
Abstract
Candida auris is a fungal organism resistant to several classes of antifungals. Since its identification in 2009, it has gained worldwide attention in healthcare for its virulence and resistance to commonly used antifungal therapeutics. Although its origin and mechanisms of transmission are not fully elucidated, it is widely recognized as a high priority healthcare-associated pathogen. Infection control efforts in skilled nursing facilities have been very challenging due to the tendency of C. auris to persist in the environment and colonize residents. In this narrative review, we discuss the epidemiology and infection prevention of C. auris in skilled nursing facilities. We also identify challenges in the diagnosis and management of both symptomatic infections and asymptomatic colonization.
Keywords
Introduction, brief history, and microbiology
Candida auris is a fungal organism that presents significant challenges to healthcare systems around the world. For patients, systemic infection from this organism can result in poor health outcomes. For clinicians, treatment and infection control can be challenging. With high mortality rates associated with invasive C. auris infections, infection prevention efforts in skilled nursing facilities and other healthcare facilities are crucial to preventing further morbidity and mortality. 1
C. auris was first identified in Japan in 2009 from a patient’s ear drainage, although a subsequent study determined that the organism had been unknowingly isolated in 1996 from a patient’s blood culture samples in South Korea.2,3 Since 2009, multiple clades have been detected in different parts of the world in a short period of time. The first United States C. auris cases occurred between May 2013 and August 2016 among seven patients from Illinois, Maryland, New Jersey, and New York. C. auris was isolated from blood, urine, and ear cultures. Of the seven cases, five isolates were mistakenly identified as C. haemulonii, and five of seven C. auris isolates were resistant to fluconazole. None of these isolates were pan resistant. 4 C. auris may be mistakenly identified as other yeast species including other Candida species, Saccharomyces, and Rhodotorula. 5 The number of patients colonized with C. auris has increased significantly worldwide in the past few years. Increasing case counts pose a significant concern in modern healthcare because of the characteristics of C. auris and its burden to healthcare systems, including high all-cause mortality, difficulty of isolation and detection, multidrug resistance, and its pattern of transmission. 6
The exact origin of C. auris and why this organism appeared in different parts of the world virtually simultaneously still remains unknown. 7 C. auris genome analysis has revealed genome assembly size ranging from 12.1 to 12.7 Mb 8 with approximately 6500–8500 protein coding sequences that encode proteins responsible for its virulence. 9 Whole-genome sequencing of C. auris has previously identified four major clades based on the location in which the first isolates were found: South Asian (Clade I), East Asian (Clade II), South African (Clade III), and South American (Clade IV).10,11 More recently, C. auris isolates from Iran have been recognized to be separated by only 100 single-nucleotide polymorphisms (SNPs) from each other, while they differ from other clades by more than 200,000 SNPs, suggesting that these isolates represent a potential new clade (Clade V).11–15 In the United States, clades I, II, III, and IV have been isolated, with clades I and IV being most common.16,17 Phylogenetic analysis of different clades of C. auris is important as resistance pattern varies by clade type, and it provides valuable insight into its transmission dynamics.16,18 For example, clades I and III have been shown to exhibit distinct phenotypic and antimicrobial susceptibility patterns in vitro. Clade I isolates are able to form pseudohyphae unlike clade III. Also, although a majority of C. auris isolates are resistant to fluconazole, the minimum inhibitory concentrations for fluconazole and voriconazole have been higher in clade III compared with clade I. 19 Clade II appears to have no mutation in the ERG11 gene, which is responsible for encoding the target of azoles, resulting in higher susceptibility to azoles compared to other clades.20,21
C. auris has multiple virulence factors, such as proteinase and phospholipase, that enable the organism to cause invasive disease (e.g., bloodstream infections) similar to other Candida species. 22 In addition, C. auris can form biofilms which enhance its ability to inhabit human skin and act as a barrier to antifungal treatment.23,24 The genetic and molecular mechanisms of C. auris that confer resistance to the major classes of antifungal drugs (i.e., azoles, echinocandins, and polyenes) remain incompletely understood. Mutations in the ERG11 gene that encodes sterol-demethylase enzymes are frequently observed, conferring resistance to fluconazole. Furthermore, the presence of antimicrobial efflux pumps, such as major facilitator superfamily transporters or adenosine triphosphate binding cassette, can reduce susceptibility to azoles and amphotericin B.9,18,25,26
C. auris is difficult to eradicate from surfaces using traditional antiseptic agents. It can colonize and cause invasive fungal infections in vulnerable patient populations with increased exposure to healthcare settings, particularly in individuals who reside in long-term care facilities and the chronically ill. In this review, we aim to address the current understanding of C. auris from the perspective of management in skilled nursing facilities. We will discuss the healthcare epidemiology, risk factors for transmission of C. auris and summarize guidance regarding surveillance, cleaning/disinfection, clinical features of invasive disease, diagnostics, and management amongst residents at skilled nursing facilities.
