
Abstract
Background
Young patients who suffer from a pediatric condition are typically submitted to diverse and often repeated painful procedures. Theory and empirical studies suggest that communication styles used by healthcare professionals could mitigate such procedural pain. Recently, a hypnotic communication training (Rel@x) was developed with promising results. The present study aimed to describe how healthcare professionals change the words they use with patients after training.
Methods
A nine-hour training in hypnosis-derived communication was offered to 78 volunteer healthcare professionals from a tertiary pediatric hospital, and 58 participated in the evaluative study. Participants were evaluated at baseline, immediately after the training, and 5 months later (39 ± 10 yrs, 52 women, 54 nurses). We used a video-recorded standardized simulation protocol of venipuncture, and five categories of words were derived. Word categories were corroborated in a validity study with 10 independent judges. We modeled pre-post-follow-up changes over time with latent growth curve models.
Results
Following training, healthcare professionals used fewer words related to negative experiences (−51%) or medical procedures (−73%) and used more words referring to the relaxing and analgesic experience (+20%), and the specific techniques they had learned (Pleasant place +260%, Magic glove +582%). These changes were maintained at a proportion of 45–81% 5 months later. More change was observed among women and less experienced healthcare professionals.
Conclusion
Results suggest that healthcare professionals exposed to a short, structured communication training aiming to mitigate pediatric pain durably adjust the language they use when performing a painful procedure. This is encouraging for future testing and implementation of hypnosis-derived communication training in healthcare providers.
Introduction
Pain associated with medical procedures is identified as the number one issue and source of fear by young patients.1–3 This is especially the case when repeated medical procedures are necessary in situations of serious or chronic diseases requiring lengthy or repeated treatments (e.g., cancer). Research has found that such experience of pain can generate chronic stress, anticipatory fears, and post-traumatic symptoms in young patients, among other negative consequences.1,4–6 This can also lead to avoidance and issues in self-care or self-management in the long run. 6
To manage and prevent pain in pediatrics, healthcare professionals may call for a wide variety of methods. 7 These include pharmacological interventions (e.g., anesthetic cream) and non-pharmacological interventions such as communication techniques. The communication style employed by a healthcare professional has the power to mitigate much of the pain response by decreasing anticipatory fears and favoring positive experiences.8,9 Using communication to modulate the pain experience is based on the motivational priming theory, according to which negative semantic stimuli can heighten subjective pain perception.9,10 In contrast, the pain gate theory suggests that presenting a positive stimulus alongside negative stimuli (e.g., painful medical procedure) can mitigate the negative (e.g., painful) experience. 11
Hypnotic communication is a form of communication derived from the communication principles elaborated in clinical hypnosis interventions. 12 This form of communication modifies the perception of pain and procedural distress through suggestion and dialogue with the child. Several studies have reported positive effects of clinical hypnosis on pain and distress.13–15
Hypnotic communication is characterized by relating with patients to develop trust and collaboration.16,17 It typically requires that healthcare professionals use positive and relaxing words, reducing the pace of verbal communication to introduce suggestion-based and imagery-based techniques (e.g., suggesting numbness in a part of the body).16,18 Consistent with this approach, healthcare professionals refrain from using medical terminology or jargon as it is a barrier to communication, and it may attract patients’ attention to the cause of pain. Healthcare professionals also avoid using negative words and negative suggestions, such as those referring to stress or pain.16,18,19 As part of an endeavor to encourage the development of this communication style in healthcare professionals, a manualized training was recently tested (Rel@x 20 ). It demonstrated excellent feasibility and was associated with long-term skill maintenance in a sample of 58 healthcare professionals.20–22
In the present study, we quantitatively analyzed encounters that were video-recorded during the aforementioned feasibility study. 22 Encounters between a healthcare practitioner and an actor simulating a venipuncture occurred before and after a standardized hypnotic communication training. In coherence with the hypnotic communication principles mentioned previously, we explored whether words used by healthcare professionals would change over time, before and after training, and if these changes would be maintained in the long term. The results could demonstrate the extent to which hypnotic communication skills translate into words used by healthcare professionals. It could also serve to develop new, concrete, and objective outcome measures for communication interventions in this field.
