in 29.0% (9/31). The commonest chest imaging findings reported were nodules (20–90%, n = 103) and interstitial infiltrates (12.5–23.0%, n = 89). Peripheral blood eosinophilia was prevalent in 72.0–100.0% of patients (n = 130) with acute schistosomiasis and correlated with symptoms and imaging abnormalities. Three case reports in chronic S. mansoni reported elevated C-reactive protein, leucocyte, neutrophil and absolute eosinophil counts, eosinophil percentage, IgE and IgG4.
Conclusion:
There is a high prevalence of respiratory morbidity among patients with S. mansoni, particularly in the acute stage of the infection, although the studies are relatively small. Larger studies are needed to characterize respiratory morbidity in chronic schistosomiasis and determine the underlying clinical and immunological mechanisms.
Plain language summary
Bilharzia causes significant health problems among those affected. However, little is known about respiratory problems associated with bilharzia. We systematically searched for studies published on bilharzia and respiratory problems in literature. We found that a high proportion of people with bilharzia report cough, difficulty in breathing, chest pain, sputum production and wheezing. Also, a good number have lung function impairment and abnormalities on X-ray imaging. Blood eosinophils tended to be associated with the respiratory symptoms and imaging abnormalities which suggests that eosinophils may be involved in causing respiratory problems. We conclude that lung problems are common among people with bilharzia although the studies reviewed were small and mostly among people with acute infection. Larger studies are needed to further characterise lung problems in Bilharzia.
Background
Schistosomiasis contributes 2.5 million disability-adjusted life years globally. 1 Despite mass administration of praziquantel, more than 40% of individuals are subsequently reinfected with Schistosoma mansoni (S. mansoni). 2 Strategic actions are needed to improve the scientific understanding of the parasitic life cycle, diagnostics and effective interventions to achieve elimination as a public health problem in the affected countries by 2030. 1 Schistosomiasis-related morbidity is dependent on the species of the Schistosome involved. S. mansoni is the predominant intestinal schistosome which, in its severest form, causes portal hypertension that manifests with variceal bleeding and ascites. 3
Respiratory morbidity associated with schistosomiasis is less recognized in literature. Nonetheless, the acute infection is characterized by cough, haemoptysis, wheezing, and chest pain that occur about 2–12 weeks from the initial infection and is attributed to larval migration of the worm and initial egg deposition.4,5 Lung imaging studies report interstitial infiltrates, ill-defined nodular and ground glass opacification and/or consolidative changes which endure beyond the acute phase of the infection. 5 In chronic schistosomiasis, small clinical reports highlight a reduction in the forced vital capacity (FVC) 6 and forced expiratory volume in 1 s (FEV1), 7 and a decrease in exercise tolerance. 8 Further, specific complications of S. mansoni present with respiratory symptoms that have not been well characterized in literature. Pulmonary hypertension (PHT) is thought to occur in the setting of hepatosplenic schistosomiasis and this allows portal shunting and embolization of eggs to the pulmonary vasculature. 5 Patients with PHT can present with dyspnea, sleep-related breathing disorders, low 6-min walk distance and cor pulmonale which could impair the quality of life of these individuals.5,7,9 Additionally, more than a third (34%) of patients with hepatosplenic schistosomiasis have been reported to have a hepatopulmonary syndrome caused by pulmonary vasodilation and is characterized by dyspnea, platypnea, peripheral cyanosis and digital clubbing. 6
Characterizing the burden of respiratory symptoms and lung function abnormalities will increase awareness among care providers to attend to respiratory morbidity in acute and chronic schistosomiasis. The main objective of this review is to characterize the burden of respiratory symptoms and lung function abnormalities among patients with S. mansoni. We further describe the immunological and imaging findings as reported in the studies reviewed.
Materials and methods
Study design
This is a rapid review of literature published on respiratory morbidity among patients with S. mansoni. Our report follows the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) checklist. 10
Information sources
We carried out a comprehensive literature search in Embase and MEDLINE from the inception of the database to 13th March 2023.
Search strategy
We used the search query: (‘schistosoma mansoni’/exp OR ‘schistosoma mansoni’) AND (‘cough’ OR ‘dyspnea’ OR ‘wheezing’ OR ‘hemoptysis’ OR ‘chest pain’ OR ‘respiratory failure’ OR ‘pneumonia’ OR ‘forced vital capacity’ OR ‘fvc’ OR ‘forced expiratory volume’ OR ‘fev’ OR ‘exercise intolerance’) AND [(embase)/lim OR (medline)/lim OR (preprint)/lim].
Eligibility criteria of the included studies
Inclusion criteria
We included studies and abstracts that reported data on respiratory symptoms and lung function abnormalities among patients with S. mansoni. As such, any case report, case series, cross-sectional studies, cohort studies, and clinical trials were included.