Healthcare epidemiology
Current state of C. auris epidemiology in skilled nursing facilities
C. auris infection is associated with high morbidity and mortality.1,10 A review of 4733 worldwide cases reported in 33 countries found that overall mortality was 39% associated with C. auris infection, and 45% with C. auris fungemia. 27 It is estimated that ~5%–10% of colonized patients with C. auris eventually develop invasive disease.28,29 It is important to study the epidemiology of C. auris colonization and transmission in patients in skilled nursing facilities because the development of systemic infection potentially can be prevented. Residents in skilled nursing facilities are especially vulnerable to C. auris infection and transmission owing to their clinical characteristics, including multiple hospitalizations, exposures to C. auris from healthcare settings, exposures to antimicrobial agents, frequent contact with healthcare providers, and resource challenges in infection control, which can translate into higher likelihood of invasive C. auris in this setting.28,30
Risk factors
Risk factors for C. auris colonization still remain to be fully characterized. A case control study of residents in New York skilled nursing facilities identified the following risk factors for C. auris colonization: mechanical ventilation, receipt of carbapenem antibiotics in the preceding 90 days, having one or more acute care hospital visit in the prior 6 months, and receipt of systemic fluconazole in the prior 90 days. 28 Similar risk factors were observed in Chicago, Illinois, where the majority of individuals with C. auris colonization or infection had serious medical conditions requiring hands-on care and indwelling medical devices [e.g., intravenous (IV) devices, feeding tubes, tracheostomies], and previously resided in a long-term acute care hospital or ventilator capable skilled nursing facilities in the prior 3 months. 31 A more recent report from a small community hospital located in Western New York illustrated a case in which C. auris was detected from urine after 50 days of hospitalization. There were no epidemiologic or geographic links to C. auris cases elsewhere; however, extensive use of antibiotics and prolonged endotracheal intubation were described prior to the isolation of C. auris in urine, suggesting a possible correlation of antibiotic exposure with colonization or infection with C. auris. 32 Robust antimicrobial stewardship programs at skilled nursing facilities or long-term care facilities are currently needed to optimize antibacterial and antifungal usage in a concerted effort toward C. auris prevention.
Pan-resistant C. auris isolates have been reported rarely, with sporadic, geographically disparate clusters lacking direct epidemiologic linkages.10,33,34 Pan-resistance of C. auris isolates may develop through antifungal pressure during treatment, as observed in New York where three pan-resistant C. auris cases involved patients who had received prior echinocandin treatment. 34 Once developed, pan-resistant C. auris strains can transmit from person to person in healthcare settings.
It is noteworthy that C. auris clusters have occurred on units caring for COVID-19 patients during the pandemic. 35 The relation between COVID-19 treatment and C. auris transmission likely was related to pandemic efforts to conserve personal protective equipment (PPE), such as allowing re-use or extended use of gowns between patients. 36 Such COVID-19-related C. auris outbreaks highlight the importance of following routine infection control measures to prevent transmission of pathogens.