Objectives
This study aimed to evaluate changes in the lexical content used by healthcare professionals following Rel@x, a communication training to help them mitigate procedural pain and distress in children. We explored the following research questions: (1) Did healthcare professionals use different words after training and at follow-up than before the training? This should be reflected in the use of proportionally: (a) more relaxing and analgesic experience words, (b) fewer negative experience words, (c) fewer medical words or words related to the painful procedure, and (d) more words reflecting the hypnotic technique learned. (2) If these changes were significant, did they depend on the healthcare professionals’ baseline levels and their individual characteristics (i.e., age, gender, and seniority)?
Methods
Study design
The study is a secondary analysis of video-recorded simulations of healthcare professionals performing a venipuncture on an actor playing the role of a patient. Data were collected before and after training, and at a 5-month follow-up (see procedure below). Data were collected between May 2021 and March 2023. Ethical approval was granted by the Ethics Review Committee of CHU Sainte-Justine (#2019-2205), and the research was conducted according to the principles expressed in the Declaration of Helsinki. All participants provided digital informed consent.
Participants
A full description of the study sample and procedure is available in a previous report. 22 Participants were healthcare professionals working in a large Canadian tertiary hospital (CHU Sainte-Justine, Montreal, Québec) who voluntarily registered for the Rel@x training. To be eligible to participate in this study, participants had to regularly perform venipunctures on pediatric patients as part of their clinical practice. Participants who had prior training in hypnosis or hypnotic communication were excluded from the present study. Participants were compensated for their time on training and received a CAN$50 gift card after completing the study.
Fifty-eight healthcare professionals were trained with Rel@x and assessed with the simulation protocol. The sample consisted of 52 women (89.7%) and six men (10.3%) aged 39 ± 10 years. Participants were nurses (n = 54) and physicians (n = 4), and they had a work experience of 16 ± 10 years, with 14 ± 10 years in pediatrics. They worked in the hematology-oncology department (n = 31), the emergency unit (n = 13), and other hospital departments (n = 14) (Supplement Figure S1).
Interested healthcare professionals were included in the present study following a recruitment campaign targeting nurses (internal leaflets, e-mails, targeted staff meetings). The study coordinator provided them with complete study information, an electronic consent form, and a brief sociodemographic questionnaire. After obtaining consent from participants and considering their availability, they were assigned to one training group (13 training groups, n = 3-10, median = 6 participants/group).
Procedure
Training
The Rel@x training took place in person in the hospital. The training consisted of two training sessions completed within a median of 14 days between sessions #1 and #2 23 . The first session aimed to introduce participants to the main relational aspects of hypnotic communication. Participants learned about verbal communication (i.e., using positive words, not using negation or negative charged words), nonverbal communication (i.e., posture, eye contact, and body language) and paraverbal communication (i.e., tone, rhythm, and volume). The second session focused on one of the two techniques proposed during the consent process: (1) The Pleasant Place or (2) The Magic Glove.
The Pleasant Place technique is a guided imagery method designed to help children recall a pleasant moment during a medical procedure. This technique engages the child’s imagination and the five senses. The healthcare practitioner asks patients questions to gather as many details as possible about their pleasant place and encourages them to immerse themselves in an imaginary scene as realistically as possible, using the relational processes mentioned above. 23 The Magic Glove technique is a method that incorporates the child’s imagination, along with analgesic suggestions and sensory desensitization (touching the area to be treated). 24 Patients are typically instructed to imagine wearing a magic glove with protective power, providing analgesia and a sense of numbness. 24
As a result to the previous feasibility study, 25 participants were free to choose the technique they wished to train, in order to optimize engagement. In total, 50 participants (86%) were trained in the Pleasant Place technique, and 8 participants (14%) were trained in the Magic Glove technique. The training followed the curriculum developed in previous studies.20,22,26
Video-recorded simulations
We video-recorded participants performing a simulated venipuncture on an articulated arm with no venous return. The first simulation (T1, pre-training) took place just before session #1, the second simulation (T2, post-training) took place immediately after session #2, and the third simulation (T3, follow-up) took place approximately 5 months after T2 (median 5.1 months, IQR 4.40–5.55). In a subset of 11 participants, we had the opportunity to collect a 1-week baseline point before the training using the same procedure in order to explore temporal stability in absence of training. Participants were required to perform a venipuncture. After training and follow-up, actors followed a standardized scenario portraying a 15-year-old patient receiving treatment for Ewing’s sarcoma (Supplement Table S1). For the Pleasant Place, the patient depicted enjoying a picnic with their family in a park, and for the Magic Glove, the patient reported decreasing sensations as the glove was placed on their arm. The simulation protocol allowed participants to practice with an actor reacting positively to their communication technique. Actors were selected among psychology undergraduates and trained to strictly follow the scenario.
