
Abstract
Background:
The aim of this study was to review the clinical data on the effectiveness of the pharmacotherapy of HIV-associated neurocognitive disorders (HANDs).
Methods:
A literature search of PubMed was performed (from January 1996 to October 2018) using the terms: ‘HIV-associated neurocognitive disorders’, ‘HIV-associated dementia’, ‘mild neurocognitive disorder (MND)’, ‘asymptomatic neurocognitive impairment (ANI)’, ‘adjuvant therapies’, ‘antiretroviral treatment (cART)’, ‘neurotoxicity’, ‘cART intensification’, ‘fluid markers’, ‘cerebrospinal fluid’, ‘protease inhibitors’, ‘nonnucleoside reverse transcriptase inhibitor’, ‘nucleoside reverse transcriptase inhibitors’, and ‘integrase strand transfer inhibitors’. Additional references were identified from a review of literature citations. All English language clinical studies of adjunctive therapies and neuronal markers were selected in order to evaluate a closer relationship between the early involvement and the onset of cognitive decline. We identified 407 relevant studies, of which 248 were excluded based on abstract analysis. Finally, we analyzed 35 articles, organizing the results by cART, adjuvant and neuronal markers (total of 7716 participants).
Results:
It is important to inform clinicians about the importance of accurate phenotyping of HIV patients, incorporating an array of markers relevant to HAND pathophysiology, in order to assess the individual’s risk and potential response to future personalized antiretroviral treatment
Conclusion:
So far, no clinical trials of HAND therapies are effective beyond optimal suppression of HIV replication in the central nervous system. Combination of validated neuronal markers should be used to distinguish between milder HAND subtypes and improve efficiency of clinical trials, after strict control of confounders.
Keywords
Introduction
In the mid-1990s, combined antiretroviral treatment (cART) was a real revolution in the improvement of overall survival of HIV patients. Moreover, the prevalence of the more severe form of HIV-associated neurocognitive disorder (HAND), has been reduced to 5%. 1 Although the widespread use of cART has led to a marked decrease in the number of patients with more severe manifestations of HAND (e.g. HIV-associated dementia), less severe forms of HAND, namely asymptomatic neurocognitive impairment (ANI) and mild neurocognitive disorder (MND), remain high in the cART era (between 33 and 60% of all HAND).2,3 Longitudinal cohort studies showed that ANI, even with a suppressed plasma viral load, evolved into symptomatic cognitive impairment. This spectrum of mild HAND impacts on daily functioning, poor adherence and mortality as occurring earlier during the course of HIV infection.4–6
The most common causes of this change, in proportion rather than an actual crude increase in the number of individuals diagnosed, include: (a) incomplete penetration of antiretroviral drugs (ARVs) into the central nervous system (CNS) with consequent deficient viral suppression, (b) drug-resistant viruses in the CNS, (c) neuronal damage due to perpetual viral replication in the CNS, (d) neurotoxic cART exposure as well as to other factors that impair cognition. 3
Cerebrospinal fluid (CSF) and plasma are thought to reflect the neuropathology with a complex protein profile comprised of different cell types. Prior to the introduction of cART, factors associated with HAND included plasma and CSF HIV RNA and inflammation markers [e.g. chemokine (CC motif) ligand 2 (CCL2), tumor necrosis factor (TNF), interleukin (IL)-6, and neopterin]. The complex nature of factors contributing to HAND suggests these disorders reflect different pathophysiological mechanisms. There is an obvious need for markers that reflect HAND in all of its complexity.
Previous reviews on the topic focused on the current knowledge of HAND pathogenesis and several markers (fluid and neuroimaging).7–9 However, it is unclear whether these markers can distinguish among various stages of HAND. The purpose of this review is to assess whether previous studies actually address the question of an optimal management of HAND by examine the evolving concepts of HAND neuropathogenesis, and new treatment approaches. Our focus was to evaluate studies of adjunctive therapies and fluid markers of neurological injury/immune activation in order to evaluate a closer relationship between early involvement and the onset of cognitive decline. Finally, we discussed future perspectives in the field of HAND therapies and proposed recommendations to improve quality and efficiency of clinical trials for optimal pharmacological management of HAND.
