
Abstract
Introduction:
As at 2019, Nigeria was ranked the fourth highest HIV burden in the world. There is varied geographical HIV prevalence in Nigeria. The progress made is inequitable across geographical locations and sub-populations (18). Benue state has the second highest HIV prevalence in Nigeria. In 2018, about 35,623 people living with HIV (PLHIV) were yet to commence antiretroviral treatment (ART) in the state, accounting for an estimated ART coverage gap of 11% out of the combined gap of 320,921 in the country. To close this gap, the Benue ART surge (BAS) was implemented. The aim of this study was to describe the BAS strategic approaches and demonstrate progress in expanding ART access for PLHIV in Benue State, Nigeria.
Methods:
BAS was implemented in 252 health facilities from May 2019 to September 2021. Data were collected and reported using an Excel-based dashboard and electronic medical records. The trend of HIV case identification, ART initiation, viral load suppression rate, and rate of interruption in treatment during the BAS period was then described and analyzed.
Results:
Out of 893,462 clients reached, 6.7% (n = 60,297) were diagnosed with HIV and 99.8% (n = 60,236) were initiated on ART. HIV case identification per month increased by 467% from 650 at baseline to a peak of 3685 in August 2020, and then declined by 35% to 2380 in September 2021. All new HIV-infected patients (100%) were linked to ART. Viral load testing coverage and viral load suppression rate increased from 30% (43,185/126,004) and 84% (n = 36,165/43,185) at baseline to 95% (n = 193,890/204,095) and 96% (185,785/193,890), respectively.
Conclusion:
Implementation of the BAS improved access to comprehensive HIV services in Benue State. The increase in HIV case identification and ART initiation significantly reduced the HIV treatment gap in the state. To fast track the attainment of UNAIDS 95-95-95 goals, lessons learnt from the BAS should be adapted and scaled up in the national HIV program in Nigeria.
Introduction
As at 2019, Nigeria was ranked the fourth highest HIV burden in the world with an estimated 1.9 million infected persons, prevalence of 1.4% and incidence of 8 per 10,000 people. 1 There is varied geographical prevalence in Nigeria. In 2020, 1.5 million (88%) were receiving antiretroviral treatment (ART). 2 The Joint United Nations Program on AIDS/HIV (UNAIDS) set the 90-90-90 targets in 2014 for HIV epidemic control by 2020: 90% people living with HIV (PLHIV) are aware of their HIV status; of these, 90% are receiving sustained ART; and of these, 90% have viral load suppression. 3 To determine progress toward the set targets and to exhaustively describe the distinctive feature, Nigeria conducted the 2018 Nigeria AIDS Indicator and Impact Survey (NAIIS), estimating the national HIV prevalence at 1.4%. Nigeria’s progress toward the UNAIDS 90-90-90 targets was 47-96-81, with approximately 1 million HIV-infected individuals who are yet to be diagnosed. The survey showed prevalence, as well as the estimated total numbers of PLHIV and PLHIV on ART, varied widely by state).4,5 This variability implied that policymakers needed to implement HIV program strategies tailored to states in order to control HIV epidemic in Nigeria.
The US President’s Emergency Plan for AIDS Relief (PEPFAR) supports the Government of Nigeria in providing HIV services, including technical assistance and direct funding of implementing partners, launched the ART Surge in April 2019, intended to rapidly increase the proportion of PLHIV identified and linked to treatment. To help close the state ART gap, staff from APIN Public Health Initiatives (APIN) and its funder United States Centers for Disease Control and Prevention (CDC), partnered with the state Ministry of Health to implement this scale-up, termed the Benue State ART Surge (BAS) through intensified case finding, linking and continuity of identified cases in treatment, in order to achieve viral suppression. The magnitude of this proposed scale-up required that novel interventions were deployed to achieve this objective. We describe the strategic approaches aimed at achieving treatment saturation for PLHIV during the BAS implementation, as well as demonstrate progress in expanding ART access for PLHIV in Benue State from May 2019 to September 2021.