Measures
Main outcomes
All video-recorded encounters were transcribed. We used the Sonix® software for transcription and checked all transcriptions manually. We then applied word count using the R (tm and stringr packages). The words were then categorized according to lexical content. Categories of words (or lexicon) were derived from the existing literature on hypnotic communication and the training itself. Five categories of words were constructed: (1) Relaxing and analgesic experience words. This lexicon encompassed all words related to relaxing and analgesia sensations and included words such as “comfort,” “relaxation,” “calm,” or “happiness.” (2) Negative experience words. This lexicon encompassed words of unpleasant sensations or experiences and comprised words such as “pain,” “fear,” or “stress,” and included the use of negation. (3) Medical and Procedure words. This lexicon refers to medical procedures, medical equipment, procedural context, or disease. This lexicon comprised words such as “venipuncture”, “tourniquet”, or “vacutainer”. (4) Words specific to the Pleasant Place. This lexicon encompassed the lexical field of the imagined pleasant moment from the simulation protocol, i.e. a picnic in a park. It included words such as “sandwich,” “trees,” or “picnic basket.” (5) Words specific to the Magic Glove technique. This lexicon encompassed the sensation of analgesia produced by the glove; it referred to the arm’s anatomy, the glove description and the lexical field of superpowers and protection and included words such as “glove,” “imaginary,” or “magic.”
After a necessary step of data cleaning involving regrouping occurrences of similar words (plurals, conjugated verbs), we used the Antidote® search tool and a lexical field dictionary 27 to define each lexicon. We then led a preliminary face-validity study of the five lexica. We asked 10 independent judges (six psychology graduate students and four young professionals) without prior involvement in the study to confirm or reject each word previously included in the five lexica. Each judge had five lists of words that they were instructed to relate with a brief definition. Judges were instructed to tick “agree” or “disagree” to include each word listed to represent the brief definition. For instance, they had to evaluate whether “pain” would belong to the Negative experience lexicon. If they ticked “disagree,” they were required to provide a brief explanation in writing. Overall, very few words were discarded by judges, and when they were, only a few judges did so. As an index of validity, we calculated the median agreement % among the 10 judges. The results were in support of the five lexica: Relaxing and analgesic experience: median = 98% (n of words = 323), Negative experience: 94% (n = 213), Medical and Procedure: 98% (n = 84), Magic glove: 98% (n = 209), Pleasant place: 96% (n = 787). After this analysis, we discarded three words with lower face validity. The detailed results of this analysis and the decisions made are available in Supplement Tables S2 and S3. Each category’s final content and the lexicon’s final definition are available in Supplement Table S4.
Then, we used an Excel spreadsheet to count the number of occurrences of each word belonging to each category at the individual level. We calculated the total number of occurrences of words in each category (e.g., total N of Relaxing and analgesic experience words). For instance, if the word “calm” was used three times, it counted for a value of 3 in this total score. We then divided the total number of occurrences for each category (or lexicon) by the total number of words used by each healthcare practitioner during the whole encounter. This calculation provided a proportion of occurrences of words of each lexical set that would later be analyzed in the main analysis: (1) Medical and Procedure, (2) Negative experience, (3) Relaxing and analgesic experience, (4) Pleasant Place technique, and (5) Magic Glove technique.
Contributors
We collected the following descriptives from an online self-reported questionnaire completed by participants when accepting to participate in the study: age (years), gender (men vs women), profession (nurses vs physicians), years of practice, years of practice in hematology-oncology, and chosen technique (Pleasant Place vs Magic Glove).
Analysis
We conducted preliminary analyses to ascertain distribution variability in outcomes and described the three timepoint scores (pre-, post-, and 5-month follow-up) using a distribution chart. Following recommendations when missing data are limited (in this case 1.27%), we used the full-information maximum likelihood estimation method (FIML) to deal with missing data, allowing us to retain all participants. 28 For the main analyses, we used latent growth curve models (LGCMs) to examine changes over time, as they are recommended for interventions with small sample sizes (e.g., n ≤ 50 participants). 29 Each LGCM included an intercept with its variance (i.e., the average initial level of the score and inter-individual variations around this average initial level) and a slope with its variance (i.e., the average amount of change across all participants and inter-individual variations around this average level of change).
