
Abstract
Background:
Diseases caused by invasive nontyphoidal Salmonella strains present with various extraintestinal manifestations, including bacteremia. Factors affecting the incidence include Salmonella serotype, geographic location, and host factors.
Case:
We present an unusual case of Salmonella enteritidis primary bacteremia in a patient without any risk factors and originating from a region with the lowest burden of invasive nontyphoidal Salmonella infections. We observed an incomplete clinical response to the treatment with a third-generation cephalosporin, despite the in vitro susceptibility of the strain.
Discussion:
The diagnosis of Salmonella bacteremia was far from expected in our previously healthy patient from Taiwan, without any preceding diarrhea and the lack of marked response to therapy with ceftriaxone. Making the diagnosis was a challenge, requiring wide range of laboratory, imaging, and consultative work to rule out alternative diagnoses and complications.
Conclusion:
Invasive Salmonella infections are uncommon in our clinical practice at the present. Air transportation, intensive migration processes, and changes in climate are able to change the burden of infectious diseases dramatically in the near future. That fact along with the raising antibacterial resistance among invasive nontyphoidal Salmonella strains make imperative the profound understanding of the epidemiology and pathophysiology of those infections.
Introduction
Salmonellae are Gram-negative motile bacilli, which belong to the family Enterobacteriaceae. There are currently 2463 serotypes (serovars) of Salmonella species [Brenner et al. 2000]. They typically produce one of three distinct syndromes: nontyphoidal enterocolitis, nontyphoidal focal disease, or typhoid (enteric) fever. The severity of illness in individuals with nontyphoid salmonellosis is determined by the virulence factors of the infecting strain and also by host properties [Hohmann, 2001]. The most common risk factors for primary bacteremia and death in recent researches from Taiwan were found to be infection with group B, C, and D Salmonellae, immunodeficiency, presence of systemic lupus erythematosus, liver cirrhosis, solid organ cancers, and age [Hsu and Lin, 2005]. Salmonella enteritidis is reported to be the commonest isolated serotype from Taiwan hospitals (about 28% of the isolates), but Salmonella choleraesuis is mostly associated with primary septicemia [Chiou et al. 2015; Jean et al. 2006].
Case report
A 61-year-old previously healthy Taiwanese male presented to the emergency department (ED) of our hospital, with a 4-day history of fever up to 40°C with marked chills and shivering, malaise, and anorexia. His symptoms appeared during a direct flight from Taiwan to Bulgaria, where he was to spend a holiday with his wife. On the day of admission, he vomited several times and became somnolent. He and his wife denied the presence of any chronic diseases and previous hospitalizations, smoking, or alcohol intake. In spite of the age, the patient was actively engaged in sports. He did not have diarrhea neither from the onset of the disease nor on the previous days. He denied having had any contact with acutely ill patients.
Physical examination on admission revealed a weak, somnolent patient with subnormal temperature of 34.9°C, arterial blood pressure 104/78 mmHg, heart rate 88 per minute, dry mucous membranes, increased bowel sounds on abdominal auscultation, and mildly enlarged liver on palpation (2 cm below the ribs). No other abnormalities in the physical status were observed. Except for the somnolent state and the difficulties to come in verbal contact, the rest of neurological examination was unremarkable.
Laboratory tests performed during the hospital stay showed moderately increased leucocytes in the beginning with neutrophilia and left shift, which changed to normocytosis with normal distribution of the white cell types. Other abnormalities at admission included markedly elevated C-reactive protein (CRP) level, liver enzymes, mild hypoalbuminemia, slightly elevated blood glucose, and urea blood products. Further elevation of creatine phosphokinase (CK) and a drop in platelet count to below 100 × 109/L on the fifth day after hospitalization occurred. In the next days, they gradually returned to normal values. The urine examination revealed transient mild proteinuria. The rest of the laboratory tests were in normal ranges during the whole period, including acid–base profile, serum electrolytes, alpha-amylase, and urine sediment (Table 1).