Exclusion criteria
Studies that reported respiratory morbidity in schistosomiasis but did not disaggregate the data by schistosome species were excluded. Animal studies, narrative reviews, editorials and commentaries were excluded as well.
Selection process
After the database search, duplicates were removed automatically, and titles and abstracts were exported to MS Word. Thereafter, two reviewers (JBB and RO) screened the titles and abstracts of all the articles retrieved to remove articles that are unrelated to the study question. The full text of the articles that passed this initial screen were then retrieved and assessed by two investigators independently (JBB and RO). Any disagreements were resolved by consensus.
Data collection process
We designed a data extraction form to capture data on study variables (see below). One reviewer (JBB) extracted the data from each article and a second reviewer (RO) cross-checked the accuracy of the data collected.
Data items
We collected data on the following variables: first author’s name, publication year, the country in which the study was done, type of study, number of participants with S. mansoni, clinical stage of S. mansoni (acute versus chronic S. mansoni), the proportion of patients with any respiratory symptom and the proportion of participants with any of cough, wheezing, chest pain, dyspnea, hemoptysis and sputum production. Data on signs of tachypnea and prolonged expiration were also abstracted. We also extracted data on proportion of patients with S. mansoni with lung function abnormalities (reduced FVC, FEV1, and FVC/FEV1). Any immunological and imaging abnormalities reported in the eligible studies are reported, although this was not a primary objective of the review.
Data analysis and synthesis
The results are presented descriptively. For all the case reports, where one patient is reported on, the proportion of a given outcome is reported by dividing the frequency of that outcome to the total number of case reports. These were computed using Microsoft Excel®.
Results
Study selection
Figure 1 shows the PRISMA diagram. A total of 274 records were retrieved from our database search. After removing 104 duplicate records, 170 records were screened by title and abstract and 53 records were retrieved for full text screening. Seven records were excluded, of which three did not provide relevant data,11–13 respiratory symptoms were attributed to other causes in two records14,15 and respiratory symptoms specific for S. mansoni were not enumerated in the other two records.16,17

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram showing the results of the data base search and record screening process.
Study characteristics
A total of 2243 patients with S. mansoni were reported from 24 case reports (24 patients), 11 cross-sectional studies (1121 patients), 7 case series (45 patients), 2 cohort studies (53 patients) and 2 randomized controlled trials (1000 patients). Of all the studies, 26 (56.5%) were published more than 10 years ago (before 2013). Most studies were from Brazil (n = 11, 23.9%) and Israel (n = 5, 10.9%). Only 8 (17.4%) reports were from countries in sub-Saharan Africa. Half of the studies (n = 23) were among patients with acute schistosomiasis. Table 1 summarizes the study characteristics.
Characteristics of studies included.

Source of infection is reported for only the eight patients with respiratory symptoms.
RCT, randomized controlled trial.
The prevalence of any respiratory symptoms in S. mansoni
Of the 2243 patients, 380 (16.9%) had acute schistosomiasis and the rest had chronic schistosomiasis. The prevalence of any respiratory symptom was 57.1–63.3% in four studies (n = 89)20,28,52,62 but the study by Schwartz et al. (n = 60) reported a low prevalence of 13.3%. 24 All these studies were among patients with acute schistosomiasis except the case series by Gobbi et al. 52 (n = 7) which reported a prevalence of 57.1% of a respiratory symptom in chronic schistosomiasis.