In the first step of the analysis, we compared two models for each outcome variable (i.e., Medical and Procedure, Negative experience, Relaxing and analgesic experience, Pleasant Place technique, and Magic Glove technique). (1) A linear model was estimated, where linear change was expected in the outcome variable over time. (2) A non-linear model was estimated, where a non-linear change was expected in the outcome variable over time. In this model, the first time point was constrained to be 0, the second time point was constrained to be 1, and the third time point was freely estimated. This way, the slope reflected the total change between T1 and T2, while the freely estimated time point (T3) reflected how much change occurred in T3 compared to the initial change level (T1–T2).
In the second step of the analysis, we added time-invariant predictors of the intercept and the slope (i.e., age, gender, profession, years of practice, years of training in hemato-oncology, and technique chosen) to examine their potential associations with the initial scores of the outcomes as well as with their change over time. Age, years of practice, and years of training in hemato-oncology were used as continuous variables. Gender (i.e., women = 0, men = 1), profession (i.e., physician = 0, nurse = 1), and technique chosen (i.e., magic glove = 0, pleasant place = 1) were used as categorical variables in the analyses.
Models were evaluated using sample-size independent goodness-of-fit indices: Comparative Fit Index (CFI; ≥.90 adequate; ≥.95 excellent), Tucker-Lewis Index (TLI; ≥.90 adequate; ≥.95 excellent), and Root-Mean-Square Error of Approximation with its 90% confidence interval (RMSEA; ≤.10 acceptable; ≤.08 adequate; ≤.06 excellent).30–32 The robust maximum likelihood estimator was used for all LGCMs.
LGCMs were performed in Mplus 8.7®. Other statistics were performed in SPSS v24 and Excel 365 2023. The repository to access data and syntax is: https://doi.org/10.17605/OSF.IO/SRX5J
Results
Preliminary results
When comparing raw differences within non-imputed data across time points, we observed a significant increase in the total number of words from T1 to T2 (+186.25 words; 95% CI 144.41–228.1) and from T1 to T3 (+98.76 words; 95% CI 67.73–129.78). These shifts translate into percentage changes in the total number of words as follows: +82% from T1 to T2 and +44% from T1 to T3.
When examining changes in the proportion of each lexicon across time points, we observed T1–T2 increases in the Relaxing and analgesic experience (+1.00 point average, 95% CI 0.13–1.80), the Pleasant Place (+8.52 points, 95% CI 7.22–9.81), and the Magic Glove (+9.31 points, 95% CI 7.47–11.14). We observed decreases in Medical and procedure words (−2.24 points, 95% CI 1.65–2.83) and Negative experience (−3.12 points, 95% CI 2.41–3.82). These shifts translate into percentage changes in lexical content as follows: Relaxing and analgesic experience words +20%, Medical and Procedure words −73%, Negative experience words −51%, Pleasant Place technique words +260%, and Magic Glove technique words +582%. (Supplement Table S5 and Figure S2).
Furthermore, these initial findings suggested maintenance of these changes at T3, with T1-T3 5-month improvements in all but one lexicon index (Relaxing and analgesic experience: −.5 points, 95% CI -0.03–1.4). We observed increases in Pleasant Place (+6.30 points, 95% CI 4.97–7.62) and Magic Glove (+4.16 points, 95% CI 1.60–6.72) and decreases in Medical and Procedure words (−1.80 points, 95% CI 1.18–2.42%) as well as Negative experience (−2.01 points, 95% CI 1.16–2.86%). These changes translate into percentage changes in lexical content: Medical and Procedure words −32%, Negative experience words −58%, Pleasant Place technique words +188%, and Magic Glove technique words +260%.