Methods
Study setting
Benue State has the second highest prevalence and burden of HIV in Nigeria. It has a statewide HIV prevalence of 4.9% with an estimated burden of 184,745 PLHIV. It is one of the seven states that account for 50% of estimated PLHIV, with ART coverage gap of 35,623 out of the combined gap of 320,921 (11%). 4
Description of the BAS
In the context of HIV/AIDS, epidemic control is defined as the critical point reached where the total of new HIV infections falls below mortality from all causes among PLHIV, with both indices declining. 6 UNAIDS declared a 95-95-95 target in December 2020 for year 2025. That entails that 95% of PLHIV know their HIV status, 95% of those diagnosed with HIV receive sustained antiretroviral therapy and 95% of those on ART achieve viral suppression. 7 The implementation strategy of the Benue ART surge was anchored on the Incident Command System (ICS) and State Surge Consortium. The ICS is a flexible stable model for responding to large-scale events as the chain-of-command helps communication and implementation. 8 There was a structured command system from CDC to APIN team led by incident commanders, and other focal persons. The ICS was supported by a decentralized operational structure with state and local government area (LGA) team approach to make programmatic decisions that are data-driven, real-time, tailored to local context; and facilitate a bottom-top approach to program management. BAS consortium was formed and launched on 25 February 2020 to collaborate between State Government, PEPFAR, community-based organizations (CBOs), and the private sector to galvanize support to achieve the targets. The surge consortium was to ensure enabling environment, ownership, and sustainability of HIV program in the state, elimination of ART-associated user fees so as to improve access, provide platforms for sourcing additional support for the surge, such as commodities/rapid test kits, garner support for expanded case finding and support public information dissemination and awareness creation.
Strategic approaches of the Benue ART surge
Strong stakeholder engagement
A state HIV consortium was formed for the rapid scale up of ART, which required stakeholder participation, coordination, and resource mobilization and alignment.
Coronavirus disease 2019 adaptation strategies
The coronavirus disease 2019 (COVID-19) epidemic in Nigeria threatened to disrupt the progress of the Benue ART Surge. To overcome service disruption due to COVID-19, a series of adapted strategies for all PLHIV populations were implemented in February–September 2020.9,10
Small area estimation
This was used to identify LGA-level ART gaps for targeted HIV intervention. Small area estimation (SAE) is a model-based estimation that uses pre-existing survey data, such as NAIIS and program data. 11 SAE helped prioritize LGA-level testing and resource allocation.
A three-tiered facility management approach
A volume analysis and tiering of facilities providing HIV services was conducted in order to map facilities to enhance optimal performance in case finding. Tier 1 and 2 sites constituted 80% of client load with suboptimal and optimal performance, respectively, in terms of weekly case-finding targets. All the other facilities in the remainder of 20% formed tier 3.
Facility-based testing
To improve case finding, the HIV risk stratification tool (HRST) was deployed across different testing streams within the facility to assess HIV infection risk and to increase the likelihood of identifying PLHIV.
Expansion of targeted community-based testing
Dedicated community teams were deployed to conduct HIV education, screening, counseling, and testing in the communities because optimization of HIV testing in the facility could not solely deliver on the recalibrated case-finding targets. The testers and linkage coordinators were also motivated by applicable performance-based incentives (PBIs) to enhance their outputs.
Scale-up comprehensive key population program
Key population (KP) friendly CBOs were engaged to provide population-sensitive community testing services using high yielding and efficient HIV testing modalities.
Third-party strategy of case finding
This was in collaboration between private clinics, laboratories, delivery homes, pharmacy, and patent medicine vendors for case identification and linkage.
Continuity of treatment
The strategy focused on readiness to start treatment and employed a multidisciplinary approach to treatment retention. Case management was instituted to ensure close follow-up within the first 3 months of ART, which is critical to long-term continuity of treatment (CoT). This made use of the 90-day adherence calendar. Other strategies included pre-emptive measures to reduce missed clinic appointments (patient education, structured appointment system, appointment reminder, scale up of differentiated service delivery models and patient satisfaction surveys),12,13 improved identification of missed appointments, client tracking after missed appointment and documentation of tracking outcomes, peer support and champions to support adherence counseling and linkage to support groups and leveraging technology for the delivery of client centric care.
Viral load optimization
Viral load was optimized in consonance with achieving at least 95% viral suppression in all patients on ART as the end point of the surge.
Enhanced program management
Project Extension for Community Healthcare Outcomes (ECHO) is a collaborative model of medical education and care management that is operated via remote, low-bandwidth technology to share and disseminate best practices among colleagues. 14 Project ECHO and peer-to-peer learning ensured continuous quality improvement of service delivery. ECHO was deployed to all tier 1 and 2 sites. The Benue surge team conducted in person and virtual visits to selected treatment sites every month. Quality improvement approaches were used to problem-solving during such visits. 12
Site transition
In line with the national treatment program alignment plan toward improved resources/program efficiencies and maximum impact in the national HIV program, the Global Fund implementing partner in Benue, transited HIV service delivery with number of current PLHIV receiving ART of 13,475 to APIN by January 1, 2021.