Transmission
Skilled nursing facilities have a significant role in the regional transmission of C. auris within and between healthcare facilities. For instance, epidemiologic relationships were drawn among most cases upon reviewing 77 clinical cases of C. auris in healthcare facilities located in seven states of United States from June 2016 to May 2017. 6 Three Illinois cases were related to one particular long-term care facility. Cases from New York and New Jersey had overlap between hospitals and long-term care facilities. Moreover, isolates from New York and New Jersey were grouped in clade I, and those from Illinois were grouped in clade IV, suggesting separate introductions of C. auris into the United States, with subsequent regional transmission. 6
Contamination of the healthcare environment with C. auris is likely a major driver of transmission to skilled nursing facility residents. Careful surveillance of the healthcare environment in a Chicago skilled nursing facility caring for residents with C. auris demonstrated frequent contamination of the environment (70/100 environmental samples from doorknobs, windowsills, and bed handrails). 37 Notably, the handrails of two beds occupied by noncolonized residents were contaminated with C. auris. Fungal shedding from the occupants was suggested to be a common cause of environmental contamination, with a positive relationship between residents’ C. auris skin burden and environmental contamination. Similar findings were seen in a multi-regional study of six long-term care facilities and one acute care hospital, which showed that environmental C. auris contamination was common in rooms of colonized residents (29%–38%). When the study’s investigators disinfected the room, recontamination of room surfaces occurred quickly (within 4–12 h) and was associated with the number of patient body sites colonized with C. auris. 38
Lastly, shared medical equipment may be important vectors of transmission. During an outbreak of C. auris in an intensive care unit in the United Kingdom, multiple infection control measures were used including weekly screening, contact precautions, and enhanced environmental cleaning. Despite this bundle of infection control measures, the outbreak was not controlled. A case–control analysis found reusable axillary temperature probes that were shared among patients to be a risk factor for C. auris acquisition, and the outbreak was not controlled until the difficult-to-clean probes were removed from the unit. 39
Infection control
Surveillance
Surveillance plays a crucial role in guiding the public health response to C. auris. The World Health Organization (WHO) recognizes the limitation of data on the impact of C. auris in public health due to the general lack of effective surveillance across the globe. 40 Global Antimicrobial Resistance and Use Surveillance System (GLASS) was launched to standardize antimicrobial resistance surveillance in 2015. 41 An early implementation protocol was developed to assist participating nations in developing national surveillance systems incorporating invasive Candida species. 42 For instance, South Korea, one of the first countries to detect C. auris isolates, implemented Kor-GLASS in 2016. 43 From its nine sentinel hospitals, one case of C. auris bloodstream infection was identified out of a total 766 candidemia cases in 2 years of observation. 44 A centralized, global surveillance database for C. auris using this system is not available at this time.
In the United States, C. auris has been a nationally notifiable condition since 2018, and individual states have reporting mandates.45,46 Clinical cases of C. auris reported by local and state health departments are published weekly by the National Notifiable Diseases Surveillance System (NNDSS). 47 However, because not all states of United States mandate reporting of C. auris cases, the NNDSS database of C. auris is incomplete. Figure 1 shows the number of clinical cases of C. auris in the Unites States by state in 2022. Note that some states, such as California, Florida, Illinois, New York, and Nevada, had high incidence of C. auris (101–500 reported cases per state in a 12 months period), whereas it was not reported in some states. 48 For the future, expansion of the current mandatory reporting protocol to all states of United States or establishing a nation-wide, centralized C. auris surveillance system, ideally with genomic sequencing data, would be helpful for comprehensive surveillance and tracking of C. auris.