Main results
For all outcomes, the results indicated that the non-linear LGCM models fit the data better than the linear models. Therefore, the non-linear models were retained for further analysis. (Fit indices and parameter estimates are available in Supplement Table S6). Figure 1 shows a visual summary of the results (The main results from the LGCM are available in Supplement Table S7). Graphical representation of the latent growth curve models (LGCM) results for the main results.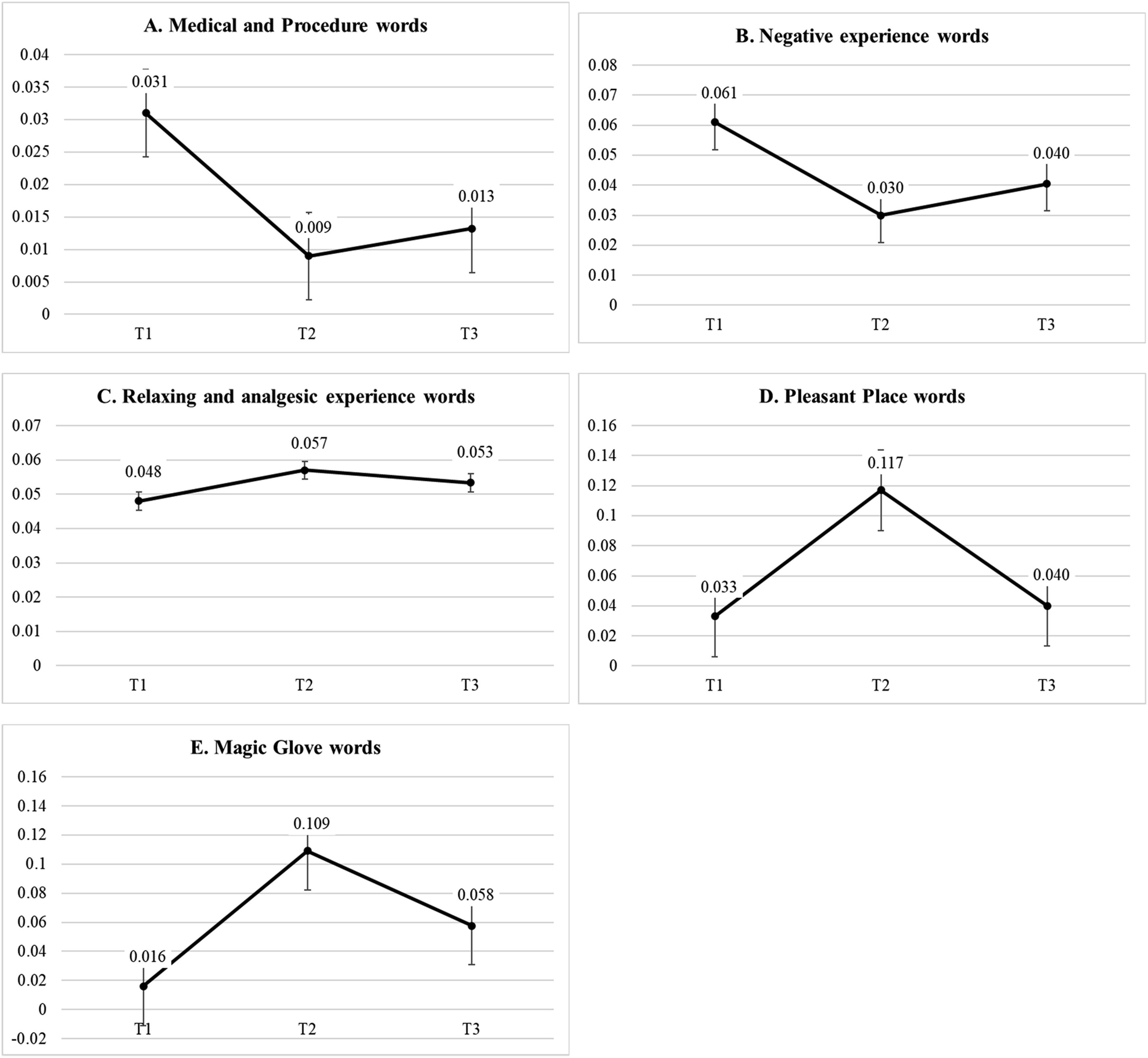
Total number of words
The findings suggest an increase in total words used by healthcare professionals (+184.72 words) from T1 to T2. At T3 (follow-up) this increase was maintained at a proportion of 52.7% and the number of words remained significantly higher than at T1. No significant variation was observed in the trajectory (slope) and no significant effect of the baseline (intercept) values on the trajectory was present. Similarly, no time-invariant predictors were associated with the intercept or the slope over time (all ps > .089).