Enhanced program monitoring
APIN successfully set up structures and processes for implementing daily program monitoring in Benue state. The system also entailed strengthening real-time data capture into the electronic medical records (EMRs) with daily national data repository (NDR) data uploads. Multimonth Dispensing (MMD) is a programmatic strategy of enabling stable patients pick up drugs for up to dose of 3 months and above to reduce frequency of visits to health facilities.
Study design
This is a retrospective, descriptive, analysis of program data for PLHIV in Benue State from May 2019 to September 2021.
Study variables/outcome
In this study, the variables of interest include HIV positivity yield refers to the proportion of patients who tested positive among those that were tested for HIV. Linkage to ART is defined as the proportion of newly identified HIV-positive patients that were initiated on ART. Treatment current (TX_CURR) is the number of adults and children currently receiving ART. Interruption in treatment (IIT) is defined as the number of ART patients (who were on ART at the beginning of the quarterly reporting period or initiated treatment during the reporting period) and then had no clinical contact since their last expected contact. Viral load coverage (TX_PVLS (D) is the percentage of viral load eligible ART patients with a viral load test result, while viral load suppression (TX_PVLS (N) is the percentage of ART patients with a suppressed Viral Load (VL) result (<1000 copies/ml) within the past 12 months.
Data collection process
Data on the number of clients tested for HIV, diagnosed with HIV, and commenced on ART into the surge reporting dashboard were collected. At the end of every week, the reports were validated and extensively triangulated with all source documents. This validated report is then collated from all the 252 supported facilities using a mobile data collation form. This helped to improve the timeliness of reporting and reduced transcription errors. Data was aggregated at the state level for weekly reporting to the CDC using the excel-based dashboard. The weekly surge indicators captured in paper-based Data Capturing Tools (DCTs), EMR outputs and the NDR data were triangulated for concurrence. This was further analyzed using Excel-based analytics tool to monitor performance and compare the numbers of patients who were tested, newly identified HIV positive clients and initiated on ART during the ART surge implementation.
Data quality check
The Benue State Surge team data leads reviewed and submitted daily facility and community data for error checks and made requisite corrections in consultation with site staff. A full-scale community testing stream was activated in November 2019. Community testing efforts were tracked in a separate Excel-based tool. The Excel tool provides a weekly and monthly display of aggregate data to show progress from November 2019 to September 2021. The Benue surge team tracked numbers of individuals screened for HIV risk using the HRST, tests done, positive individuals found, and treatment initiations on a daily basis.
Data analysis procedures
All variables were investigated using univariate analysis to determine the frequency, distribution, tables, and charts. Independent sample t-test was employed to compare the number of HIV-positive cases and the number linked to ART between the first year (May 19–April 20) of implementation and the second year (May 20–April 21). All analysis was conducted using Microsoft Excel and STATA version 16 statistical package and statistical significance was established at 5%.
Ethics
APIN Public Health Initiatives is a leading non-governmental organization (NGO) that focuses on the provision of prevention, care and treatment services to patients with diseases of public health significance such as HIV/AIDS, Tuberculosis and Malaria. APIN also provides technical assistance to relevant government agencies to strengthen the delivery of Reproductive Health, Maternal, Newborn and Child Health, Laboratory services. The vision is to become the leading Public Health NGO committed to disease burden reduction and impact mitigation in Nigeria and Africa. While the mission is to provide cutting-edge, innovative and sustainable approaches to address diseases of public health importance through effective program management, service delivery, capacity building, research, strategic information & advocacy in partnership with other stakeholders.
The APIN Public Health Initiatives Institutional Review Board (IRB) reviewed the study and was it determined to be exempt as non-research, public health program activity. This study required no direct contact with human participants and only utilized de-identified pooled program data that formed part of standard of care; thus no informed consent was required. 15 This is reinforced by the International Ethical Guidelines for Health-Related Research Involving Humans on waiving informed consent. A research ethics committee may waive informed consent if it is convinced that the research would not be feasible or practicable to carry out without the waiver, the research has important social value, and the research poses no more than minimal risks to participants. 5
Results
HIV testing, positivity rate, initiation of ART
Over the 30 months of the Benue ART surge period from May 2019 to September 2021. 893,462 clients were reached and tested for HIV in Benue State, Nigeria. Of these, 6.7% (n = 60,297) were diagnosed with HIV and 99.8% (n = 60,236) were enrolled and initiated on ART.