Methods
A literature search was performed in PubMed to identify studies published between January 1996 and October 2018 using terms as ‘HIV-associated neurocognitive disorder’, ‘HAND’, mild neurocognitive disorder MND ‘asymptomatic neurocognitive impairment ANI’, ‘adjuvant therapies’, ‘antiretroviral treatment cART’, ‘neurotoxicity’, ‘injury cART intensification’, ‘protease inhibitors’, ‘nonnucleoside reverse transcriptase inhibitor’, ‘nucleoside reverse transcriptase inhibitors’, ‘integrase strand transfer inhibitors’, ‘fluid markers’, and ‘cerebrospinal fluid’. Additionally, the reference list of each article was searched manually to include pertinent citations. Inclusion criteria were: adult human patients, publication date, and the English language. Letters, summaries, dissertations, reviews, theses, animal models and case reports were excluded.
To be eligible, studies had to meet the following conditions: (1) population: participants in the trials had to meet diagnostic criteria of HAND, ANI and MND and (2) primary outcomes were: new approaches to the treatment of HAND and their implications in the era of HIV eradication, specifically, adjunctive therapies targeting CNS inflammation and other metabolic processes, potential neuronal biomarkers for HAND; secondary outcomes were: evolving concepts of HAND neuropathogenesis.
Study selection and data extraction
A total of three investigators with advanced training in HAND pharmacotherapy and critical appraisal screened all titles and abstracts retrieved through the search. We further examined all full-text articles of identified abstracts that met inclusion criteria. In case of debate during the eligibility assessment, the other two study investigator reviewed the abstract/full text in doubt and made a final objective approval. We only included studies that fulfilled the appropriate diagnostic criteria established by the original authors. Any discrepancies between the investigators were resolved through discussion.
The variables extracted from each manuscript were the following: study type (including design), sample characteristics, type of treatment, dosage/mechanism of action, neuropsychological/biochemical/functional measures and main outcomes. After retrieving the full text of included studies, all investigators independently assessed the methodological quality of randomized controlled trials (RCTs) studies according to the Cochrane Handbook for Systematic Reviews of Interventions, 10 and the Newcastle–Ottawa scale (NOS) for assessing the methodological quality of cross-sectional studies. 11 The Cochrane risk of bias tool for RCTs incorporates sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other potential sources of bias. 10 Each item is rated as ‘yes’, ‘no’, or ‘unclear’. The quality of clinical trials can be divided into three levels. If the study design satisfied all the preceding six criteria, it is considered as an A level, which means a low risk of bias. A B level is assigned if one or more criteria are partly met, and when one or more criteria are not met, the study was defined as a C level, implying a high risk of bias. 10 The NOS criteria comprised: (i) Patient selection (scores, 0–4); (ii) comparability of subjects (scores, 0–2); and (iii) clinical outcomes (scores, 0–3). The NOS scores ranged between 0 and 9 and a score ⩾7 indicated that a study was of good quality. 11

Schematic Representation of HAND neuropathogenesis. A Schematic model demonstrating the key steps (activated macrophages, microglial cells) of HAND pathogenesis as well as potential targets of current therapies such as anti-inflammatory (minocycline), NMDAR antagonists/anti-excitotoxic (memantine), antioxidants agents (selegiline).
Results
The described search identified 407 relevant studies (Figure 1 supplementary material), of which 248 were excluded (duplicates, obvious irrelevance to our study aim by checking the titles and abstracts). A total of 159 abstracts were identified as relevant or potentially relevant. Of those, 122 were excluded (full texts could not be retrieved, eligibility criteria not met). Finally, 37 studies were reviewed as a full text. We performed qualitative data synthesis, organizing the results by cART (n = 11; Table 1), adjuvant therapies (n = 12; Table 2), and neuronal biomarkers (n = 12; Table 3). No further relevant citations were found from weekly electronic database updates up to 1 October 2018. Finally, we analyzed 35 articles: 10 RCTs, 17 cross-sectional, 1 open-label, single arm, 1 prospective, 1 cohort, 1 transversal analysis, 1 placebo-controlled, 2 longitudinal, 1 population-based with a total of 7716 participants (Tables 1–3). Given the heterogeneity of included studies, it was impossible to conduct meta-analyses. Tables 1–3 summarize the main methodological characteristics and results of the included studies. Our review identified 10 RCTs with a moderate methodological quality of level B. The NOS scores for cross-sectional studies ranged between 7 and 8 with good quality.