Changes in lexical content
As expected, the findings suggested that the use of some categories of words decreased from T1 to T2 for the Medical and Procedure words (−2.00 points) (Figure 1 panel A) and the Negative experience words (−3.10 points) (Figure 1 panel B). These decreases remained at follow-up at a proportion of 81% and 66%, respectively. The analysis also revealed an increase in the use of Relaxing and analgesic experience words (+0.90 points) (Figure 1 panel C), Pleasant Place words (+8.40 points) (Figure 1 panel D), and Magic Glove words (+9.30 points) (Figure 1 panel E) from T1 to T2. These increases remained at follow-up at a proportion of 59%, 76%, and 45%, respectively. Notably, the Magic Glove lexicon results should be interpreted with caution, given the small number of participants. We found no effect of baseline (intercept) or variation in the trajectory (slope) for all but one lexicon. The only exception was for the Pleasant place, where the results indicated a significant variance in participants’ slopes (p < .001), suggesting that change could be greater for some participants.
Predictors
The following results were observed when exploring time-invariant predictors of the variability of the intercept and slope. For Medical and procedure words, gender emerged as a significant predictor of the slope, suggesting that the use of medical jargon or words related to medical procedures decreased more steeply among women than among men (B = −0.013, p = .030). For Negative experience, no effect was identified. For Relaxing and analgesic experience, a significant effect of seniority (years in hematology-oncology) on changes over time was identified, suggesting that changes were greater in participants with less experience (B = −0.001, p = .001). For Pleasant Place, we identified gender as a significant predictor of the intercept, meaning that before training, women tended to use a higher proportion of words related to the Pleasant Place lexicon compared to men (B = −0.024, p = .002). For Magic Glove, significant effects of seniority and profession on the slope were observed. Having less experience in hematology-oncology (B = −0.001, p = .008) and being a nurse (B = −0.031, p < .001) were associated with larger changes over time. In addition, nurses (vs physicians) tended to use more words related to the Magic glove lexicon before training (B = −0.020, p < .001). These results concerning the Magic Glove lexicon and gender should be interpreted carefully, given the small number of participants.
Additional analyses
After inclusion, participants had to be registered on a waitlist. For 11 participants, this gave us the opportunity to collect an additional baseline measure 1 week before T1, a time point we called T0. We calculated intraclass correlation coefficients to assess temporal stability between the two baseline measures, T0 and T1 (ICC, mean-rating absolute agreement, mixed effect). Across the five lexica, we observed a median ICC level of 0.748, suggesting a good stability in the absence of intervention. 33 Although the number of baseline measures here is limited to two, an examination of the graphical pattern of the trajectory for all available lexica in the 11 individual cases suggested that training was associated with changes in lexica above natural change (Supplement Figure S3).
Discussion
In this study, we examined how categories of words, or lexica, evolved after a hypnotic communication training in healthcare professionals. The results suggest that pediatric professionals who participated in the study used significantly different types of words after training and, more importantly, that a number of changes remained significant 5 months after the training. Specifically, healthcare professionals used fewer negative experience words after training, fewer medical words, or words related to the painful procedure and more relaxing and analgesia-laden words. They also used more words directly related to the hypnotic communication technique learned, either the Pleasant Place or the Magic Glove. These results are important for the evaluation of the effectiveness of the Rel@x training since the categories of words reflect the foundation of hypnotic communication in the verbal aspects. It has been shown that word meaning (e.g., using words of unpleasant content) can affect a patient’s pain experience.8,9,17–19,34,35 Along with some other elements, such as nonverbal and paraverbal communication, the changes observed in word categories favor the development of a trustful and collaborative relationship with patients.12,16,23 These changes also enhance patients’ receptivity to suggestion or imagery techniques. 36
We observed that, after training, a significantly lower proportion of words used by healthcare professionals during simulations related to negative experiences. Several studies9,19,35,37,38 have shown that using negatively charged words and suggestions, such as “pain,” “stress,” or “fear,” can negatively modify pain perception. Additionally, using minimizing words such as “try,” “probably,” and “maybe,” or the negation form such as “not to,” has been found to have no effect on moderating the effect of what is being said, 18 a fact that is consistent with the motivational priming theory. 10 To summarize, decreasing the focus on negative experiences in such a proportion in clinical encounters could alleviate patients’ painful experience.