The absolute number of newly diagnosed HIV patients increased by 467% from 650 in 2019 to a peak of 3685 in August 2020, and then declined by 35% to 2380 in 2021 (Figure 1). Figure 1 highlighted weekly trend in performance with call out explaining series of events associated with spikes and dips. Of the 60,297 new HIV cases identified during the BAS intervention, 45% (n = 27,309) of them were offered HIV Testing Services (HTS) and tested within the community (Figure 2; Table 1).

The trend of HIV case identification with 10-week medians and key milestones during Benue ART surge between 2019 and 2021 in Benue State, Nigeria. ART, antiretroviral treatment.

HIV positively yield and linkage to antiretroviral treatment between May 2019 and September 2021 during Benue ART Surge in Benue State, Nigeria. ART, antiretroviral treatment.
Statistical analysis.

ART, antiretroviral treatment; CI, confidence interval; HIV, human immunodeficiency virus.
The above table showed a statistically significant increase (p < 0.05) in the number of HIV-positive cases and the number linked to ART between the first year (May 19–April 20) of implementation and the second year (May 20–April 21).
Linkage to treatment
All diagnosed HIV patients were linked to ART during the ART surge period. Figure 3 shows the number of PLHIV diagnosed, HIV positivity yield, PLHIV initiated on ART and linkage to ART per month between May 2019 and September 2021.

Number of PLHIV diagnosed disaggregated by facility-based and community-based HIV testing between May 2019 and September 2021 during Benue ART Surge in Benue State, Nigeria. ART, antiretroviral treatment; PLHIV, people living with HIV.
Figure 4 shows the trend of patients active on ART per quarter. At baseline in Q2 of 2019, a total of 136,606 patients were active on ART (TX-CURR) based on the 28-day IIT definition. From Q2 of fiscal year 19 to Q4 of fiscal year 21, 60,236 new HIV-infected patients were initiated on ART and by the end of the quarter, 219,910 were active on ART. As of September 31, 2021, 98.7% (n = 219,910/222,689) were retained on ART.

Treatment growth analysis showing increasing number of adults and children current on ART by quarter between May 2019 and September 2021 during Benue ART surge in Benue State, Nigeria. ART, antiretroviral treatment.
Treatment interruption
