
Abstract
Background
Elective lumbar spine surgery is increasingly being implemented to treat patients with specific low back pain. However, approximately 30% of patients continue to have long-term pain and disability after surgery.
Objective
The aim of this study was to systematically review the literature on the effectiveness of pre-surgical rehabilitation (prehab) alone or in combination with usual care versus usual care on patient-oriented outcomes and health-related costs following elective lumbar spine surgery.
Data sources
Electronic databases from MEDLINE, CINAHL, EMBASE, and AMED were systematically searched from their inception to November 2022.
Study selection
Randomized controlled trials that examined adult (age >18 years) prehab programs and evaluated one or more outcomes of interest were included in this review.
Data extraction
In pairs, six reviewers independently conducted a risk-of-bias assessment and extracted outcome data from included studies, in accordance with the Template for Intervention Description and Replication (TIDieR). A meta-analysis was conducted when trials were homogeneous.
Data synthesis
A total of eight trials (n = 739 participants), reported in 13 different manuscripts, were eligible for inclusion. Exercise prehab interventions are superior to usual care for disability at 3-month (MD: −2.56, 95% CI −4.98 to −0.15), back pain at 6-month (MD: −6.65, 95% CI −13.25 to −0.05), and health-related costs (MD: €2572.8, 95% CI: €1963.0 to €3182.5). CBT prehab interventions seem to be superior to usual care for back pain at 3-month (MD: −7.3, 95% CI: −14.5 to −0.05). Individual trials showed that education prehab interventions may be superior to usual for back pain at 1-month post-operative (MD: 12.3, 95% CI: 0.9 to 23.7).
Limitations
Overall, the inclusion of heterogeneous trials (e.g., diagnosis, types of surgery, dosage, content, and duration of interventions) with small sample sizes leads to inconclusive and very low certainty of effect estimates.
Conclusion
The present systematic review has brought to light the dearth of high-quality evidence in support of prehab interventions for patients undergoing lumbar spine surgery. Given the uncertainty surrounding the results obtained from low-quality randomized controlled trials, it is currently not feasible to provide recommendations for clinical practice.
Introduction
Low back pain (LBP) is the leading cause of years lived with disability worldwide, contributing to significant personal, economic, and societal burdens.1–3 Current clinical practice guidelines recommend conservative treatments consisting of exercise therapy, psychosocial interventions, self-management, and epidural steroid injections as the first line of care.4–6 Elective spine surgery is usually recommended for individuals with LBP with severe disabling symptoms or when conservative management has failed.4,7 Surgical procedures can include microdiscectomy, laminectomy, and spinal fusion, among others.4,7 Microdiscectomy and laminectomy are used to relieve pressure on a nerve root by removing the impeding bone or disc material. 4 These procedures are generally performed in populations with a herniated disc or lumbar spinal stenosis. 4 Spinal fusion involves inserting a bone graft with or without implants to relieve painful spinal segments and improve segmental stability. Spinal fusion is usually indicated for degenerative disc disease, or alongside extensive decompression. 4
Although there has been a steady rise in the number of elective LBP surgeries performed, approximately 30% of post-surgical LBP patients continue to have long-term pain and disability.8–11 Previous studies have identified body weight, muscle strength, walking capacity, smoking status, baseline pain, and other psychosocial factors to be predictors of poor post-surgical pain and disability outcomes.11–15 It has been suggested that prehabilitation (prehab) programs delivered in the weeks prior to surgery have the potential to positively modify prognostic indicators such as walking capacity, body weight, and psychosocial factors, and improve individuals’ pain intensity and disability post-surgically.16,17 Specific examples of prehab interventions may include functional and resistance exercises, motor control training, patient education, or cognitive behavioural therapy (CBT), all of which may be implemented within individual or group formats.16,17
As prehabilitation for individuals undergoing spinal surgery has gained popularity, 18 two systematic reviews (search up to 2016 and 2017) and one scoping review have been published..19–21 The most recently published review (2023) was a scoping review 19 that described the types of prehab interventions without focusing on their effectiveness. Thus, given the growing popularity of prehabilitation interventions among individuals undergoing spinal surgery, a more robust, accurate, and updated analysis based on RCTs needs to be conducted to inform patients, clinicians, researchers, and stakeholders of the best evidence regarding prehab for individuals with LBP undergoing spinal surgery.