Summary of main characteristics of cART.

AVLT, auditory verbal learning test; PI, protease inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitors; INSTI, integrase strand transfer inhibitors; SDMT, symbol digit modalities test; GP, grooved pegboard test; COWAT, controlled oral word generation; FWL, four-word learning words recalled; DASS, depression anxiety stress scale; FAB, frontal assessment battery; CNS penetration effectiveness; WAIS-R, Wechsler adult intelligence scale-revised.
Summary of main characteristics of adjuvant therapies.

Cal Cap, California Computerized Assessment Package; ADAS-Cog, Alzheimer’s disease assessment scale-cognitive subscale; AMNART, American version of the Nelson adult reading test; ART, antiretroviral therapy; CI, cognitive impairment but not specified of which type of HAND; CSF, cerebrospinal fluid; C-W, color-word; DTI, diffusion tensor imaging; EPO, erythropoietin; FWM, frontal white matter; GP, grooved pegboard; h, hour; HAD-A, hospital anxiety scale; HAD-D, hospital depression scale; HAND, HIV-associated neurocognitive disorder; HDAC, Histone deacetylase; HDS, HIV dementia scale; IGF-I, insulin-like growth factor-I; IL, interleukin; m, months; MCP-1, monocyte chemoattractant protein-1; MIP-1alpha, macrophage inflammatory protein-1; MRS, magnetic resonance spectroscopy; NI-PI, name identity-physical identity; NMDA, N-methyl-d-aspartate; NP neuropsychiatric; NR, not reported; NS, not specified; RCT, randomized controlled trial; SRIs, serotonin reuptake inhibitors; TNFα, tumor necrosis factor α; TS, transdermal system; VL, viral load; VPA, valproic acid; w, weeks; WAIS-R, Wechsler adult intelligence scale-revised; WMS-R, Wechsler memory scale-revised.
Summary of main characteristics of fluid neuronal biomarkers.
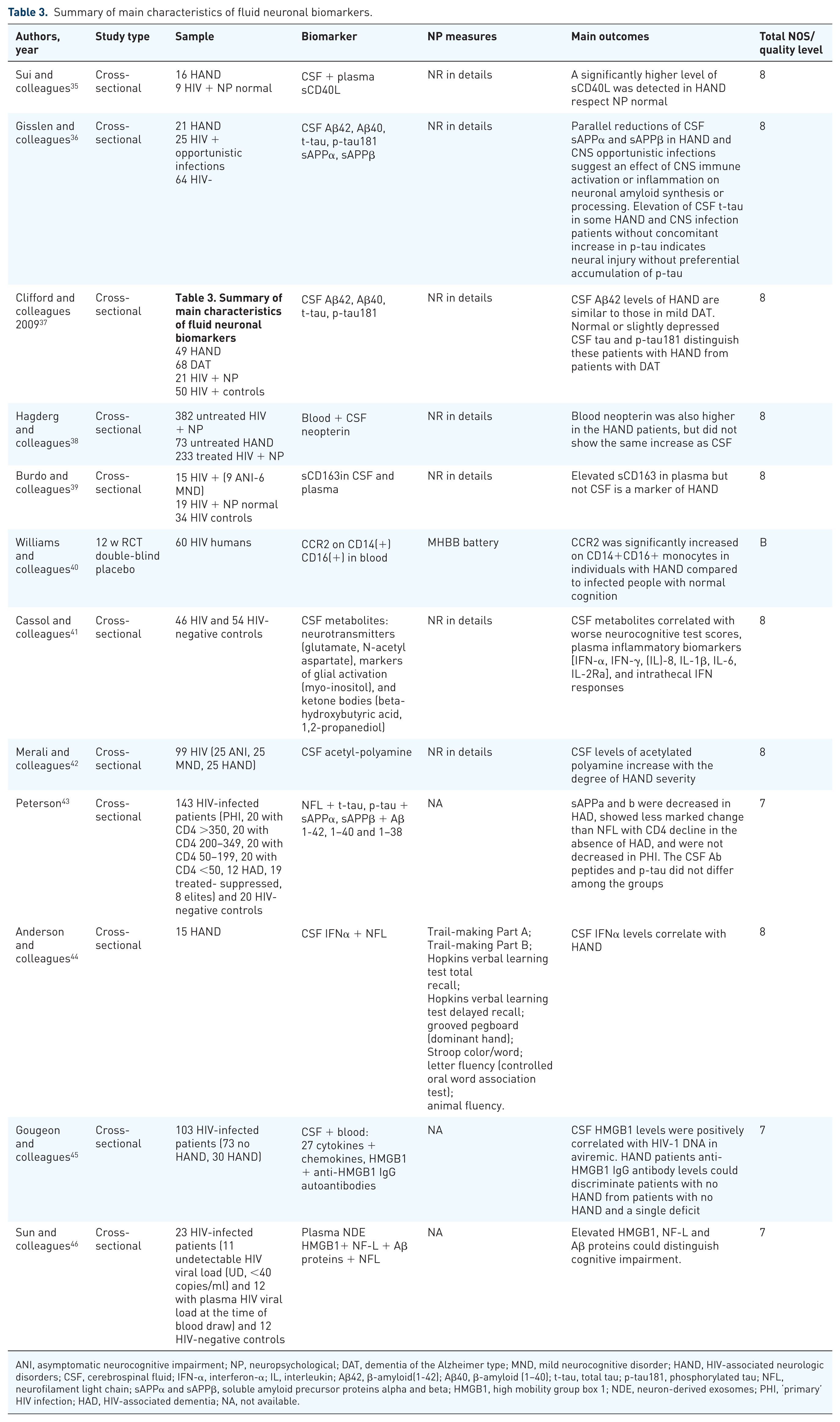
ANI, asymptomatic neurocognitive impairment; NP, neuropsychological; DAT, dementia of the Alzheimer type; MND, mild neurocognitive disorder; HAND, HIV-associated neurologic disorders; CSF, cerebrospinal fluid; IFN-α, interferon-α; IL, interleukin; Aβ42, β-amyloid(1-42); Aβ40, β-amyloid (1–40); t-tau, total tau; p-tau181, phosphorylated tau; NFL, neurofilament light chain; sAPPα and sAPPβ, soluble amyloid precursor proteins alpha and beta; HMGB1, high mobility group box 1; NDE, neuron-derived exosomes; PHI, ‘primary’ HIV infection; HAD, HIV-associated dementia; NA, not available.