Figure 5 below shows the proportion of patients in the Benue state HIV Surge Program who interrupted their treatment per quarter from Q1 of fiscal year 19 to Q4 of fiscal year 21. Statistical Analysis shows a decreasing IIT to improve retention (CoT). The Mann-Kendall test showed a statistically significant decrease in IIT rate from FY20Q1 to FY21Q4 (ρ = −0.643; p value = 0.026)
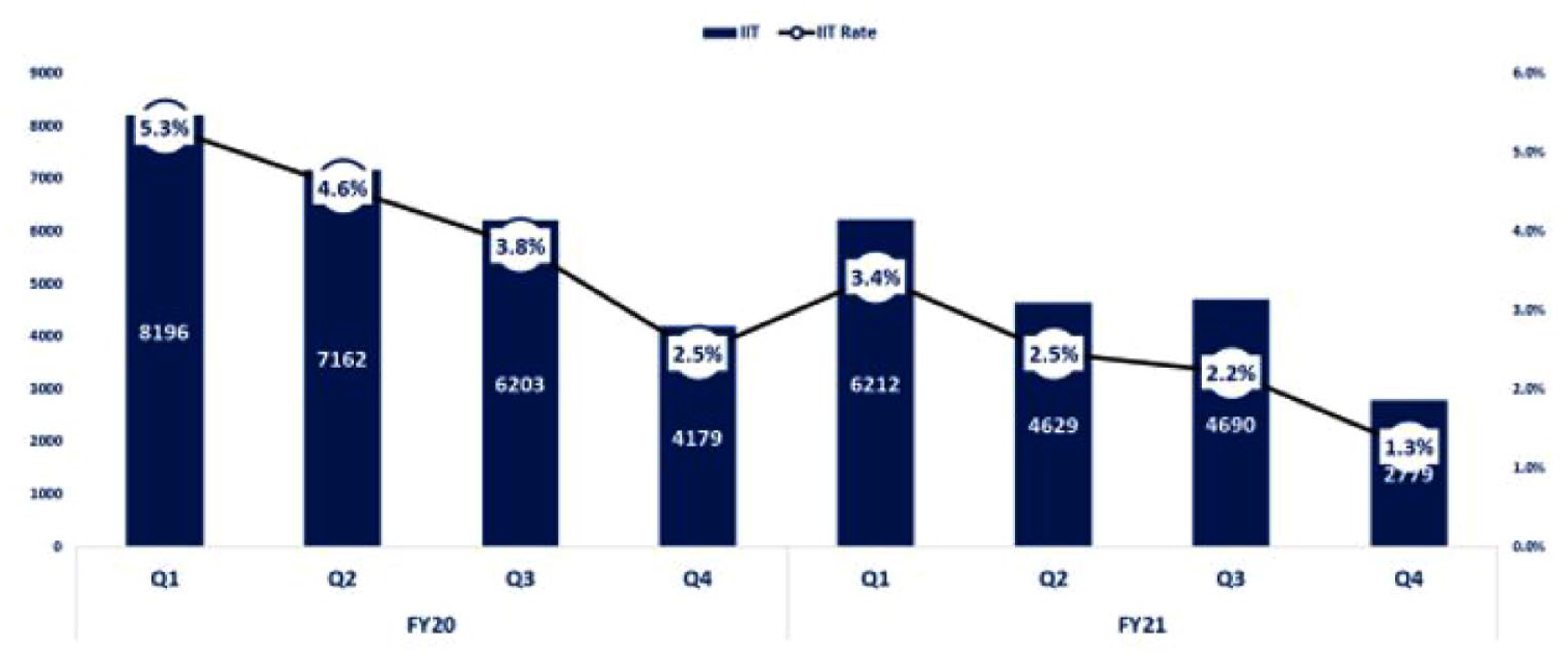
Quarterly trend of interruption in treatment (IIT) by quarter between January 2020 and September 2021 during Benue ART Surge in Benue state, Nigeria. ART, antiretroviral treatment.
Figure 6 shows MMD uptake relative to TX_CURR on a quarterly basis. The rate of IIT declined from 5.3% (n = 8196) at baseline in fiscal year 2019 Q1 to 1.3% (n = 2779) in Q4 of fiscal year 2021.

Multimonth dispensing trend by quarter between May 2019 and September 2021 during Benue ART Surge in Benue state, Nigeria. ART, antiretroviral treatment;
Figure 7 shows the trend of viral load coverage and suppression during the ART surge intervention in Benue. As of 31 September 2021, viral load coverage and suppression were 95% and 96%, respectively.

Viral load coverage and suppression between May 2019 and September 2021 during Benue ART surge in Benue state, Nigeria. ART, antiretroviral treatment;
The percentage of eligible patients with a viral load test (Viral load coverage) increased from 30% (n = 43,185/126,004) at the start of ART surge program in quarter 2 of 2019 to 95% (n = 193,890/204,095) at the end of quarter 4 of 2021. Approximately 84% (n = 36,165/43,185) and 96% (n = 185,785/193,890) of patients had a suppressed viral load test at baseline (2019-Q2) and Q4 of 2021, respectively. Using Mann–Kendall test of trend, there was a statistically significant increase in viral load coverage (ρ = 0.871; p value = 0.000) and suppression rate (ρ = 0.925; p value = 0.000) for the period under consideration
Kindly note that ρ is a coefficient of correlation testing for the linear relationship over time.
Discussion
The UNAIDS 95-95-95 programmatic cascade target was attained, which has placed Benue state on the brink of HIV epidemic control due to the success of BAS implementation. The Benue ART Surge overarching objective of diagnosing and linking the estimated gap to treatment was successfully achieved during the implementation period. All newly diagnosed HIV patients were linked to ART during the implementation of Benue ART surge. Facilitating optimal linkage to ART is the PBI for volunteer HIV counselor testers in the health facility and the community. This approach optimized the performance of testers by rewarding monthly achievement of testing and treatment targets.