Therefore, this study aims to systematically review the literature on the effectiveness of prehab versus standard care on pain, disability, function, health-related quality of life (HRQoL), and health-related costs following elective lumbar spine surgery.
Methods
The protocol for this systematic review was prospectively registered (registration number: CRD42020175059) with the International Prospective Register of Systematic Reviews (PROSPERO). 22 We used the Cochrane Back Review Group guidelines to conduct this systematic review and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for reporting.23,24
Data sources and searches
We searched the following electronic databases from their initial issues to February 2020: MEDLINE via Ovid (1946 - February 2020), CINAHL via EBSCO (1981 - February 2020), EMBASE via OVID (1974 - February 2020), and AMED via OVID (1985 - February 2020). Our search was updated in November 2022. No language or data restrictions were implemented. Search strategies for each database can be found in Appendix 1. We consulted a university librarian to build a comprehensive search strategy. We also performed citation tracking by checking the reference list of all primary studies and previous systematic reviews on this topic as well as by using the Web of Science citation tracking tool.
Study selection
In pairs, reviewers (J.V., J.S., S.R., S.I., N.I., A.C., L.A., D.R., and N.B.) screened initial search results based on titles and abstracts. All reviewers completed a pilot screen of 10 randomly selected search results to ensure a consistent understanding of eligibility criteria. The same reviewers then performed full-text screening in pairs. Disagreements regarding study inclusion were resolved through discussion and consultation with a senior third reviewer (L.M.). Study selection was completed using the Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia). A list of excluded studies with reasons can be found in Appendix 2.
Participants
Only RCTs were included in this systematic review. Studies were eligible if they included adult participants (i.e., age >18 years), who underwent elective surgery to treat specific LBP (e.g., lumbar spine stenosis, radiculopathy, spondylolisthesis, disc herniation, etc.). Serious pathologies such as trauma, infection, or cancer were not eligible for inclusion, given the complexity of care and difficulty in controlling additional bias. 25 This review did not restrict studies based on the type of surgery.
Interventions
Studies were included if they examined prehab programs for lumbar spinal surgery versus any control group. Prehabilitation was defined as any intervention predominately composed of exercise, education, cognitive behavioural therapy (CBT), self-management, or a combination of these techniques delivered prior to surgery. Education on pre- and post-operative (post-op) hygiene, lifestyle changes, exercise recommendations, and self-management were eligible. Studies that included only one session of education were excluded as they were not deemed to be a program of care and were not enough to produce long-lasting changes post-operatively. For this review, we included studies that compared prehab interventions alone or associated with usual care against usual care. Usual care was defined as no specific treatment offered by the trial, which includes a waitlist group, control group, or standard care provided prior to elective lumbar spine surgery, but not controlled by the study.
Outcomes
Studies were included if they assessed patient-centred and health-economic outcomes, including post-op pain intensity, physical function or disability status, walking capacity, Health-related Quality of Life (HRQoL), length of hospital stay, and/or health-related costs. Follow-up times were classified as short-term (i.e., <3 months after surgery), intermediate-term (i.e., >3 and <6 months), and long-term (i.e., >6 months) from the time of surgery. We gave preference to the longest time point within each follow-up time.
