
Abstract
Background:
The first case of COVID-19 virus was reported in Africa on 14 February 2020. The pandemic became more aggressive in the continent during the second wave than the first wave. Promoting vaccination behavior is an unparalleled measure to curb the spread of the pandemic. Regarding this, the health belief model (HBM) is the major model for understanding health behaviors. This study aimed to examine predictors of intended COVID-19 vaccine acceptance in the second wave of the pandemic among university students in Ethiopia using HBM.
Methods:
A cross-sectional study was conducted among 423 randomly selected medical and health science students at the University of Gondar from 21 August to 15 September 2020. Analysis of data was performed using STATA 14.0. Linear regression analysis was applied and a p value of less than 0.05 was used to declare statistical significance.
Results:
Among the total participants, 293 [72.2% (95.0%: CI: 67.2–76.8)] of them scored above the mean of COVID-19 vaccine acceptance. HBM explained nearly 46.3% (adjusted R2 = 0.463) variance in intention to receive the COVID-19 vaccine. Year of study (β = 0.288; 95% CI: 0.144–0.056), using social media (β = 0.58; 95% CI: 1.546–2.804), existing chronic disease (β = 0.12; 95% CI: 0.042–0.433), perceived overall health condition (β = 0.117; 95% CI: 0.307–0.091), perceived susceptibility (β = 0.58; 95% CI: 1.546–2.804), perceived benefit (β = 0.338; 95% CI: 1.578–2.863), and cues to action (β = 0.49; 95% CI: 0.388–0.99) were significantly associated with intended COVID-19 vaccine acceptance at p value < 0.5.
Conclusion:
Approximately, three-quarters of the participants were above the mean score of COVID-19 vaccine acceptance, which is higher compared to previous reports in resource-limited settings. Interventions in this study setting chould include placing emphasis on the risks of acquiring COVID-19, enhancing perceived benefits of COVID-19 vaccination and improving cues to action by advocating COVID-19 vaccination. Our findings also implied that social media health campaigns are significant factor in COVID-19 vaccination behavioral change in this study setting.
Introduction
The COVID-19 pandemic has become a major public health threat which needs the attention of the international community.1,2 During this survey, at the end of September 2021, the pandemic had affected 233.503 million people in the world. 3 The COVID-19 virus was reported in Africa on 14 February 2020.4,5 The second wave of COVID-19 affected most of the world, which constituted an imminent threat to society, with an immense toll in terms of human lives and the economy.6,7
Even if the first wave of the COVID-19 pandemic spread more slowly in Africa compared to other continents, the second wave became more aggressive with many more cases. 8 Ethiopia registered COVID-19 cases since 13th of March 2020 and became the fifth most affected country in Africa. 9 COVID-19 began its second wave in Ethiopia in early March 2021. 10 There had been 345,674 confirmed cases of COVID-19 with 5582 deaths according to reports at the end of September, 20213,11
Despite the immense efforts of the scientific community, there is no widely recommended treatment modality for COVID-19.12,13 This leads scientists to shift their attention to developing cost-effective vaccines. Vaccination is a safe and effective approach to control the pandemic, in addition to other protective preventive measures. 14 WHO and its member states set a plan to vaccinating 70% of the population to reach population-level herd immunity. 15
In Ethiopia, the government took several public health initiatives and policy measures to prevent the pandemic; these included restricting large gatherings, hand-washing and social distancing. 16 However, those public health and policy measures weren’t widely implemented during the second wave of the COVID-19 pandemic in different parts of the world, including Ethiopia. 17 At the beginning of July, the Ethiopian government completed the first round of vaccination programs for health professionals.18,19 However, only health professionals were invited to receive the vaccination in the first wave of the pandemic due to resource scarcity.20,21 Despite daily infection being higher during second wave than the first wave, COVID-19 vaccine hesitancy remains challenging for voluntary vaccine uptake. 8 COVID-19 vaccine acceptance is the action of consenting or not being hesitant to take the vaccine.22,23
Previous evidence, elsewhere in the world, has examined the levels and determinants of intention for COVID-19 vaccination.20,24–29 Recent findings in Ethiopia showed low trust in the vaccine among the population20,21,30–34 as one of the reasons for the increased spread during the second wave pandemic. According to reports of research findings during the first wave of this pandemic, the major determinants of vaccination intention were: education level, gender, perceived risk of getting COVID-19, family history of COVID-19, religion, access to social media, perceived risk of the vaccine, perceived benefit of the COVID-19 vaccine35–46 and HBM constructs.26,46–49