Neuropathogenesis of HAND: inflammation, glutamate and glia as the trio of mess. A link between cART and HAND
Since 2009, there has been a robust body of evidence identifying sustained inflammation in HAND as a critical pathogenic element. The main idea is that HIV replicates in the CNS, particularly in subcortical structures. 47 This specific anatomical region may explain the neuropsychological impairment pattern observed in HAND. 48 Since neurons have the lowest susceptibility to HIV infection among all cells of the CNS, their dysfunction likely results from infection of neighboring cells such as macrophages and microglia, which are cells with immune functions in the brain. Activated macrophages and microglia (Trojan horses) produce viral proteins (glycoprotein, gp-120, Tat protein and chemokines) that have the ability to damage the synapse. These proteins also activate uninfected astrocytes (a key cell supporting neurons) which will result in increased glutamate release. 49 Elevated extracellular glutamate levels lead to aberrant synaptodendritic pruning and neuronal injury. Overall, all these toxic molecules participate in a vicious cycle with overactivation of NMDA receptors and consequent excitotoxicity, free radical formation, TNF-α, arachidonic acid, quinolinic acid and nitric oxide, resulting in glial activation and neurodegeneration. Other risk factors such as methamphetamine use, coinfection with hepatitis C and atherosclerosis contribute to HAND, through further activation of uninfected macrophages and microglial cells. Despite inflammation as a key feature of HAND, its presence in the CNS is not the sine qua non for active HIV viral replication. 50 So far, neuro inflammation continues to be the core of intense study, because inhibiting viral replication alone has delayed, but not stopped HAND progression.
