
Abstract
Visceral leishmaniasis carries a significant burden of disease in the Americas with up to 7000 cases reported annually. There are several reports of autochthonous visceral leishmaniasis cases in the Caribbean, including the Dominican Republic, Guadalupe, Martinique, and Trinidad and Tobago. However, we lack recent clinical description and epidemiologic data of visceral leishmaniasis in other islands in the Caribbean. Herein, we describe an autochthonous case of visceral leishmaniasis in the Caribbean Island of Margarita in Venezuela. This index case of visceral leishmaniasis highlights the need for further regional surveillance efforts to identify animal reservoirs and to monitor the occurrence of further clinical cases. Additionally, there is an urgent need for implementing vector control strategies.
Introduction
Leishmaniasis is an infectious disease caused by Leishmania parasites. It manifests clinically as cutaneous, mucocutaneous, or visceral (kala-azar) forms. The female sand fly of the genus Phlebotomus in the Old World and Lutzomyia in the New World are the vectors responsible for the transmission of this parasitic infection. 1
The World Health Organization (WHO) estimates the incidence of visceral leishmaniasis (VL) in 50,000–90,000 new cases worldwide. In 2018, most of the reported cases occurred in Brazil, China, Ethiopia, India, Iraq, Kenya, Nepal, Somalia, South Sudan, and Sudan. 2 The estimated annual VL incidence in the Americas is about 4500–6800 cases. 3 Brazil accounts for more than 95% of VL in Latin America, followed by Argentina, Paraguay, Colombia, and Venezuela. 2
In the Caribbean, there are several reports of autochthonous VL cases in the Dominican Republic, Guadalupe, Martinique, and Trinidad and Tobago. Most VL cases in Venezuela are reported among coastal towns. 4 In previous decades, the island of Margarita contributed to some of the overall number of cases in the region. The first report of VL in Margarita Island was in 1965. In 2003, there were reports of an average of 20 cases every year. 5 The last series of cases of VL in this island occurred in the municipality of Macanao in the Margarita island in 2015. Since that year, there has been an epidemiologic silence, with no reports of VL in the Island of Margarita. 6
VL often occurs in impoverished settings with insufficient access to healthcare, reduced supply of diagnostic infrastructure and tools, and limited availability of antiparasitic drugs.7,8 In many of these settings, VL carries a high mortality rate of up to 90% and, sadly, many cases commonly affect children.
Herein, we describe a recently diagnosed case of VL in a 15-year-old individual in the municipality of Macanao in the Margarita Island. This case reflects the suspected existence of animal reservoirs harboring the parasite and the ecological persistence of the vector. Therefore, public health authorities need to consider further surveillance efforts and vector control activities in this Caribbean island to prevent new cases.
Case description
A 15-year-old female from the Macanao municipality on the Margarita’s Island in Venezuela presented to the local health center with a 6-month history of intermittent fever predominantly occurring at night, malaise, 6 kg weight loss, arthralgias, loss of appetite, dizziness, and amenorrhea.
The patient lives in a rural area close to a landfill in a house built with cement ground, brick walls, and a metal roof without running water. She has one dog (unknown Leishmania infection status) and various turtles as pets. She has no history of traveling outside Venezuela. On physical examination, she was pale, with increased respiratory and heart rate, and fever of 39°C. Her weight was 49 kg (percentile 36% according to age and gender), height of 1.57 m (percentile 22.3% according to age and gender), and an abdominal circumference of 76 cm. She had cervical, axillary, and inguinal adenopathy. Cardiac and lung examination were normal. Abdominal examination revealed right upper quadrant tenderness to palpation, and hepatosplenomegaly (liver was palpable at right flank 9.5 cm from the midclavicular line, and spleen with Hackett’s system grade V) (Figure 1). Laboratory values on admission demonstrated pancytopenia (Table 1). Abdominal ultrasound and computed tomography confirmed the presence of hepatosplenomegaly. The initial clinical suspicion was that of a lymphoproliferative or myeloproliferative disorder. From an infectious disease perspective, the possibility of VL, a systemic mycosis, or tuberculosis were entertained.

(a) Distended abdomen with splenomegaly and (b) hepatomegaly.
Laboratory results on admission to the hospital.

BUN, blood ureic nitrogen.