HBM has been one of the most widely used conceptual frameworks which was originally formulated to explain preventive health behavior since 1950. 50 The HBM suggests that a person’s belief in a personal threat of an illness (perceived barriers, perceived susceptibility and perceived severity of diseases) or disease together with a person’s belief in the effectiveness of the recommended health behavior (perceived benefit) or action will predict the likelihood the person will adopt the behavior (cues to action). Overall, the HBM covering the five constructs: perceived susceptibility, perceived severity, perceived benefits, perceived barriers, and cues to actions. 51
All the available evidence from previous studies in Ethiopia implied poor COVID-19 vaccine acceptance among health care providers and the general population.21,32,33 However, we noted a lack of research focusing on the COVID-19 vaccine acceptance among university students in resource-limited setting, particularly studies that examined the HBM approach for vaccination behavior modification were limited in Ethiopia. As it was justified in extant research of low-income countries, religious and traditional beliefs may aggravate the COVID-19 vaccine hesitancy and the misconceptions in Ethiopia. Scholars also stressed misinformation and conspiracy theories could circulate easily in resource-limited countries like Ethiopia due to the low media access and cultural factors.26,52 We also argued that the cultural tightness among the communities of low-income countries might be another concern which increases the suitability of the study at this time in this research setting.
Assessing behavioral change by applying different theories is a major means of identifying measurements to be taken so as to enhance vaccine uptake.26,52 Additionally, the Ethiopian government opened the first volunteer vaccination program for university students prior to a week of the data collection period of this study which makes conducting studies on COVID-19 vaccine acceptance critical before actual use. Medical and health science students are susceptible to COVID-19 since they have contact with different patients at the time of their internship. University of Gondar Hospital is found in the densely populated City of Gondar and has high patient flows which increase the chance of susceptibility. However, studies which assessed the vaccination behavior and health beliefs of medical and health science students in this study setting were limited. We therefore conducted a study to determine the determinants of intended COVID-19 vaccine acceptance among health and medical science students at University of Gondar, Northwest Ethiopia using HBM.
Methods
Study design, setting, and period
A cross-sectional study was conducted among 423 participants at University of Gondar from 21 August to 15 September 2020. Our target population was medical and health science students at University of Gondar (a total of 5283 students). The educational system in Ethiopia consists of 6 years term of study for medical science students, 5 years term of study for pharmacy students and 4 years term of study for other health science students. The University of Gondar is found in the historical city of Gondar, Northern Ethiopia. Gondar is the capital city of the central Gondar zone and is located 737 km away from Addis Ababa, the capital city of Ethiopia. Gondar city is a well-known tourist destination and is densely populated. Medical and health science students of University of Gondar have completed their internship and given voluntary service at University of Gondar Comprehensive Specialized Hospital. This hospital is among the largest hospitals in Ethiopia and has high patient flow. The hospital serves more than 13 million people in the catchment area and it is a sole referral center in North-West Ethiopia.
Source and study populations
All medical and health science students who attended their education at University of Gondar were recruited as source population while medical and health science students who attended at University of Gondar and who were available during the study period and willing to participate in the study were considered as the study population.
Study participants, sample size, and sampling procedure
The study participants were health and medical science students at University of Gondar. The sample size was determined by using the single population proportion formula by assuming P = 50% (since previous studies particularly on university students’ vaccination acceptance weren’t found in similar study setting), a 95% level of confidence, a 5% of margin of error and 10% of the non-response rate. Finally, a total sample size (n) of 423 was obtained. Simple random sampling technique was used to recruit study participants from each department. First, sampling frame was prepared by taking student list from each department. Then, the total sample size (n = 423) was proportionally allocated to each department. Finally, students were recruited randomly in each department.