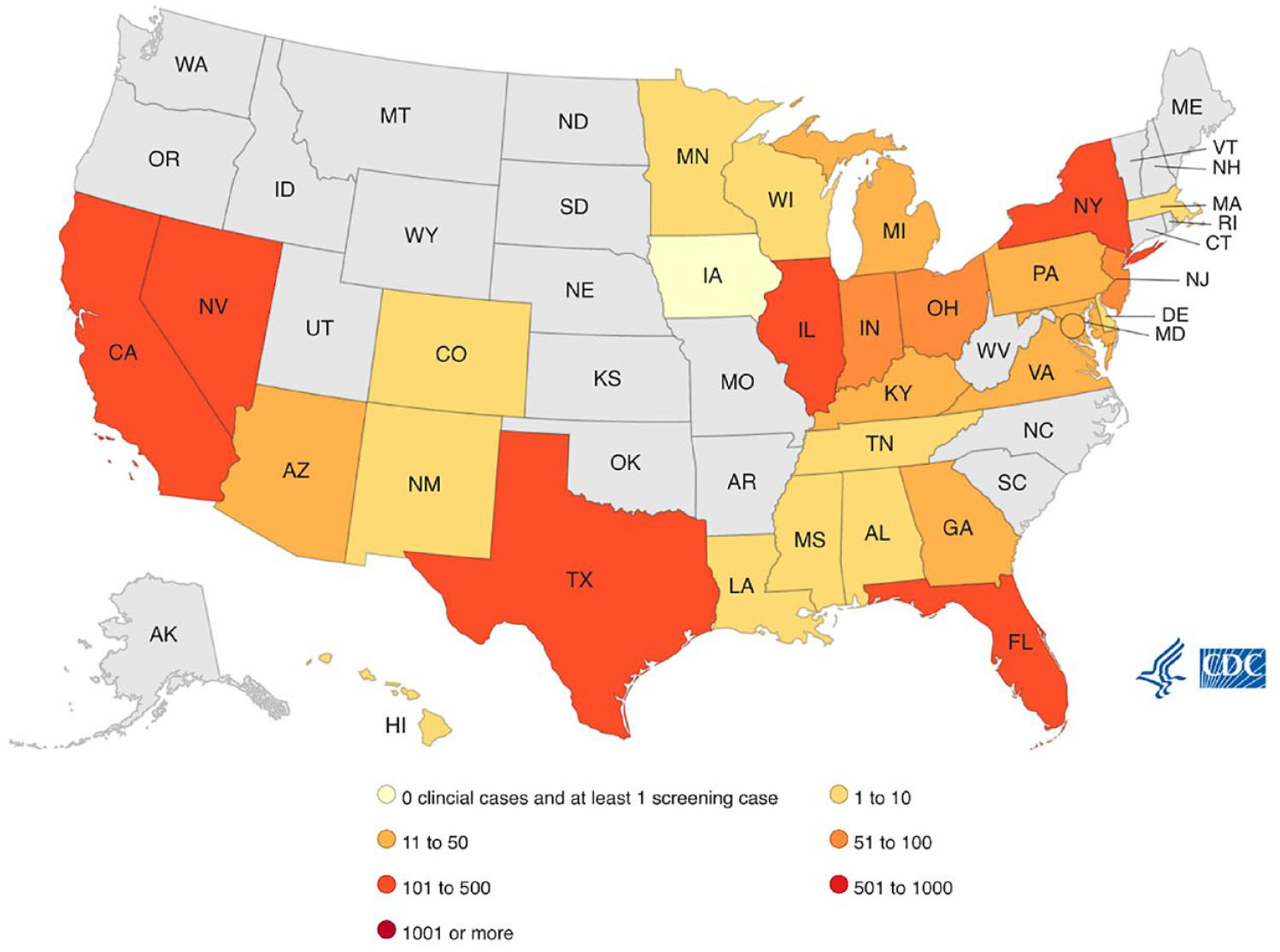
Reported clinical cases of C. auris by state in 2022.