Laboratory investigations during the hospital stay.

ALT: alanine transaminase; AP: alkaline phosphatase; AST: aspartate transaminase; CRP: C-reactive protein; CK: creatine phosphokinase; GGT: gamma-glutamyltransferase; Hb: hemoglobin; INR: international normalized ratio; LDH: lactate dehydrogenase; NA: not available; RBC: red blood cell; WBC: white blood cell.
Electrocardiogram (ECG) and chest X-ray performed in the ED were normal. Computed tomography (CT) of the brain revealed mild ventricular dilatation and hyperdense cerebral arteries with calcifications (age-related accidental findings unrelated to the present disease).
After an hour’s stay in ED, the patient was transferred to the infectious diseases department for further diagnosis and treatment, where blood, urine, and feces samples were obtained for microbiological examination, as well as for malaria and serology testing. For the suspicion of severe infection of unknown bacterial etiology and localization wide spectrum antibiotic combination (ceftriaxone + amikacin) was started intravenously. Additional therapy consisted of fluconazole as antifungal prophylaxis, parenteral rehydration with fluids, 20% human albumin as antiedema treatment for the signs of encephalopathy, probiotics, hepatoprotectors, and antipyretics.
In the first 12 hours after the initiation of treatment, the patient’s renal function fully recovered, and the patient became alert and fully responsive, but remained febrile with a temperature up to 41°C for the next 10 days. The rise in temperature was accompanied by shaking chills and profuse sweating during its critic drop. Except for the persistent anorexia, he was feeling normal between the fever periods. On day 2, a scanty petechial rash under the right axilla appeared, which disappeared without any sequel until day 5. No additional signs that could help in topical or etiologic diagnosis in the physical status appeared.
Abdominal and retroperitoneal ultrasound (US) on day 4 revealed two oval-shaped well-demarcated hyperintense lesions (13 and 11 mm in diameter) in the liver, most probably hemangiomas. Cardiac US on day 4 did not find any abnormalities.
Meanwhile, parasitologists failed to find malarial plasmodia from six blood specimens; cultures from feces were found negative for Shigella, Salmonella, and other pathogenic Enterobacteriaceae species; serology testing for viral hepatitis found only anti-HBc total antibodies positive; and HIV serology was negative.
The above-described laboratory results, imaging studies, along with the performed consultations with respiratory physician, endocrinologist, gastroenterologist, and parasitic diseases specialist ruled out malaria, carditis, acute viral hepatitis, cirrhosis, and pulmonary inflammation.
The so manifested fever of unknown origin (FUO) required further investigations. Abdominal CT on day 9 revealed the following abnormalities: discreet bilateral pleural effusions basally with minimal compression signs of the above lying pulmonary parenchyma; small amounts of ascites; two hyperintense lesions 12 mm in diameter segment 8, and 6 mm in segment 7 in the liver, showing CT characteristics of hemangiomas; a borderline hypertrophy of the medial suprarenal peduncule on the left (the formation of a nodule in it could not be excluded); and a well-demarcated hypointense oval shaped lesion 14mm in diameter in the L1 vertebral body with lipid-equivalent density (differential diagnosis – atypical hemangioma). No retroperitoneal or mesenteric lymph nodes were found enlarged; the rest of the structures in abdominal cavity, retroperitoneum, and pelvis showed normal CT characteristics (Figure 1).