Data collection tool, quality control, and procedure
Data were collected using a pretested self-administered questionnaire that was adapted by reviewing different literatures.26,27,48,53–56 Questionnaire was prepared in English language and pretested on a group of 22 students at Bahirdar University which was similar to our study setting. Content validity was checked by using views of experts and correction was made accordingly. Four data collectors and two supervisors participated in the data collection process. Training was given for data collectors and supervisors on the objective of the study and data collection procedures.
The questionnaire consisted of four sections. The first section of the questionnaire includes information on sociodemographic variables which had eight item questions.26,52,57,58 Part two was about COVID-19 experience (e.g. Do you currently believe that you have, or think that you recently had, contact with confirmed/suspected COVID-19 patient?) and self-perceived health status (e.g. Do you have an existing chronic disease such as cancer, cardiovascular disease, diabetes, etc.?)59,60 which had five item questions. On the other hand, part three was about COVID-19 vaccine acceptance. COVID-19 vaccine acceptance is the action of consenting to receive or receive the COVID-19 vaccine which was measured using three items with five-point Likert scale questions.21,23,25–27,33,61,62 Ratings were made based on one to five scale where; 1 = absolutely disagree, 2 = disagree, 3 = neutral, 4 = agree and 5 = absolutely agree.26,48,54
The final section of the questionnaire was about HBM predictor variables which covered the five constructs: perceived susceptibility(which was defined as beliefs regarding being infected by COVID-19 measured by three items) 35 ; perceived severity (a person’s perception on the seriousness of being infected by COVID-19 by three items) 62 ; perceived benefits (value of receiving COVID-19 vaccine measured by three items) 27 ; perceived barriers (it included vaccine cost and concerns about vaccine safety and side effects assessed by five items) 26 ; and cues to actions (include information, people and events that guide an individual to be vaccinated by four items).26,29,63
Data processing and analysis
Epi Data version 4.6 and STATA version 14 was used for data entry and analysis, respectively. Descriptive statistics was computed for sociodemographic variables and health-related variables. The test of Pearson correlation was used to show linear correlation of continuous variables with each other. Linearity was checked with scatter plot and multicollinearity was checked using variance inflation factors (VIF) in which no or little multicollinearity was observed. Both simple and multiple linear regression analyses were performed to identify associated factors of intention to use the COVID-19 vaccine. The independent variables in simple linear regression analysis with p < 0.2 were entered into multiple linear regressions. R 2 was calculated to show the proportion of variance which could be explained by the HBM constructs. For multiple linear regressions, the strength of the association was described at 95% CI and p value < 0.05 was considered as statistically significant for multiple linear regressions.
Results
Sociodemographic characteristics
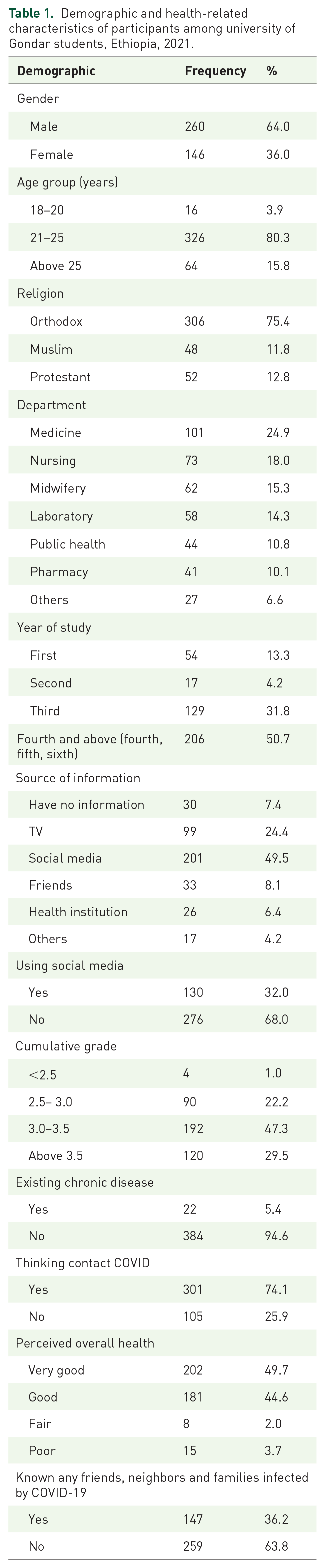
Out of the 423 questionnaires, 406 participants responded with a response rate of 96.0%. Most of the study participants 326 (80.3%) were between the ages of 20 and 25, and the mean age was 22.6 ± 1.2. A total of 260 (64.0%) of the study participants were male. About two-thirds, 306 (75.4%) of the study participants were followers of Orthodox religion. In terms of field of study, about one-fourth, 101 (24.9%) of the study participants were medicine students. About half, 206 (50.7%) of the study participants were above fourth year students (see Table 1 for more detail).