CoT during the Benue ART surge was optimal. The rates of IIT steadily declined per quarter during the ART surge period. The downward trend of IIT suggests that the majority of patients adhered to their ART refill and clinic appointment. The improvement in CoT can be attributed to the client-centered nature of the ART surge strategies. When interventions are designed to meet the individual health needs of patients that are enrolled in the ART program, more patients will be encouraged to adhere to drug refill and clinical consultation appointments. 16 Differentiated service delivery models such as the community-based and facility-based ART models were implemented to minimize attrition. These models contributed to improve CoT in the Benue ART surge program. Established patients on ART had their ART refill through Community ART pharmacy, community ART refill venues, and one-stop shop clinics for KP in the program. This finding is similar to Differentiated Service Delivery (DSD) model implementation in different settings in Nigeria.13,17
The improvement in viral load coverage and suppression over time indicate the effect of Benue ART surge strategies on VL optimization. The use of viral load champions was a novel strategy that enhanced the demand and supply side of viral optimization. The viral load champions worked in synergy with other healthcare workers to identify and address gaps in the uptake of viral load tests and processing of viral load results. The use of nurse adherence counselor to provide tailored adherence counseling contributed to improved suppression rates. These VL-targeted strategies resulted in improved viral load coverage and suppression in the program.
The Benue ART surge outlines the strategies and results to close gaps in HIV case finding, linkage to ART, CoT, viral load coverage and suppression. Small Area Estimation, expansion of community-based HIV testing and enhanced program monitoring were essentially the most effective of the strategies deployed. The overall success of the Benue ART surge can be attributed to strong leadership, strategic coordination of resources, and accountability to implement context-specific and appropriate interventions. The incident command structure increased collaboration among stakeholders to foster joint decision-making and rapid dissemination of information and adaptation of strategies that improved HIV testing and treatment outcomes among PLHIV. 17 This type of collaboration should be encouraged in the national and sub-national HIV programs to ensure ownership and sustainability.
The upward trend of new PLHIV initiating ART per week indicates the efficiency of the ART surge strategies to improve HIV case finding and linkage to ART. At the onset of the ART surge implementation, the number of patients testing HIV positive increased marginally per week. However, with the provision of the community HIV Testing Services (HTS), there was a significant increase in the of HIV cases Community HIV testing contributed 45% to the total number of PLHIV diagnosed with HIV in the state. These findings about HIV case finding and linkage are comparable to other studies that evaluated ART surge strategies in other states in Nigeria17,18 and in Zambia. 19 In these studies, implementation of ART surge strategies was associated with an increase in HIV case identification and linkage to ART.17–19 HIV testing positivity rates was maintained between 4% and 11% during the study period. This finding underlines the HIV testing efficiency. The prioritization of LGA for HIV testing and resource allocation using SAE, differentiated community HIV testing strategies, and the use of HRST can explain the increase in testing efficiency during the surge implementation. All potential patients for HTS were screened for testing eligibility using the HRST. A study on HRST, index testing, and other strategies showed that the use of HRST increased the efficiency of HTS and increased HIV case detection in many states in Nigeria. 20 Community HIV testing can complement facility-based HIV testing services.
The COVID-19 pandemic presented the HIV program with challenges of low HIV case finding and CoT. To address these challenges, the program adapted the ART surge strategies by intensifying community testing and scaling MMD of ART to new and established PLHIV from 1 to 3 months and 3 to 6 month, respectively. These strategies improved CoT by reducing the frequency of face-to-face interaction and waiting time in the health facilities and costs of transportation to the health facilities for drug refills. Other supporting strategies that improved CoT are pre-emptive strategies that prevented missed appointments and IIT (pre-appointment reminder/check-in calls/SMS, virtual client engagement/support, peer support
Findings from this analysis come from real-life setting in a low-resourced setting and it can inform the design, planning, and implementation of the vertical HIV program in Nigeria. The limitations of this study include observational bias that is inherent in non-experimental research designs as well as an inability to directly attribute interventions to the observed outcomes. Attrition on ART should be interpreted with caution because data were aggregated at the state level and the proxy indicator, percentage of IIT, discounted patients with IIT from the expected number of patients on ART per quarter. We minimized possible duplication in the documentation of ART enrollment and initiation by implementing Patient Biometrics Solutions (PBS) among all patients who consented to have their fingerprints captured and conducted de-duplication at the NDR level. To strengthen systems for data quality, APIN conducted (PBS) to ensure duplicates are eliminated from both existing and new clients. This PBS captures the fingerprints of clients in order to identify and expunge duplicates. For new clients, PBS was mandated as part of client enrollment process to forestall recycling of clients. Invariably this has improved the quality assurance of the surge Epidemic Control.
In conclusion, our analysis revealed improved HIV testing and treatment outcomes (HIV case detection, ART initiation, CoT, and viral load suppression) during the implementation of Benue ART surge program. To fast track the attainment of UNAIDS 95-95-95 goals, lessons learnt during the Benue ART surge period should be adapted and scaled up in settings with similar context in Nigeria and other sub-Saharan African countries.