Quality assessment and data extraction
Risk of bias for each study was individually assessed using the Cochrane Back Review Group’s Risk of Bias Tool 2.0, which includes five grading domains.26,27 Any disagreements between pairs of reviewers were resolved via discussion and consultation with a senior third reviewer (L.M.). Each domain was labelled as having ‘high’, ‘low’, or ‘some’ risk of bias according to the domain-specific algorithms outlined within the tool. 27 The overall quality of evidence for each outcome was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.27,28 We used the five GRADE considerations (i.e., study limitations, inconsistency, imprecision, indirectness, and publication bias) to assess the quality of evidence as high, moderate, low, or very low. 26 We also used the Template for Intervention Description and Replication (TIDieR) for reporting of complex interventions. 29
Prior to full-text screening, risk of bias assessment, and data extraction, a set of three papers were used to calibrate reviewers. A standardized extraction form was used by assessors to extract data from each included study. Data extraction was also completed independently in pairs. Disagreements were resolved via discussion and consultation with a senior third reviewer (L.M.). Reviewers extracted authors’ names, year of publication, participants’ information (e.g., age, sex, type of surgery, diagnosis, and prehab vs control group, etc.), intervention and comparison protocol, outcome measures selected, and findings. The TIDieR checklist was used to collect the reporting of interventions. 29 Sample size, mean, and standard deviations were extracted for continuous data. The Cochrane Handbook was used to estimate values when outcome data were not available. 26 In cases of missing outcome data, we contacted the respective authors to collect the requisite raw outcome data. In the case of non-responsive authors, missing data was omitted. 26