It is worthwhile to consider the ‘resistance iceberg’: for every known C. auris-colonized resident identified through clinical culture testing, there may be many more unknown C. auris-colonized residents.49,50 For example, in Chicago, the public health department performed a point prevalence survey of the ventilator unit of a skilled nursing facility after one resident was identified as C. auris colonized; an additional 28 residents were subsequently identified as colonized with C. auris. 31 Active surveillance for C. auris among skilled nursing facility residents requires access to a laboratory that can test for the organism. In the United States, collaboration with local public health departments can facilitate access to regional public health laboratories in the Antibiotic Resistance Laboratory Network. 51 Screening typically occurs via a composite swab from bilateral axillae and groin sites and may be targeted at skilled nursing facility residents at time of admission or as a part of an outbreak response (e.g., testing close contacts or testing an entire ward or facility). 52
Cleaning and disinfection
The environmental control of C. auris is challenging, as illustrated by a study performed in four long-term care facilities and one acute care hospital. 53 The investigators performed targeted cleaning of high-touch surfaces in the patient room occupied by patients with confirmed multidrug-resistant organisms including C. auris and demonstrated recolonization of C. auris within 4 h of cleaning on the overbed table, handrail of the bed, and remote control. Of note, C. auris contamination of surfaces outside of resident rooms was much less common (1 of 120 swabs positive), suggesting that environmental contamination is primarily within patient rooms and can be contained within rooms if proper hand hygiene and gown/glove precautions are followed by staff upon exit of the room. Contamination of surfaces can be prolonged and varies by surface type; laboratory studies have shown that C. auris can survive at least a week on dry steel, 54 and at least 2 weeks on plastic surfaces. 55
Not all routine healthcare environmental disinfectants are active against C. auris, and some products with C. albicans or fungicidal claims may not be effective. In particular, quaternary ammonia compounds that are commonly used in the healthcare setting are not effective in controlling C. auris.56,57 Commercially available products with claims of activity against C. auris are registered with the United States Environmental Protection Agency (EPA) (‘List P’; see Table 1). 58 This list should be consulted when establishing local guidelines on selection of antimicrobial products and applying the product for the correct contact time. Infection control recommendations for residents in shared rooms include maintaining a minimum of three feet of separation, use of privacy curtains and high-quality environmental cleaning. 59 A negative result from environmental sampling for C. auris does not confirm absence of this organism and is not recommended by the US Center for Disease Control and Prevention (CDC) other than specific scenarios in which it could be useful such as investigation of an outbreak.
Antimicrobial products with claims to eradicate C. auris, registered with the EPA 58 (accessed March 28, 2023). Note that there are several commercial products with the same active ingredients. Contact time is per label instruction of each product, which may differ depending on the formulation type or the product.

DDAC, Didecyldimethylammonium chloride; EPA, Environmental Protection Agency.
Implications on rehabilitation
Stringent cleaning, disinfection, and isolation requirements may significantly impact the capability to perform rehabilitation. Although literature is sparse on this subject, there have been reports of successful care in inpatient rehabilitation with patients with C. auris.60,61 In light of the risk of cross-contamination,6,39,62,63 physical therapy (PT) and occupational therapy (OT) were performed in the patient room. The report on inpatient rehabilitation experience in a large academic center located in New York, NY, illustrates a patient who was hospitalized in a two-bed patient room. In the patient room, the second bed was removed to repurpose the space for private PT/OT sessions. Dedicated PT/OT equipment was used for the patient, which was also stored in the aforementioned space. Additional resources required for the prevention of in-facility spread of C. auris, including dedicated environmental service, staff education, private therapy sessions, and blocking a patient bed, can pose a significant burden to patient care. 60 The impact of C. auris on cost, efficacy, or infection prevention associated with rehabilitation in skilled nursing facilities is not well described. Strategies adopted by inpatient rehabilitation facilities for prevention of C. auris cross-transmission during PT and OT sessions could be adapted for skilled nursing facilities.60,61
Transmission-based precautions
Because C. auris spreads from person to person via touch, transmission-based precautions such as Contact Precautions or Enhanced Barrier Precautions are strategies to control C. auris spread. The US CDC currently recommends isolation (Contact Precautions or Enhanced Barrier Precautions) in taking care of residents with C. auris for the duration of the residents stay at a long-term care facility. 59 Contact Precautions involve the use of gown and glove at the time of room entry for any type of in-room activity, and residents given dedicated equipment and placed in a private room (or cohorted in multi-bed rooms). Residents on Contact Precautions are restricted from leaving their rooms, except for medically necessary care, and are not allowed to participate in group activities.59,64 The use of Enhanced Barrier Precautions, in which gown and glove are used during high-contact activities such as dressing, bathing, wound care, or changing linens, is another option for C. auris control that is resident-centered and a more practical option in the skilled nursing facility setting because residents are not restricted exclusively to their rooms and can participate in group activities. 65
In addition to implementing isolation protocols, a multifaceted approach to adopt a combination of several interventions may be required to maximize effectiveness of infection control. On an individual level, each practitioner and staff member should understand the implication of colonization and contamination by C. auris in patient care, practice correct use of transmission-based precautions and abide strongly by institutional infection control guidelines to limit nosocomial spread.