Demographic and health-related characteristics of participants among university of Gondar students, Ethiopia, 2021.
Health beliefs toward COVID-19 vaccine
The reliability was calculated using Cronbach α coefficient to determine the internal consistency of all health belief constructs such as perceived susceptibility, perceived severity, perceived benefit, perceived barriers and cues to action. Cronbach’s alpha value of greater than or equal to 0.7 indicates high reliability, a value between 0.5 and 0.7 indicates moderate reliability and if it is less than 0.5 indicates low reliability. The reliability test of HBM items for Cronbach α ranged from 0.69 for perceived barriers to 0.86 of perceived benefit (see Table 2 for more detail).
COVID-19-related health belief items among university of Gondar students in Ethiopia, 2021.

Correlation analysis between health beliefs and intended COVID-19 vaccine acceptance
According to the result from Pearson correlation (r) there was a strong positive significant correlation between perceived benefit (r = 0.84, p < 0.05) and cues to action (r = 0.81, p < 0.05) with COVID-19 vaccine acceptance whereas perceived susceptibility (r = 0.69, p < 0.05) and perceived severity (r = 0.23, p < 0.05) had moderate significant positive correlation with COVID-19 vaccine acceptance. Additionally, there was a negative weak association between perceived barriers (r = 0.17, p < 0.05) and COVID-19 vaccine acceptance. On the other hand, regarding HBM constructs’ linear correlation with each other, there was no significant linear correlation between cues to action and perceived susceptibility (see Table 3 for more detail).
Pearson correlation of HBM constructs and COVID-19 vaccine acceptance among university of Gondar students, Ethiopia, 2021.
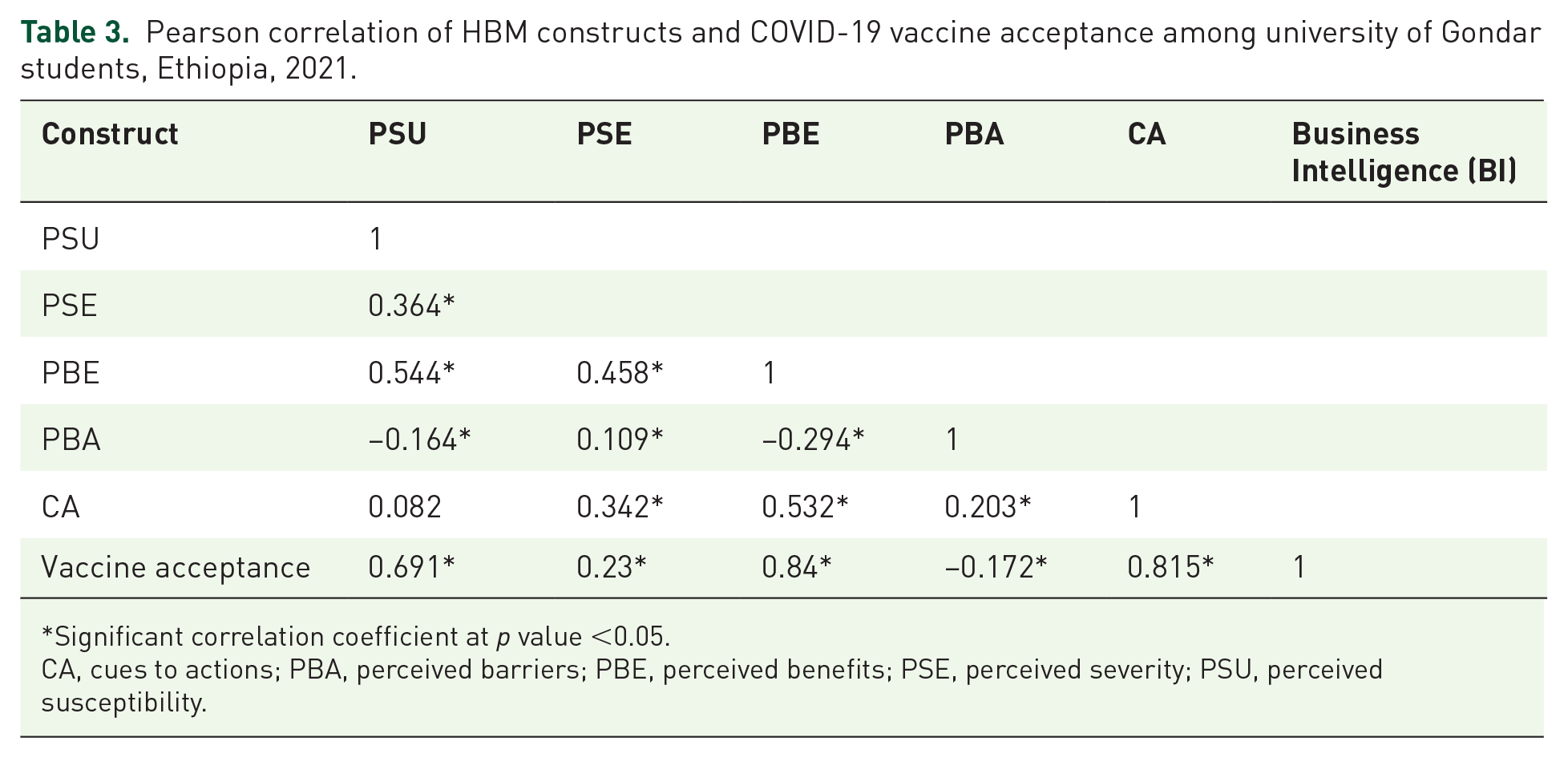
Significant correlation coefficient at p value <0.05.
CA, cues to actions; PBA, perceived barriers; PBE, perceived benefits; PSE, perceived severity; PSU, perceived susceptibility.