Data synthesis and analysis
Study characteristics and summary results data were presented qualitatively in tables. All pain and disability scores were converted to a 100-point scale and reported as mean differences (MD) with 95% CI as conducted on previous systematic reviews of LBP. 30 For the other continuous outcomes which were measured in different units across trials, we reported their pooled results, when available, by calculating standardized mean differences (SMD) and expressing uncertainty via 95% confidence intervals (CI). Statistical heterogeneity was assessed by calculating the I2 of pooled studies, and statistically unimportant heterogeneity (i.e., statistical homogeneity) was defined as I2 < 50%.26,31 Where trials were sufficiently homogenous based on interventions, outcome measures, timelines, and an I2 value less than 50%, a meta-analysis was conducted on Cochrane RevMan 5.3 (London, United Kingdom) using a random effects model.
Results
Search outcomes
The database search yielded 13,768 studies in addition to one study identified through hand search (Figure 1), and 12,028 after removal of duplicates. In total, 72 full texts were screened for eligibility (11,948 were excluded). A total of eight trials, reported in 13 different manuscripts,32–44 met the inclusion criteria for this systematic review. Reasons for exclusion were not including a prehab program, inappropriate study design, inappropriate population or outcomes, and being a duplicate reference (see Appendix 2 for a list of excluded studies with reasons). All 13 trials were included in the qualitative analysis, and five were included in the quantitative analysis. Prisma flow diagram. Flow diagram of systematic review and meta-analysis inclusion and exclusion of articles for prehabilitation prior to elective lumbar spine surgery.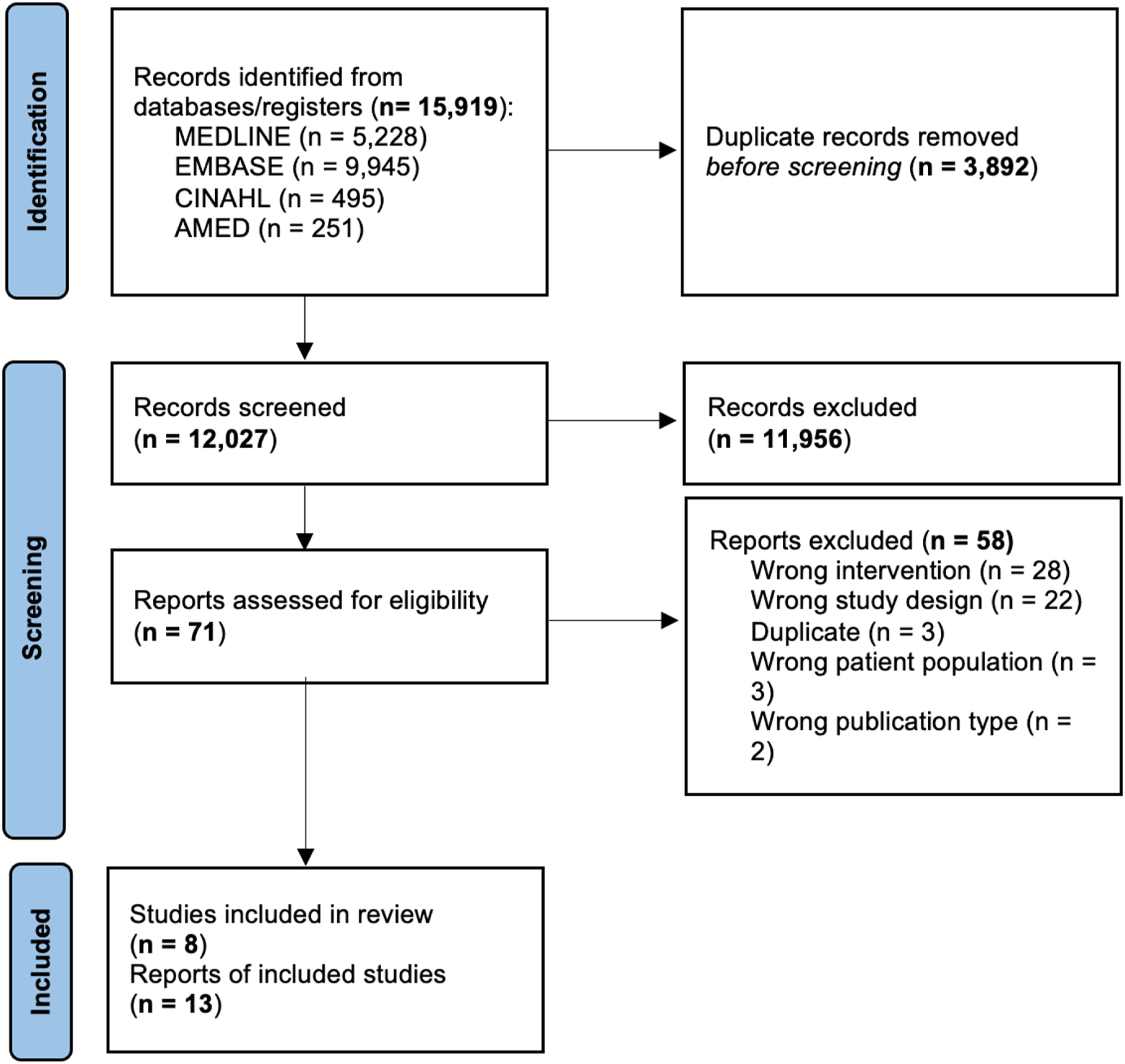