It is also important to understand the implications of resident isolation for other infectious diseases on the incidence of C. auris. An increase in C. auris cases in Orange County, California during 2020 and 2021 was reported among long-term acute care and skilled nursing facilities, and it was felt that these were attributable to alterations in infection control practices amid the COVID-19 pandemic such as crisis capacity strategies involving re-use or extended use of PPE, improper PPE use (double gloving), cohorting based on COVID-19 status alone, and inadequate environmental cleaning. 66
Visitors (including family members and personal aides) to the skilled nursing facility residents should abide by Contact Precautions or Enhanced Barrier Precautions at all times given the likelihood of them providing assistance with activities of daily living such as bathing or dressing. The risk of C. auris transmission to family members is generally believed to be low, with healthcare contact posing the highest risk of acquisition. Lastly, clear lines of communication must be in place while accepting patients or transferring residents with a C. auris diagnosis. This is vital to curb the chain of inter facility transmission (acute care facility to long-term care facility or vice versa, and long-term care facility to long-term care facility).
Diagnosis and treatment
Diagnosis
Use of traditional phenotypic methods for yeast identification, such as VITEK-2 YST, API 20C, BD Phoenix yeast identification system, and Microscan, can lead to misidentification of C. auris as erroneous species such as C. haemulonii or C. parapsilosis. 5 There are now a variety of advanced testing platforms that can accurately identify C. auris from different sample types including matrix-assisted laser desorption/ionization time of flight and real-time-polymerase chain reaction.67,68 These newer diagnostics have sensitivities and specificities for C. auris reported to approach nearly 100%. 67 However, many community hospitals and laboratories are not equipped with these advanced tests due to their high costs. In such settings, the use of differential and selective growth media has been described in the literature, which can be used in resource-limited settings before sending the specimen to a reference laboratory for confirmatory testing. 67 Differential media, which include CHROMagar Candida Plus and CandiSelect, allow for the growth of multiple fungal species with distinctive colony coloration. C. auris grows as white to cream colonies on CHROMagar Candida Plus supplemented with Pal’s medium. 69 Selective media, such as Selective Auris Medium, are able to preferentially grow C. auris over other Candida species, with sensitivities and specificities reported to be 100%. 70 We encourage providers in skilled nursing facilities to contact their local laboratory to determine the available testing options for identifying C. auris. Furthermore, staff education on C. auris diagnostic techniques is critical at this point in time as the risk posed by this organism continues to escalate. 71 Long-term care facilities in the United States are required by the Centers for Medicare & Medicaid Services to have a dedicated, on-site, trained infection preventionist (IP). 72 IPs at long-term care facilities typically coordinate diagnostic testing and reporting with public health authorities per federal and state regulations.