Magnitude of intended COVID-19 vaccine acceptance among University of Gondar students, Ethiopia
The study implied that about 293 [72.2% (95.0%: CI: 67.2–76.8)] of participants were scored above the mean score of COVID-19 vaccine acceptance. The mean score of COVID-19 vaccine acceptance was 10.2 and the standard deviation was 3.3 (see Table 4 for more detail).
COVID-19 vaccine acceptance among university of Gondar students, Ethiopia, 2021.

Predictors of intended COVID-19 vaccine acceptance among university of Gondar students, Ethiopia, 2021
Variables such as gender, year of study, using social media, perceived overall health, presence of chronic disease, source of information, contact with known/suspected COVID-19 infected, perceived susceptibility, perceived severity, perceived benefit, perceived barrier, and cues to action were significant in simple linear regression at p value <0.2. Significant variables in simple liner regression were subjected to multiple linear regression to control the confounding effect.
In multiple linear regressions, by controlling other determinants, HBM explained nearly 46.3% (adjusted R 2 = 0.463) of variance to COVID-19 vaccine acceptance. Year of study (β = 0.288; 95% CI: 0.144–0.056), using social media platform (β = 0.221; 95% CI: 0.135–0.325), existing chronic disease (β = 0.12; 95% CI: 0.042–0.433), rating overall health(β = 0.117; 95% CI: 0.307–0.091), perceived susceptibility (β = 0.58; 95% CI: 1.546–2.804), perceived benefit (β = 0.338; 95% CI: 1.578–2.863), and cues to action (β = 0.49; 95% CI: 0.388–0.99) were significantly associated with the COVID-19 vaccine acceptance at 5% level of significance (see Table 5 for more detail).
Multiple linear regression of intended COVID-19 vaccine acceptance among university of Gondar students, Ethiopia, 2021.

Significant coefficient at p value < 0.05. **Continuous variable. ref, reference.