Following training, healthcare professionals also tended to use less medical jargon. This may be particularly beneficial in the pediatric context, as medical jargon has been shown to be related to issues in understanding, hampering patient–provider collaboration, and thus negatively affecting health outcomes.39,40 Therefore, using less medical terminology promotes collaboration between patients and providers, which could mitigate the nocebo effects and promote adherence. Using less medical terminology could also translate to less painful experiences. 18
We also observed a significant rise in healthcare professionals’ use of relaxing and analgesic words following the training. This result is particularly important in regard to the patient’s adherence to the suggestions and imagery techniques. It also reflects communication about analgesia, a key aspect in hypnotic communication. 41 Research has supported that using positive cues (words such as “comfort,” “secure,” and “numb”) could minimize or reverse the nocebo effect. 42 This is consistent with the pain gate theory 11 stating that when presented simultaneously, two stimuli, one positive (i.e., the positive and/or analgesic suggestion) and one negative (i.e., the painful procedure), the positive stimuli will prevail. Hence, by using significantly more relaxing and analgesic words, healthcare professionals could again strongly mitigate the experience of pain.
As expected, the results showed that healthcare professionals used significantly more words relevant to the two communication techniques learned (i.e., Pleasant Place and Magic Glove), suggesting they used the technique they were trained to use. In essence, this is a procedure check of the training. The findings are original, though, as we observe a large proportion of maintenance of change in the longer term, 5 months after training. This suggests that healthcare professionals remembered the technique and/or practiced it without recall or additional supervision. It is particularly encouraging for future testing of hypnotic communication techniques.
When exploring explanatory factors for these results, we found that few of them contributed to variance in our sample. One result suggested that the female gender could play a role in using less medical jargon after training (but this result should be considered with caution because of the small number of men). This could reflect gender-specific attitudes toward empathy or pain-related communication in pediatrics. 43 In a critical review of the literature on the role of physician gender in communication style, Roter and Hall 30 have observed that female physicians tend to adopt a more patient-centered communication style, characterized by longer and more empathetic exchanges. Similarly, in a study examining the role of gender and ethnicity in caregiver–patient interactions, Peck and Denney 31 had found that women speak more during encounters with their patients, while men use a more physician-centered communication style. Studies have also shown that women pediatricians tend to use more complementary or alternative medicine in the healthcare setting than men. 32 Nevertheless, since very few men participated in the present study (10%), these results should be considered preliminary. Future studies should explore this phenomenon in detail.
Seniority appeared as the other factor contributing to change, where healthcare professionals with less specialized experience tended to increase their use of relaxing or analgesic words such as “exhale,” “calmly,” or “peaceful” in comparison with professionals with longer specialized experience. It is possible that professionals with more experience may have already developed their own strategies (i.e., embedded routines) to deal with pediatric pain and continue to use the words they are used to. 44 It could also be that more experienced professionals are less open to new techniques 45 or that they would require more training for other reasons. Another potential explanation is that younger professionals are particularly receptive or flexible as to these communication techniques. Finally, seniority could also influence how professionals value changing what they say to patients, a factor that has been identified as essential for change. 46
In most cases though, we could not identify any factors accounting for variability in lexical change. This was particularly notable for words relevant to hypnotic communication techniques. For the Pleasant Place, although significant variability was found, none of the measures tested could account for this result. In this case, we can hypothesize that many unmeasured factors could account for this result, such as levels of motivation to use a technique, confidence in using the given technique, or personal experience, warranting further examination.
It is unlikely that the proportion of categories of words as operationalized here would evolve naturally over time. In the present study, we could make use of two baseline time points in a subgroup of participants. The results suggested a relative stability across lexica without training, further reinforcing the observation that a significant portion of the changes observed could be related to the training. This baseline stability, although in very small sample, also suggests that a “no training” condition could be a comparator in future studies aiming to evaluate the training.