We performed a bone marrow biopsy to rule out a hematologic malignancy but also to assess the possibility of histoplasmosis or VL by Giemsa staining. Cultures were negative, but the K-39 ELISA Leishmania titers were positive at 1:100. Immuno-phenotyping of bone marrow cells demonstrated a heterogeneous population of leukocytes with arrest and anomalies in the myeloid line’s antigenic maturation, and 1% of blasts compatible with a secondary myelodysplastic syndrome. Bone marrow biopsy showed hypocellularity, discrete collagen fibrosis, and increased macrophages with severe intracellular colonization of Leishmania donovani (Figure 2). Tuberculin skin testing and serologies for human immunodeficiency virus (HIV), syphilis, cytomegalovirus, and Epstein-Barr virus were all negative.
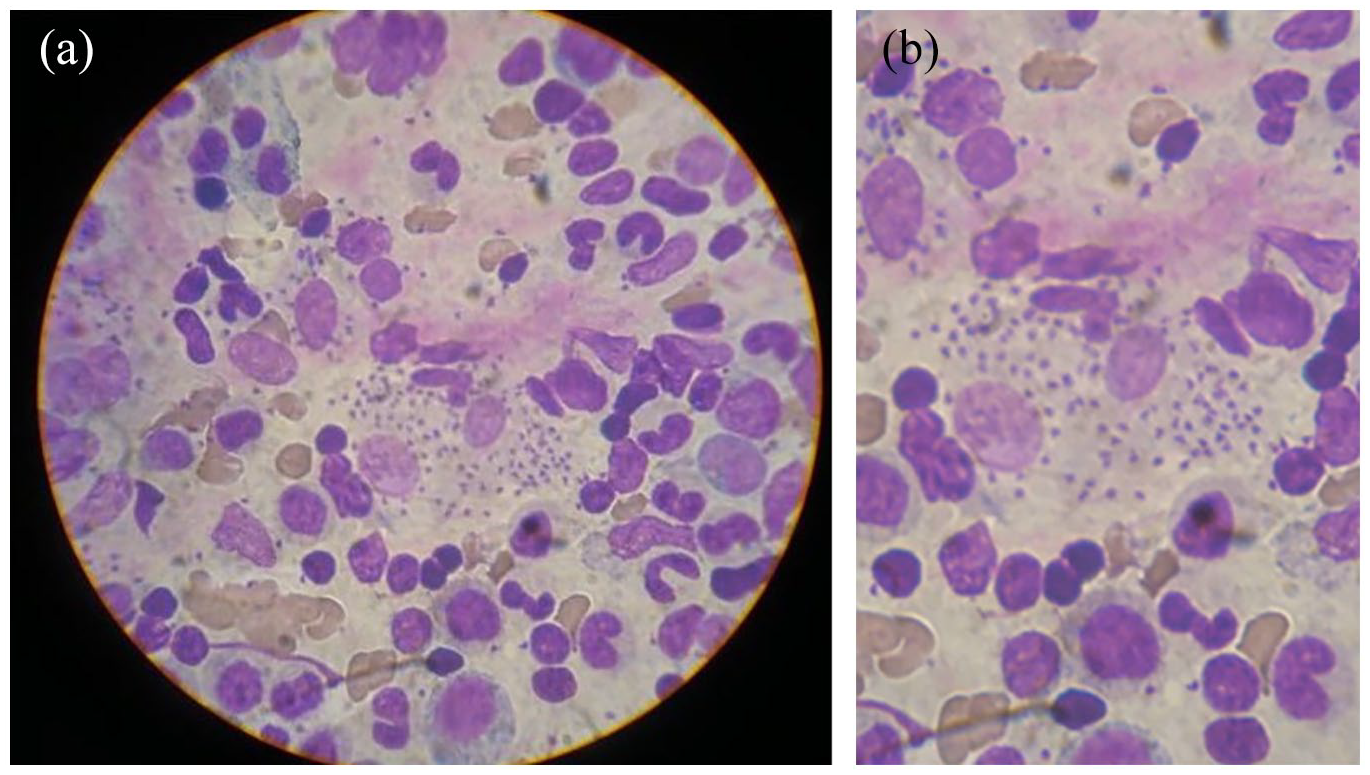
(a) Bone marrow aspirate evidencing macrophages with Leishmania amastigotes. (b) Increased magnification of the bone marrow aspirate demonstrating amastigotes.
The patient received treatment with meglumine antimoniate at 20 mg/kg/day for 30 days and tolerated this therapy without any significant side effects. The patient experienced significant improvement after completion of the treatment, becoming afebrile, and with increased appetite and gradual regression of her hepatosplenomegaly, and was discharged on stable clinical condition. Follow up laboratories after completion of antiparasitic therapy showed a hemoglobin of 10 g/dl, hematocrit of 29%, leukocytes of 5800 U/l, and platelets of 231,000 U/l.