Symptomatic disease and management
Due to the high mortality rates associated with invasive disease, early consideration of potential C. auris infection is important. Bloodstream infections, otomastoiditis, skin and wound infections, device and catheter infections, urinary tract infections, and central nervous system infections are well documented in the literature.3,73–77 Symptomatic disease due to C. auris can manifest with or without constitutional symptoms, and clinical signs can vary based on the affected organ system(s) and/or device(s). There is no distinctive feature of C. auris infection given its ability to infect various tissues.73,78,79 Given this, appropriate collection of fungal cultures from the affected site (blood, urine, ear discharge, etc.) is important to establish a definitive diagnosis. Isolation of C. auris at the site of symptoms (especially if this site is sterile), combined with clinical interpretation of a patient’s signs and symptoms, helps with differentiation between symptomatic infection and asymptomatic colonization). 73 The US CDC highly recommends an infectious disease consultation while managing C. auris. 80
In the United States, 85% of C. auris isolates are resistant to azoles, 33% to amphotericin B, and 1% to echinocandins. 81 In vitro antifungal susceptibility to micafungin at low concentrations across multiple strains of C. auris has been demonstrated in literature. 82 Thus, echinocandins (e.g., micafungin, caspofungin, or anidulafungin) are the empiric treatment of choice for invasive C. auris infections. For certain infections, liposomal amphotericin B is preferred, such as when C. auris is isolated from the cerebrospinal fluid and reliable concentrations of echinocandins cannot be attained in that space. 83
One of the difficulties that skilled nursing facilities face is the treatment of systemic infections due to C. auris. Echinocandins are only available in IV formulations due to large molecular weights causing poor oral bioavailabilities, 84 which may add burden to nursing staff in skilled nursing facilities related to the placement and management of IV access. From a practical perspective, development of a new generation of echinocandins with a less frequent dosing schedule (e.g., rezafungin with once weekly dosing schedule)85,86 is encouraging, as it may provide an easier means to manage C. auris infection in the skilled nursing facility setting.
New classes of antifungals are also in development. For instance, ibrexafungerp, a first-in-class triterpenoid antifungal, which works similarly to echinocandins by inhibiting (1 → 3)-β-
Asymptomatic colonization and management
Many Candida species are considered part of commensal organisms in the human gastrointestinal tract and other body sites such as skin and nails.91–93 Notably, C. auris appears to have a propensity to colonize on the skin. 91 One study of nursing home residents investigated the relative sensitivity of screening one or more body sites for C. auris among nursing home residents in Chicago, where Clade IV is predominant. 94 Screening the nares alone resulted in the highest sensitivity (53%); the most-sensitive two-site combination was nares with palm/fingertips (76%), and a minimum of six body sites (nares, palm/fingertips, toe webs, perianal skin, inguinal crease, and axilla) was needed to identify all colonized residents, suggesting a wide degree of variation of body site colonization. In practice, the most commonly recommended approach to asymptomatic screening uses a composite swab of a resident’s bilateral axillary and inguinal creases, sometimes with the addition of anterior nares.52,95 There is no consensus on decolonization protocol at this time. High-concentration chlorhexidine gluconate bathing (⩾625 μg/mL) was shown to be effective in reducing the odds ratio of detecting C. auris on the skin. 94 In practice, even if chlorhexidine gluconate cannot completely eradicate C. auris from the skin, it may reduce skin burden and thereby prevent invasive disease. However, it is important to note that C. auris outbreaks have been observed in skilled nursing facilities routinely using chlorhexidine bathing. 31
Conclusions
C. auris is a multidrug-resistant fungus that is a threat to healthcare settings worldwide. 6 Invasive infection from C. auris is associated with high mortality for nursing home residents, with few available options for treatment.10,81 Skilled nursing facilities that care for residents requiring chronic mechanical ventilation or other highly dependent care are particularly vulnerable to C. auris outbreaks. As skilled nursing facilities evolve to care for a sicker resident population, C. auris will be an emerging threat that will demand higher attention to infection prevention and greater collaboration between healthcare facilities and public health.