The prevalence of individual respiratory symptoms in S. mansoni
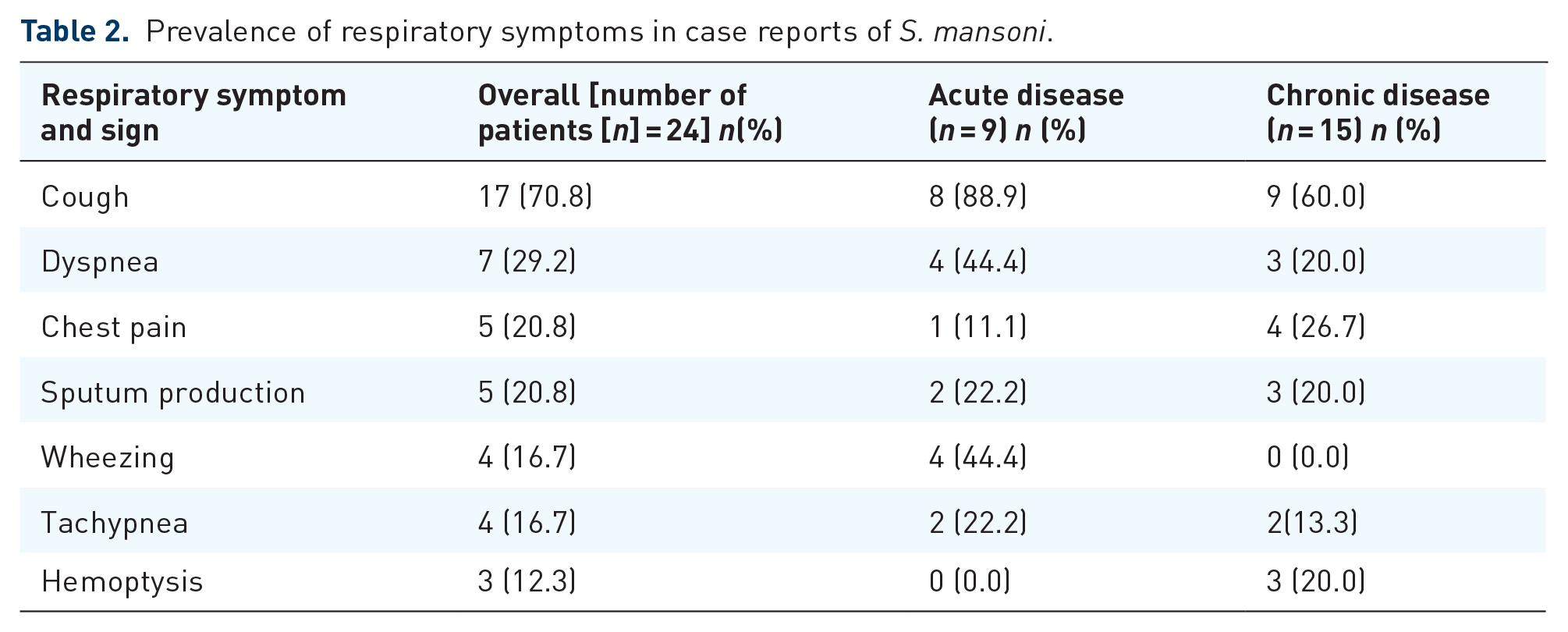
In the 24 case reports of patients with S. mansoni (Table 2), the commonest symptoms were cough (70.8%), dyspnoea (29.2%), chest pain (20.8) and sputum production (20.8%). In the other studies (Table 3), the prevalence of respiratory symptoms among patients with S. mansoni in whom respiratory symptoms were sought for was: cough (8.3–80.6%),19,20,22,24,26–28,33,38,39,44–46,52 dyspnea (1.7–100.0%),20,22,24,26,28,39,30,41 chest pain (9.0–57.1%),20,22,26,39,52,60 sputum production (23.3%) 20 and wheezing (0.0–20.0%).20,22,46,51,58 The prevalence of the symptoms was mostly lower in chronic than acute schistosomiasis (Tables 2 and 3).
Prevalence of respiratory symptoms in case reports of S. mansoni.
Prevalence of respiratory symptoms in studies of S. mansoni other than case reports.

The estimates are ranges reported in the studies cited in the last column.
The prevalence of lung function abnormalities among patients with S. mansoni
Only three studies reported lung function abnormalities. De Jesus et al. 26 reported that 29.0% (9/31) of patients with acute schistosomiasis had a restrictive lung disease pattern which persisted in 9.7% (3/31) patients at 5 months of follow-up. A restrictive lung pattern (low forced vital capacity and/or forced expiratory volume in 1 s) was also reported by two case reports in acute and chronic S. mansoni.18,56
Chest imaging abnormalities among patients with S. mansoni and respiratory symptoms
In acute schistosomiasis, Nguyen et al. 28 (n = 10) and Schwartz et al. 24 (n = 8) found that all patients (100%) had imaging abnormalities, including asymptomatic individuals. The prevalence of the different imaging abnormalities on chest X-ray or CT scan were: nodules (20–90%, n = 103),20,22,24,28,45 interstitial infiltrates (12.5–23.0%, n = 89),24,26,45 consolidation (10–40%, n = 15),22,28 bronchial wall thickening (66.7%, 20/30) 20 and ground glass opacities (50.0%, 5/10). 28
In chronic schistosomiasis, lung nodules,48,52 patchy consolidation, 56 interstitial infiltrates, 25 pleural effusion and segmental lung collapse, 23 cavitary disease 49 and a pseudotumour 34 were reported in case reports.
Immunological markers among patients with S. mansoni and respiratory symptoms
In cross-sectional studies and case series, peripheral blood eosinophilia was observed in 72.0–100.0% of patients (n = 130) with acute schistosomiasis.20,22,26,33,62 Relative eosinophilia (elevated eosinophil percentage) was reported in 80% (8/10) in a case series by Nguyen et al. 28 In that study, symptoms correlated with the degree of eosinophilia and not with chest CT abnormalities. Conversely, in the study by Rocha et al., 20 peripheral blood eosinophilia correlated with imaging abnormalities.