Discussion
There is scarce data on the prevalence and incidence of VL in Latin America and the Caribbean. National surveillance programs and case notifications are largely incomplete with significant underreporting. 9 Previous epidemiological studies have revealed an incidence of three human cases per 100,000 population in Margarita Island (Nueva Sparta State). 10 Officials reported two associated deaths of human visceral leishmaniasis in the state in 1998. Serologic surveillance studies conducted in dogs from 1995 to 2000 have shown rates of Leishmania infection of 28.5% [confidence interval (CI): 26–31.1%] in the region. 10 Other surveys in the Margarita Island have identified seropositive rates of 21–33% among local dog populations. 11 This recent case of VL highlights the ongoing transmission risk of VL in humans on the island despite of years of surveillance quiescence.
In our case, the most likely form of transmission was vectorial, with the domestic dog acting as the potential reservoir. Unfortunately, we do not have any data on the animal available to confirm it as the infection source. In rural impoverished areas in Latin America and the Caribbean, the domestic dog is likely the main reservoir instead of some marsupials or sloths in sylvatic regions. Previous reports in the region have shown VL predominantly affecting men and children younger than 15 years. Untreated VL is associated with a case fatality rate of 90%. Establishing a diagnosis of VL remains a major challenge, particularly when medical professionals have a low index of clinical suspicion due to a paucity of cases. Affection of the reticuloendothelial system often leads to obtaining a bone marrow biopsy to rule out hematopoietic malignancies. Systemic invasive mycoses, disseminated tuberculosis, malaria, schistosomiasis, and VL should be considered among patients with fever, hepatosplenomegaly, and pancytopenia. 12
Several clinical factors may influence the range of clinical presentations. Coinfection with dengue can result in liver injury. Immunosuppression can lead to relapses after treatment with Amphotericin B. 13 Sometimes, the diagnosis of VL is delayed due to low clinical suspicion due to insufficient understanding of the epidemiology of transmission and the lack of obtaining a detailed travel history. 14 However, the possibility of VL should be entertained among patients presenting with the triad of fever, hepatosplenomegaly, and pancytopenia even in the absence of apparent epidemiologic risk factors because new autochthonous foci can develop.15–23 Hyperferritinemia and the hemophagocytic lymphohistiocytosis (HLH) can occasionally be the presenting clinical presentation of cases of VL in children or adults.15–18
VL is classified as a neglected tropical disease (NTD) by WHO because it generally affects poor populations and historically has not received as much attention as other diseases. Several poverty factors play a role in the ongoing transmission and burden the disease instills in the region. Like in other resource-constrained settings, our patient lived in a low-income neighborhood and enduring social factors that predispose children to develop VL in tropical and subtropical areas. A recent systematic review of environmental and socioeconomic factors revealed that distance to vegetation (e.g., bamboo), poor quality houses, low educational status, lack of access to essential services (sewage, water supply, garbage collection), having an infected dog, rainfall, and humidity climates, are all risk factors for VL. 2 Public health interventions to reduce the impact of VL require strengthening public health surveillance, vector control activities, and social improvements.3–8
Conclusions
VL is a reemerging NTD in the Island of Margarita in Venezuela. There is an urgent need to strengthen surveillance activities to identify animal reservoirs, case detection, and implement interventions including vector control and educational campaigns targeting local populations. Medical professionals must be informed of the risk of VL in the island to have a low threshold of clinical suspicion of VL in the differential diagnosis of patients with fever, pancytopenia, and hepatosplenomegaly. For the local healthcare system, it is crucial to ensure supplies of pentavalent antimonial drugs and amphotericin B formulations to manage this reemerging NTD in the Island of Margarita. Similar to other NTDs, authorities need to consider social improvements to reduce the vulnerability of impoverished populations to develop VL and other poverty-associated infections.
Footnotes
Author contributions
Conceptualization: G.G. and A.F.H.M.; investigation: L.C.P.A and A.F.H.M.; resources: G.G., L.C.P.A., A.F.H.M, C.F.P and J.A.S.; writing—original draft preparation: L.C.P.A.; writing—review and editing: A.F.H.M.; visualization: G.G., L.C.P.A., A.F.H.M, C.F.P and J.A.S.; supervision: A.F.H.M, C.F.P and J.A.S. All authors have read and agreed to the published version of the manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics
Written informed consent for publication was obtained from the patient and the mother of the patient.