Discussion
The current study was conducted among medical and health science students at University of Gondar in Ethiopia using the HBM during the second wave of the COVID-19 pandemic. To our knowledge, this is the first study to provide insights in developing strategies of HBM-based promotion of COVID-19 vaccination behavior among Ethiopian university students. Medical and health science students are among the most vulnerable groups since they are frequently spending their time with patients in hospital during their internship. In spite of their vulnerability, they were not considered as priority recipients for COVID-19 vaccine. The study revealed that 293 [72.2% (95.0%: CI 67.2–76.8)] of participants were above the mean score of intended COVID-19 vaccine acceptance.
The finding implied approximately three-fourth of university students scored above the mean score of intended COVID-19 vaccine acceptance. This study result is considerably good to reach a required threshold to achieve herd immunity of vaccination uptake which would need to be at least 70%, 15 according to WHO recommendation. This finding is slightly comparable with previous finding in the United States (69%), 64 UK (74.2%), 65 Pakistan (75%) 40 and Vietnam where 76.10% 36 of participants were to get a COVID-19 vaccine respectively.
The current study implied a higher acceptance to receive COVID-19 vaccination than previous findings in Ethiopia which was from 31.3 to 62.6%.20,21,30–34 This could be due to the difference in study participants. Most of those previous studies were conducted among the general population which enables having different reasons for refusal of vaccines. The other possible justification could be the time period in which the studies were conducted. For instance the current studies were conducted in the second wave of the pandemic, while the previous studies were conducted during the first wave of the pandemic. Accordingly, the perception toward the pandemic could change within this time period and individuals might develop positive beliefs about getting the vaccination. Moreover, during the data collection period of this study the Government of Ethiopia declared the availability of enough vaccines for everyone who was willing to receive it, whereas in the study period of those previous findings no vaccination was permitted and available except for health professionals. Hence, the actual availability of the vaccine in the country might be a cause for the change of intention.
The finding in this study is also lower than that of another study conducted in France (77.6%), 39 and among university students in three countries of Europe which was 85.49% 42 and India (89.3%). 29 Whereas the finding was higher than that of two previous studies from the USA, in which the intention to receive the COVID-19 vaccination was 56.8% 22 and 59.1%, 24 and also another study in Japan, which implied 56.1% 25 of participants intended to be vaccinated. It was also higher than other findings elsewhere in the world.23,26,28,30,38,40,45–47,56,57,66,67 The reason for this variation could be the study population and the data collection period. Those previous studies were conducted during the first year of the pandemic in which the trust of the population toward drug companies and vaccine-related beliefs were different and might have changed within this time period. Additionally, the purposive sampling method was used in those previous studies which might be the reason for this discrepancy.
According to the results of linear multiple regression, the year of the study had a positive significant association with COVID-19 vaccine acceptance among sociodemographic factors of this study (β = 0.288; 95% CI: 0.144–0.056). This result was corresponding to the study finding elsewhere in the world.26,44 This could be due to education level difference between junior and senior students. Hence, senior students might have more awareness about vaccine benefits and the severity of the pandemic. Additionally, it is known that senior students are more involved in clinical practice which might enable them to have deeper knowledge and understanding about COVID-19 vaccine and the pandemic itself.
The finding also implied frequent social media platform users (β = 0.58; 95% CI: 1.546–2.804) were more likely candidates for COVID-19 vaccine acceptance. This finding was supported by studies conducted in China.59,60 This could be due to the fact that social media platforms can quickly disseminate information, which might induce COVID-19 vaccine behavioral change. This finding implies that officers of public health institute, government and other concerned bodies should give emphasis to the dissemination of information using social media health campaigns.
Study participants who perceived their overall health as poor (β = 0.117; 95% CI: 0.307–0.091) were more likely to accept COVID-19 vaccine than those who perceived themselves as having a good health condition. This finding was consistent with previous findings elsewhere in the world. 44 The possible justification for this could be that having poor health condition increases the concern and fear of COVID-19 which finally leads to positive beliefs of vaccination behavior. Additionally, this study also showed participants who had chronic diseases (β = 0.12; 95% CI: 0.042–0.433) were more likely to adopt COVID-19 vaccine acceptance. This was corresponding to previous findings elsewhere in the world.26,38 This might be due to their consideration that the chronic disease itself increases their probability of getting the infection and in such case, they develop positive health beliefs toward vaccination behavior. In addition, it is a fact that chronic patients visit hospitals more frequently than healthy people, so this enabled them to understand the direct and indirect impact of COVID-19.