The integrase strand transfer inhibitors (INSTIs) raltegravir, dolutegravir and elvitegravir are used as first-line ART in a combination of two nucleosides [nucleoside reverse transcriptase inhibitors (NRTIs) and either a nonnucleoside reverse transcriptase inhibitor (NNRTI), or protease inhibitor (PI)]. 51 These drugs may decrease the severity of neuropathogenesis but cannot prevent the emergence of milder forms of HAND. Older NRTIs (zidovudine and abacavir) are associated with a reduced incidence of HAD, which is likely attributed to effective CNS penetration. 51 A CNS penetration-effectiveness (CPE) index recently has been proposed to guide the choice of antiretrovirals in patients with HAND. Each antiretroviral drug is given a score of 1 to 4 (4 = much above average CNS penetration, 3 = above average, 2 = average, 1 = below average), and the sum of the individual agents’ scores in a combination regimen provides the CPE score for that regimen. Individual ART agents with scores of 4 include zidovudine, nevirapine, and indinavir/ritonavir. Notably, a combination of NRTI and NNRTI with good CNS penetration was associated with a poorer neurocognitive performance.16,20 Previous studies have yielded conflicting results on the effect of cART on cognition14,15,18,19,22,12,13,17 (Table 1). An explanation might be that the reduction of neural stem cell proliferation due to NRTIs could contribute to a decline in the regenerative actions of these cells, which under NNRTI conditions would oppose the chronic injury induced in the brain by HIV itself, HIV-activated glial cells, or HIV-secreted proteins such as gp120 and Tat.
Adjuvant therapies for HAND: what is new in an old story
Since the introduction of cART in 1996, 11 adjuvant therapies (as mitigates of pathogenesis) have been studied as following: (1) memantine, as a first generation NMDA receptor antagonist showed no cognitive improvement in HAND patients, 30 (2) selegiline a monoamine oxidase B inhibitor produced no significant benefit, 17 (3) deprenyl with cognitive improvement + thioctic acid (α-lipoic acid) without significant benefit, 24 (4) valproic acid (HDAC inhibitor, GABAergic effects) 28 with benefit, (5) lithium (unknown mechanism) 31 without benefit, (6) CPI-1189 (TNFα blocker) 27 without benefit, (7) peptide T (blocks gp120 binding to brain tissue) 25 with improvement in patients with NP global deficit score ⩾0.5 or with relatively preserved immunological status (CD4 count > 0.200 109 cells/L,(8) lexipafant (platelet-activating factor receptor antagonist) 26 with trends toward improvement, (9) OPC-14117 (free radical scavenger) 23 without benefit, (10) rivastigmine (acetylcholinesterase inhibitor) 33 without benefit, and (11) minocycline (tetracycline-class antibiotic) without benefit 32 (Table 2). These studies gave mixed results (seven negative versus four positive).