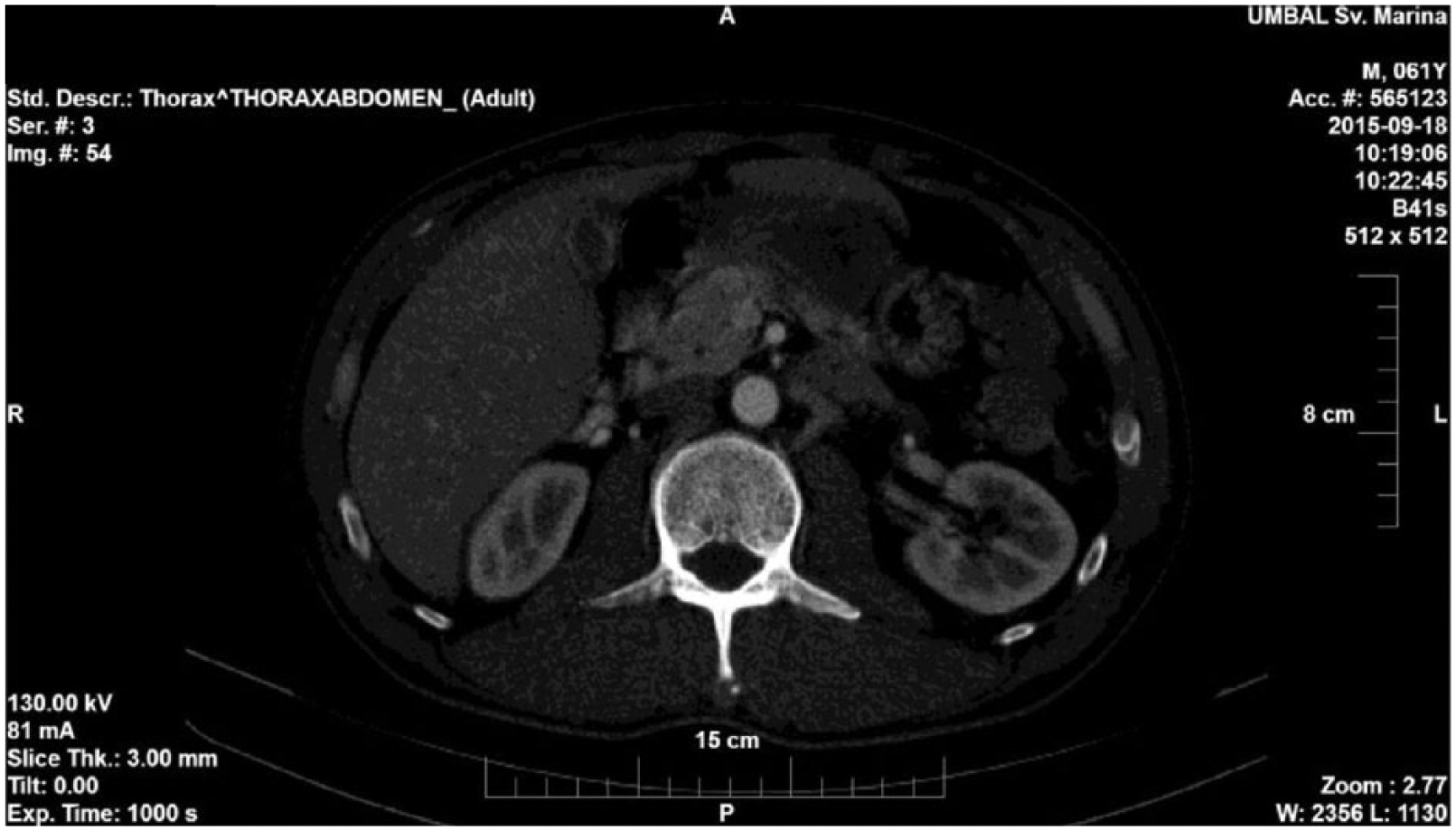
Abdominal computer tomography showing a hyperintense lesion in the liver on day 9 after admission.
Due to the lack of response to therapy on day 7, the initial combination ceftriaxone–amikacin was replaced by intravenous levofloxacin. The diagnosis was elucidated by blood cultures, which grew S. enteritidis. In terms of antibacterial susceptibility, the encountered strain appeared highly sensitive: ampicillin/sulbactam, piperacillin/tazobactam, ticarcillin/clavulanic acid, aztreonam, cafapime, cefotaxime, ceftazidime, ceftriaxone, ciprofloxacin, levofloxacin, ertapenem, imipenem, meropenem, and trimetoprim/sulphametoxazol.