This study is the first to reliably measure the lexical content of trainees following a hypnotic communication training targeting the pain experience. One interesting feature was the use of systematic categories of words. Once the sets of words are defined, determining the frequency of each lexicon means counting objectively a set of words. This involves no further human action. It is thus a potentially powerful and reliable technique. In our field, it could be an alternate approach to existing coding schemes to evaluate hypnotic communication.22,47 In this regard, future studies may even be conducted with automated identification and coding (i.e., some robust programs exist, such as the Linguistic Inquiry and Word Count and the French-language “Analyseur Lexico-Syntaxique Intégré,” but are yet not fully adapted for all languages).48–50 From a clinical point of view, this study adds to the potential impact of hypnotic communication training in pediatrics. Although it was not the purpose of this study, we could foresee that the changes in lexical content could well facilitate the mitigation of the pain experience. Future studies should address this important issue. Another potential avenue would be to study paraverbal characteristics that may change in such communication training, such as speech rate or prosody.
We should recognize the limitations of this study. Firstly, this is an exploratory descriptive study that did not use a control group. In that sense, we cannot attribute lexical changes to the training with certainty. Arguments in favor of the effect of training lie in changes relevant to specific hypnotic communication techniques (e.g. the Pleasant Place) and relative stability in baseline analyses. Some results should also be considered preliminary in the main analyses, as small subgroup sizes could have affected the reliability of results. This is the case of the group receiving the Magic Glove training (n = 8), the small number of participating physicians (n = 4), and more generally men (n = 6). We also recognize that there may be a recruitment bias since participants registered voluntarily. Those who participated could be more open and interested in changing their communication style with patients. Finally, it is a core result that changes in lexical contents persist in the long-term (i.e., participants used different words), during a standard venipuncture. Yet, maintenance of change was hard to interpret as we did not have access to data on the practice of hypnotic communication between the end of training and follow-up.
Conclusion
In a secondary analysis of video-recorded simulations of a venipuncture before, after, and at a 5-month follow-up after a hypnotic communication training, we observed significant changes in the words used by participants. Participants used fewer words associated with negative experiences, medical jargon, and procedures but more words related to relaxation, pain relief, and hypnotic techniques. These changes remained significant at follow-up, suggesting successful acquisition of the skills and potential use of the techniques in participants’ everyday work. When exploring factors contributing to increased change, we identified having less professional experience as a potential factor This study suggests that the content of communication is modified following a short hypnotic communication training. This study exemplifies an alternate way of coding communication content to evaluate communication among healthcare professionals.
Supplemental Material
Supplemental Material - How professionals in pediatrics change the words they use to mitigate pain: A lexical description after a short hypnosis-based communication training
Supplemental Material for How professionals in pediatrics change the words they use to mitigate pain: A lexical description after a short hypnosis-based communication training by M. Bedu, D. Ogez, J. Aramideh, B. Bőthe, A. Levesque, E. Rondeau, A.-F. Tessier, M. Duval, and S. et Sultan in British Journal of Pain.
Footnotes
Acknowledgments
The research team is most grateful to the healthcare teams of the Centre Hospitalier Universitaire Sainte-Justine who facilitated access of their personnel to the training. We also deeply thank the patient partners who helped us with data collection and interpretation: Ariane Lacoste-Julien, Mathias Tyo-Gomez. We thank all research personnel involved in data collection. We are grateful to Claude-Julie Bourque, Christian Dagenais, Jocelyn Gravel, Andrea Laizner, Sylvie Le May, Ahmed Moussa, and Argerie Tsimicalis for their help in securing funding and facilitating access to participating professionals.
Ethical considerations
Ethical approval was granted by the CHU Sainte-Justine Research Ethics Board (#2019-2205) and the research was conducted according to the principles expressed in the Declaration of Helsinki. All participants provided written informed consent.
Authors’ contributions
Conception: MB, DO, MD, SS
Design: MB, DO, BB
Data acquisition and analysis: MB, DO, JA, AL, ER, AFT, MD, SS
Interpretation of data: MB, DO, JA, BB, AL, ER, AFT, MD, SS
Drafting: MB, SS
Revision: MB, DO, JA, BB, AL, ER, AFT, MD, SS
All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the FRQs-Oncopole, Grant #302025 (year 2020). The funder had no specific role in the conceptualization, design, data collection, analysis, decision to publish, or preparation of the manuscript. BB was supported by the FRQSC – Research Support for New Academics (NP) Program. AL is a recipient of the Doctoral Research Award from the Canadian Institutes of Health Research (CIHR).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.