In nine case reports of acute schistosomiasis,18,29,31,32,37,40,42,54,55 peripheral blood eosinophilia was reported in 55.6% (5/9), relative eosinophilia in 44.4% (4/9), leukocytosis in 44.4% (4/9), elevated C-reactive protein in 22.2% (2/9) and elevated immunoglobulin (Ig) E, and thrombocytosis in 11.1% (1/9) each. Eosinophilia in bronchoalveolar lavage was reported in one case. 18
Three case reports49,53,56 reported immune biomarkers in chronic schistosomiasis among patients with respiratory symptoms. These reported an elevated C-reactive protein, leucocyte, neutrophil and absolute eosinophil counts, 49 eosinophil percentage,53,56 IgE, 53 and IgG4. 56 Leukopenia and thrombocytopenia, 53 as well as a normal CRP level and absolute eosinophil count, were also reported. 56
Discussion
In this rapid review, we describe the prevalence of respiratory symptoms and lung function abnormalities among patients with S. mansoni. We found a high prevalence of respiratory morbidity: any respiratory symptom (up to 63%), restrictive lung disease (29%), and chest imaging abnormalities (up to 100%). The findings highlight the need for surveillance for respiratory morbidity among patients with acute and chronic S. mansoni. This is particularly important in sub-Saharan Africa, which carries a disproportionate burden of schistosomiasis, yet only 17% of the studies in our review were from this region. 64 Interestingly, the reports published elsewhere in our review were mostly from travellers or immigrants from Africa.
We observed that patients with chronic schistosomiasis had a relatively lower frequency of respiratory symptoms than those with acute schistosomiasis. This is likely because larval migration and initial egg deposition in the lungs is a key component of the lifecycle of the schistosome in the human host where it elicits granuloma formation, and macrophage and eosinophil rich structures in the acute infection. 4 The studies reviewed reported blood eosinophilia and eosinophilia in bronchoalveolar lavage to suggest that eosinophils are involved in driving lung pathology.18,20,22,26,33,62 Nguyen et al. 28 and Rocha et al. 20 further demonstrated that the eosinophil count correlated with symptoms and imaging abnormalities, respectively. It is unknown if eosinophils can be a therapeutic target for ameliorating acute and chronic respiratory morbidity. This deserves further evaluation.
There were few clinical reports among people with chronic schistosomiasis and therefore the burden of respiratory symptoms is largely unknown in chronic S. mansoni. The same goes for lung function abnormalities where all the reports in our review were in acute schistosomiasis.18,26,56 It was interesting to observe that the restrictive lung disease was persistent in 10% of individuals, 5 months after the acute infection. 26 Future studies could evaluate spirometric abnormalities among people with chronic schistosomiasis. From our review, chest radiographs of patients with chronic S. mansoni showed lung nodules, patchy consolidation, interstitial infiltrates, pleural effusion and segmental lung collapse, cavitary disease and a pseudotumour. It is unclear whether these are enduring features from the acute infection, or they occur as a result of porto-systemic shunting of eggs from hepatosplenic schistosomiasis. 65 Chest imaging of patients with schistosomiasis is desirable to further characterize imaging abnormalities in chronic S. mansoni. It would be important to rule out other concurrent comorbidities that could confound or worsen respiratory morbidity. In this review, smoking18,48 and co-infections such as coccidiomycosis, tuberculosis, Human immunodeficiency virus infection and pneumonia21,25,47,55 were reported in case reports.
To our knowledge, this is the first review of respiratory morbidity among patients with S. mansoni. Nonetheless, there are some limitations to it. The studies were mostly small, and few were from sub-Saharan Africa. This suggests that the findings are not representative of the most affected populations. This calls for more studies to evaluate respiratory morbidity in this region. Relatedly, chronic schistosomiasis, which is the more prevalent form of the disease, is underrepresented, particularly when it comes to lung function abnormalities. Moreover, a contemporary evaluation of respiratory morbidity is needed, since most studies were conducted more than 10 years ago. Additionally, this was a rapid review and was limited to a few databases. As such, this could have excluded other studies that are relevant. Nonetheless, our goal was to provide preliminary estimates for respiratory morbidity in S. mansoni to raise awareness on this subject. A non-exhaustive list of potential areas of further research is shown in Table 4.
Areas for further research in S. mansoni and respiratory morbidity.

Conclusion
The burden of respiratory morbidity is high among patients with acute and chronic schistosomiasis, although most studies are old, have a small sample size and are predominantly among people with acute schistosomiasis. Larger studies are needed to evaluate respiratory morbidity in chronic schistosomiasis, the more prevalent form of the disease, especially where the burden is high as the case is in sub-Saharan Africa.