The patient became afebrile on day 11, his clinical condition gradually improved during the stay, his appetite was fully restored, and no additional symptoms appeared through the hospital stay. He was discharged after 10 days of treatment with parenteral levofloxacin with recommendations of further 5 days intake of levofloxacin + probiotic perorally. He left the country immediately after discharge, thus making his follow-up impossible.
Discussion
This was a case of invasive nontyphoidal Salmonella (iNTS) infection, primary bacteremia, a diagnosis that was actually far from suspicion at presentation. S. enteritidis is the second most encountered serovar causing iNTS infections, without diarrhea, accounting for 33.1% of all cases [Ao et al. 2015]. According to the results of a research on epidemiology of nontyphoidal Salmonella strains in Malaysia and Spain, serotype enteritidis strains were the most invasive [Dhanoa and Fatt, 2009; Galofre et al. 1994]. iNTSs have emerged as a prominent cause of bloodstream infection in Africa and have adapted to occupy an ecological and immunological niche provided by HIV, malaria, and malnutrition, with an associated case fatality of 20–25% [Feasey et al. 2012]. Yet, NTS primary bacteremia in our case was unexpected for two major reasons. First was the lack of any predisposing host risk factors such as immunosuppression and co-morbidities [Gordon, 2008]. The second was that our patient originated from the world region with the lowest burden of iNTS diseases − 0.8/100,000 population in that part of Asia [Ao et al. 2015]. Therefore, making the diagnosis was a challenge, requiring wide range of laboratory work, imaging studies, and consultative work to rule out other possibilities. Furthermore, in the setting of a lack of decisive response to the therapy with ceftriaxone, it was important to rule out co-infections and complications. The most feared complications were cardiovascular, due to the unique virulence mechanism of Salmonella species to infect endothelial-lined structures, confirmed by a number of case reports in relation to it [Ohl and Miller, 2001; Hibbert et al. 2010; Ortiz et al. 2014; Gorecki et al. 2008; Papamichalis et al. 2011]. Thus, the differential diagnosis included typhoid fever, sepsis with other etiology, recurrent typhus, endocarditis, Q-fever, malaria, flu, HIV-infection, abscesses in the liver, suppurative hydatid cysts in the liver, renal infection, hematologic malignancy debut, and so on.
In terms of treatment, we observed an incomplete clinical response to it, in spite of the fact that it was started with a third-generation cephalosporin, which coincided with the in vitro susceptibility of the particular isolate. In addition, the microorganism remained constantly undetectable in blood, urine, and feces in all samples but the first one. Full response to therapy was achieved after 3 days of application of parenteral levofloxacin. Complications and additional diseases accounting for that fact had been ruled out. The explanation might be found in the intracellular distribution and survival of iNTS similar to Salmonella typhi in typhoid fever. This scenario is corroborated with some studies of S. typhi infection, in which fluoroquinolones result in more rapid and durable clinical response than do cephalosporins, and from in vitro data, which show greater penetration of fluoroquinolones into phagocytic cells where Salmonellae persist [Cao et al. 1999; Chiu et al. 1999].
Invasive Salmonella infections, especially primary bacteremia without preceding diarrhea, are not typically observed in our clinical practice even in our HIV-infected patients. The most possible explanation is the low burden of iNTS strains in our community.
Conclusion
The fact that we have encountered such an iNTS disease in a patient from the most remote region of the world should not calm us. Air transportation, intensive migration processes, and changes in climate make the possibilities for introducing new strains among atypical populations quite real. Unfortunately, that fact in combination with the raising antibacterial resistance among iNTS strains makes the future in the best case insecure for the patients with invasive salmonellosis and quite problematic for their physicians.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.