Regarding HBF constructs, the results of this study indicate that perceived susceptibility to COVID-19 pandemic (β = 0.58; 95% CI: 1.546–2.804), perceived benefits of COVID-19 vaccine (β = 0.338; 95% CI: 1.578–2.863) and cues to action (β = 0.49; 95% CI: 0.388–0.99) were major determinants of COVID-19 vaccine acceptance. This was in line with previous research studies.20,23,27,35,40,43 Accordingly, participants who had perceived that they could be infected by COVID-19 were more likely candidates for COVID-19 vaccine acceptance. The finding was consistent with previous finding.21,23,25–27,33,61,62 The justification for this report could be that fear of future susceptibility helps to develop positive beliefs toward COVID-19 vaccine importance. This implied if individuals understand the personal risk of getting infected with COVID-19, they do not hesitate to accept the vaccine.
Individuals who understood the benefit of COVID-19 vaccine uptake for their health were more likely to adopt COVID-19 vaccine acceptance, which was supported by previous reports elsewhere in the world.20,23,27,35,40,43,67 This could be due to the fact that knowing the positive outcome of COVID-19 vaccination enhances the intention to accept it. Strengthening the current finding, a previous report suggests that preventive health care behaviors were strongly influenced by the value that individuals perceived in engaging in such actions. 51
On the other hand, cues to action had positive significant association toward COVID-19 vaccine acceptance. This was supported by previous findings elsewhere in the world.21,26,37,48 The justification could be different events that trigger or stimulate an individual to be vaccinated positively affect their acceptance.
However, the result of this study showed that perceived severity and perceived barriers did not have significant association with COVID-19 vaccine acceptance. This finding is contradictory to previous reports elsewhere in the world in which perceived severity had positive significant association41,53,55 and perceived barriers had negative significant association with COVID-19 vaccine acceptance.37,62,63 The contradiction might be due to the study population and geographical variation as the perceived threat might vary in different socio-demographic conditions.
Strengths and limitations of the study
This was the first study in Ethiopia presenting university students’ vaccination behavior, particularly COVID-19 vaccine acceptance using the HBM approach. Moreover, this study provides up-to-date information on the intention to vaccinate against COVID-19 during the second wave of the pandemic. However, it is difficult to know about the precedence of the problem in detail because the study was cross-sectional. The data for this study was also collected based on self-reported information, which might lead to an overestimation of perceived behaviors. The other limitation of the study was that it did not collect qualitative data. Additionally, this study was limited to only medical and health science students, which might lower the generalizability of the findings.
Conclusion
Approximately, three-quarters of participants were above the mean score of intended COVID-19 vaccine acceptance, which was higher compared to previous reports in resource-limited settings. Correct interventions for promoting COVID-19 vaccination based on HBM should be a primary concern for health policy makers, healthcare providers and planners. Interventions in this study setting could include placing emphasis on the risks of acquiring COVID-19, enhancing perceived benefits of COVID-19 vaccination and improving cues to action by advocating COVID-19 vaccination. Our findings also implied the same; social media health campaigns are factors in COVID-19 vaccination behavioral change.
Supplemental Material
sj-docx-1-tai-10.1177_20499361231213226 – Supplemental material for COVID-19 vaccine acceptance in the second wave of the pandemic among university students in Ethiopia: application of the health belief model
Supplemental material, sj-docx-1-tai-10.1177_20499361231213226 for COVID-19 vaccine acceptance in the second wave of the pandemic among university students in Ethiopia: application of the health belief model by Befkad Derese Tilahun, Tiruneh Adane, Molla Fentanew, Tilahun Dessie Alene, Gebremeskel Kibret Abebe and Habtamu Setegn Ngusie in Therapeutic Advances in Infectious Disease
Footnotes
Acknowledgements
The authors would like to thank the data collectors and the study participants for their collaborations throughout the study period.
Declarations
Availability of data and materials
The data is available on responsible request from the corresponding author by the following address. E-mail:
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.