However, research efforts need a long way before gaining positive results in patients with HAND. Specifically, nitro memantine, a second-generation NMDA receptor antagonist that preserved synaptic normal activity, which suggested a better tolerability while allowing the use of higher and more effective doses.52,53 A combination of erythropoietin and insulin growth factor 1, two United States Food and Drug Administration (US FDA)-approved biological agents for other indications, showed a remarkable neuroprotection, in part, in a mouse model of HAND, through cooperative activation of phosphatidylinositol 3-kinase/Akt/GSK-3β signaling. Nonetheless, it still remains to be tested in humans with HAND. 54
Furthermore, statins HMG-CoA reductase inhibitors, have gained interest due to in vitro evidence of modulation of the immune system, and possibly of HIV replication. 55 However, there was no significant effect of atorvastatin on levels of CSF HIV RNA and neurocognitive performance. 55
Given that serotonin (5-hydroxytryptamine) and its receptors may play a role in HIV replication and disease progression, there has been growing interest in selective serotonin reuptake inhibitors (SSRIs, e.g. citalopram, sertraline, trazodone) as HIV infectivity modulators. While controlled studies are lacking, a cross-sectional study of 658 HIV patients with cognitive impairment has shown better neurocognitive performance as well as undetectable CSF HIV RNA with SSRIs, but not with statins. 34
Future directions of HAND pharmacotherapy research
One of the barriers of novel HAND pharmacotherapy is the lack of interest from the pharmaceutical industry in the development of therapeutics for HAND, because the condition has not been perceived as an applicable target. This condition translates into enormous costs for the academic sector to insist on new therapeutics for HAND. An example of ongoing efforts is the development of intranasal insulin, or cambinol (sphingomyelinase inhibitor), as therapeutic agents for ANI and MND. 56 Intervening with drugs targeting astroglia may disrupt the neuroinflammation during HIV-1 infection and methamphetamine abuse. These drugs may be multiple sclerosis drugs, such as fingolimod, 57 copolymer-1, 58 antioxidants, such as flavonoids, 59 and synthetic cannabinoids.60,61 HIV-associated comorbidities, neurological and metabolic complications and related glia implications will continue to constitute the hotspot of future research. So far, it is unknown how these interactions differ in the setting of long-term cART. Epigenetic factors may play a significant role in those interactions, but we have only seen the tip of the iceberg in terms of genetic susceptibility in future HAND pharmacogenomic research.
Immune and neuronal biomarkers
In 1998, the National Institutes of Health Biomarkers Definitions Working Group defined a biomarker as ‘a characteristic that is objectively measured and evaluated as an indicator of normal biological processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention.’ 62 In the new era of cART, both CSF and blood biomarkers of viral load, immune/inflammatory responses or neuronal injury are less likely to discriminate among the milder HAND subtypes. Elevated levels of sCD40L and TNF-α in CSF and plasma have been reported as a general marker for HAND. 35 CCR2 on CD14+CD16+ monocytes were not associated to HIV disease progression or severity of HAND. 40 Alterations in the CSF metabolome of HIV patients on cART overlapped with advanced age in HIV-negative controls. 41 CSF levels of acetylated polyamine increase with the degree of HAND severity. 42 Elevated sCD163 in plasma but not CSF is a marker of neurocognitive impairment in HIV infection. 39 Although nonspecific, elevated levels of CSF neopterin (marker for monocytes, macrophages, microglia, and astrocytes) are associated with an increased risk of dementia. 37 Low CSF leptin levels are associated with worse learning and memory performance in HIV-infected men. 37 CSF interferon alpha levels correlate with neurocognitive impairment in ambulatory HIV-infected individuals. 44 One of the promising neuronal biomarkers for dementia research, CSF Aβ42 levels [metabolized product of soluble amyloid precursor proteins (sAPPs)] were lower in HAND patients in respect to HIV + nondemented patients. 36 Increased CSF t-tau in HAND patients without a concomitant p-tau increase was reported as an indicator of neural injury without preferential accumulation of hyperphosphorylated tau as found in Alzheimer’s disease (AD). 43 Other neuronal CSF biomarkers, such as neurofilament light protein (NFL) showed a different profile in AD compared with HAND, (reduced sAPP levels and increased NFL levels in HAND). 45 Of the above CSF neuronal biomarkers, NFL was the most sensitive and demonstrated the presence of active neural damage in early HAD stage. 46 High mobility group box 1 (HMGB1), a proinflammatory mediator, was elevated in the CSF of HIV patients on stable cART, as a biomarker for early stages of HAND. 63 NDE from HAND patients had significantly higher levels of HMGB1, NF-L and Aβ proteins compared with HIV-negative controls. 64 Elevated HMGB1, NF-L and Aβ proteins could distinguish among the early stages of HAND. The combined view of these fluid biomarkers suggested a novel profile and evolution of neuronal injury across viral suppression.