Addressing Missing data Authors from one included study were contacted via email for additional data pertaining to outcomes at predetermined time points. However, the additional data was not received. In accordance with the Cochrane Handbook, this data was omitted. 26
Study characteristics
Summary of study characteristics.
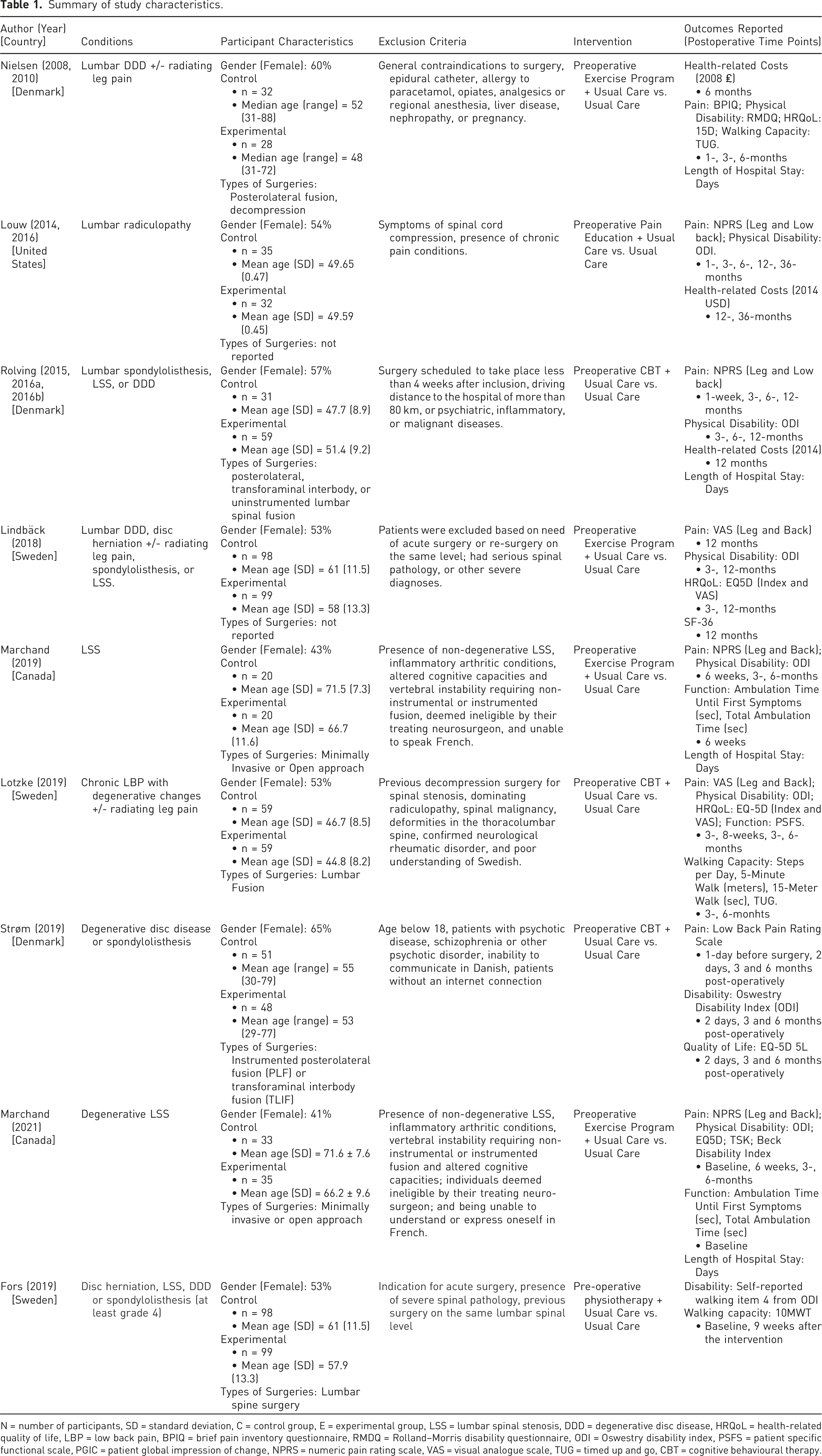
N = number of participants, SD = standard deviation, C = control group, E = experimental group, LSS = lumbar spinal stenosis, DDD = degenerative disc disease, HRQoL = health-related quality of life, LBP = low back pain, BPIQ = brief pain inventory questionnaire, RMDQ = Rolland–Morris disability questionnaire, ODI = Oswestry disability index, PSFS = patient specific functional scale, PGIC = patient global impression of change, NPRS = numeric pain rating scale, VAS = visual analogue scale, TUG = timed up and go, CBT = cognitive behavioural therapy.
Intervention characteristics.
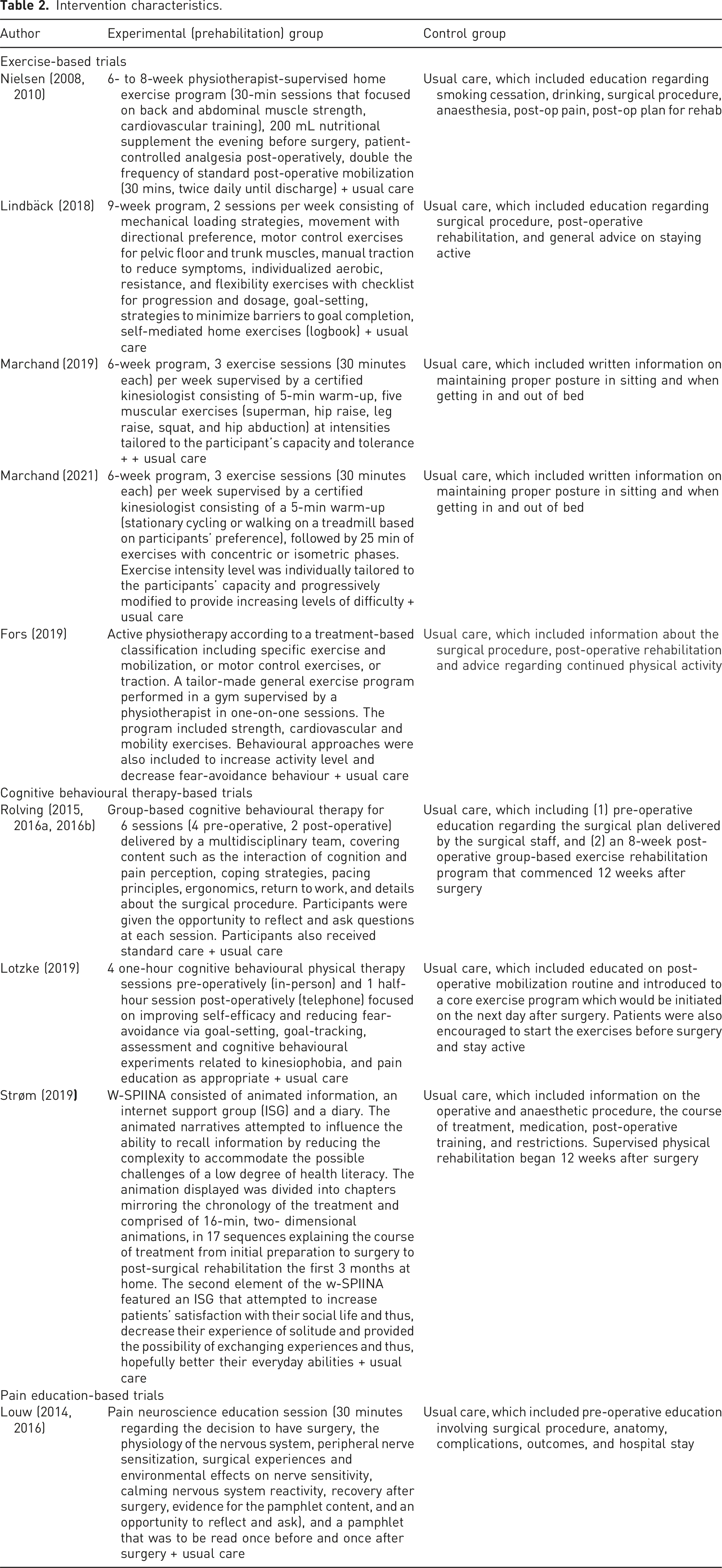
Indications for surgery included lumbar disc degeneration, lumbar disc herniation with radiating leg pain,33,34,39–43 severe lumbar radiculopathy,35,36 or lumbar spinal stenosis with radiculopathy,33,37 spondylolisthesis (grade 1–2), 33 degenerative disc disease or spondylolisthesis, 44 or degenerative lumbar spine stenosis. 38 Types of surgeries included posterolateral, transforaminal, or uninstrumented lumbar spinal fusion surgeries,34,40 spinal stenosis surgeries via a minimally invasive or open approach,37,38 instrumented posterolateral fusion or transforaminal interbody fusion, 44 and decompression. 40