Discussion
HAND remains an unresolved multifactorial problem in HIV patients under modern cART era that often achieves HIV suppression of replication to levels below the limit of detection of currently used assays. This review showed that no clinical trials of HAND therapies are effective beyond optimal suppression of HIV replication in the CNS.
An important finding of this review is the lack of definitive ‘adjuvant’ strategies. Significant methodological issues such as their cross-sectional nature do not permit causality. 56 However, an accurate longitudinal design is often impractical due to the prolonged period of HAND progression. In the same context, there is an absence of uniform access concerning neurocognitive assessment, likely related to multiple factors, including complex social situations, limited access to medical care and lack of concern in the HIV community as regards the long-term effects of HAND. For all these reasons, adjuvant HAND therapy would subsequently be tested in larger, and more rigorous confirmatory trials including multiple outcome measures such as neuropsychological scores, alterations of biomarkers or neuroimaging. 65
cART intensification involves extension of the traditional three-drug regimen to reduce inflammation caused by HIV and residual HIV viral replication, and hence the size of HIV latent reservoirs. There are conflicting data indicating whether intensifying cART will be necessary in cure strategies or not.64–68 Despite the coexistence of multiple sites of HIV reservoirs (lymphoid tissue, bone marrow) it is important not to ignore the CNS as a major reservoir site for eradication strategies. The key idea is to accomplish a ‘clean’ and ‘pure’ CNS for a successful HIV eradication strategy. A potential factor limiting the efficacy of ARVs in the CNS is the blood–CNS barrier. Ideally, high ARV penetration into the CNS in therapeutic concentrations may reduce HIV RNA levels in the CSF, and perhaps better neurocognitive performance. 69 ARV drug susceptibility, besides drug CNS penetration, can play a role in the control of HAND. 70 Further adding to the complexity is the presence of transporters at the blood–CNS barrier that actively pump out drugs, including many ARVs currently in use. Detecting latent viral reservoirs could be another step, but the degree of this elimination cannot be estimated. 71 In addition, latency reversing agents might pose a risk of inflammatory over-response by activating latent viral reservoirs in the brain in immunocompetent patients with further neurological damage.
A crucial step is to quantify the penetration of various ARV drug regimens with emphasis on the CSF as a reflection of disease progression in CNS. Observational studies, rather than longitudinal, on reductions in the CSF viral load as a function of the resulting CPE have yielded controversies and no correlation with the development of HAND is proven. 72 The range to which ARV distribution and CNS toxicity influence clinical outcomes is also questionable. Dolutegravir (DTG), a once-daily, HIV type 1 (HIV-1) integrase inhibitor, achieved therapeutic concentrations in the CNS of cART-naïve patients. 73 In contrast, in a large cohort of 1938 HIV cART-naïve patients at enrollment, 74% of those receiving cART with high CPE showed an increased risk of HAND. A practical guide suggests the use of the most tolerable cART regimen, without taking into account nonverifiable CPE in order to avoid confusion.
There is a matter of involvement of poor neurocognitive function under cART and neurotoxicity of these drugs, leading to persistence of HAND. 74 One in vitro study, using markers for neuronal damage (MAP-2 staining, dendritic arborization complexity, and neural responses to exogenous calcium) showed neuronal toxicity of 15 different antiretroviral drugs from different drug classes. 75 For example, long term use of efavirenz, a common cART, was correlated with worse neurocognitive functioning compare to lopinavir-ritonavir, suggesting an antiretroviral neurotoxicity. 21 However, drug–disease interactions, such as hepatitis C virus coinfection, are still too complex to be explained. The clinical relevance of these findings for other cART regimens remains uncertain. The question is whether the benefits of better HIV suppression through greater penetration of antiretrovirals in the CNS may be balanced by neurotoxicity. Even the large and prospective HIV Anti-Retroviral Therapy Effects Research (CHARTER) study was unable to demonstrate cART effects. 76 Early introduction of cART with strict monitoring assure sustenance of viral suppression and immune-competence, leading to favorable neurocognitive effects. 77 For the past two decades, cART has been an indisputable life-saving regimen, and hence should not be discontinued, despite the theoretically complex issue of neurotoxicity.
One of the strengths of this review is to reveal the absence of sensitive and highly specific markers of HAND subtypes prediction/or progression in previous studies.34,35,56,57–62 A potential explanation might be the lower levels of immune activation in HIV patients with prolonged viral suppression on cART. There may be other non-inflammatory mechanisms, such as cerebrovascular dysfunction, metabolic modifications, or neurotoxicity of cART regimens, but their relationship with HAND subtypes remains elusive. However, a promising finding of this review is that the combination of fluid neuronal biomarkers could distinguish among early stages of HAND 55 and further predict a positive outcome of cART.
There are various limitations of the included studies. First, numerous methodological issues were identified in many of the studies such as poor study design (e.g. cross-sectional). Future research should include longitudinal studies with important information on how individual differences impact long-term treatment outcomes. Second, there are various confounding conditions in included studies such as demographics (e.g. age, race, sex), comorbidities (HCV coinfection, smoking, alcohol.14–16,18–20,22,30,12,13,17 Third, there is an important heterogeneity of HIV cohorts (e.g. current and nadir CD4 count, initiation of cART, previous and current cART regimens), which make difficult to establish a clear causal link between treatment and outcome.14–16,18–20,22,30,12,13,17 Another issue regarding cART monitoring using biomarkers is the heterogeneity of techniques; for example, current standard enzyme-linked immunosorbent assay methods are insensitive to very low concentrations of biomarkers in CSF and blood. However, major differences existed for (1) type of antibodies, (2) type of calibrators to build the standard curve, and (3) detection/quantitation methods. Future studies should include monitoring with standard methods for biomarkers employed in drug discovery for HAND.
However, this review is not without its limitations. There are a small number of studies available for analysis. We searched a limited number of databases. Consequently, there is always the possibility that we overlooked studies in other databases. In addition, there is always the possibility of publication bias due to underreported negative results and grey literature. However, the use of fewer search limits increases the sensitivity of the search method.
Relevance to patient care and clinical practice
An accurate phenotyping of HIV patients, incorporating an array of markers relevant to HAND pathophysiology, may assess the individual’s risk and potential response to personalized antiretroviral treatment.
Conclusion
So far, optimal pharmacotherapy of HAND does not exist. HAND is not a rare complication in HIV patients under cART. HAND management remains an under-researched clinical entity with many unanswered questions regarding its epidemiology, pathophysiology and treatment. The wide range of adjuvant therapies that have been studied for HAND management show that we are still in an exploratory phase regarding its treatment. This review provides foundation for future studies using standardized procedures to confirm previous findings and expand on speculations as to whether a combination of biomarkers can increase discriminating power. There is a lack of highly specific markers to distinguish HAND subtypes or predict the disease’s progression. A combination of validated surrogate markers should be used to distinguish between milder HAND subtypes and improve efficiency of clinical trials, after strict control of confounders.
Supplemental Material
Fig1_supplementary – Supplemental material for Optimal treatment of HIV-associated neurocognitive disorders: myths and reality. A critical review
Supplemental material, Fig1_supplementary for Optimal treatment of HIV-associated neurocognitive disorders: myths and reality. A critical review by Anastasia Bougea, Nikolaos Spantideas, Petros Galanis, George Gkekas and Thomas Thomaides in Therapeutic Advances in Infectious Disease
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Ethical approval
This is a critical systematic review of publish studies thus there is no need to obtain a consent from the local Ethics Committee of Institutional Reviewer Board. There is no need to include a statement as to whether written/verbal consent was obtained from the patients or patients’ parent/carer.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.