Outcomes reported across studies included back pain and leg pain reported using visual analogue scale (VAS) or numeric pain rating scale (NPRS), disability using the Oswestry Disability Index (ODI) or the Rolland–Morris Disability Questionnaire (RMDQ), Health-related Quality of Life (HRQoL) using EuroQol-5D (EQ-5D) or the 15D instrument. Details regarding additional relevant outcome measures and time points are reported in Table 1.
Quality assessment
Risk of Bias Tool 2.0 assessment for each study is presented in Appendix 4. Assessments were performed per-manuscript (n = 13) as opposed to per-trial (n = 8) as methods employed were different at long-term follow-ups. This difference mainly arose from the use of varying methods to address loss to follow-up (e.g., intention-to-treat vs per-protocol) or reporting bias with the omission of pre-specified outcomes. Six manuscripts were scored as having a low risk of bias,32,33,35,36,42,43 six were scored as having some risk of bias,32,34,37–40,44 and one was scored as having a high risk of bias. 41 All manuscripts had a low risk of bias in randomization and allocation concealment.
Treatment effects
Treatment effects are presented based on comparisons and outcomes of interest. The results of individual studies (mean differences and CI) for all outcomes and time points are tabulated in Appendix 5.
Prehab exercise interventions plus usual care versus usual care
Back pain
Three trials (four manuscripts)37–40 compared prehab exercise plus usual care against usual care and reported back pain outcomes. Pooled results of three trials37,38,40 demonstrated very low certainty of evidence (downgraded due to risk of bias, inconsistency, imprecision, and publication bias) that there is no statistically significant difference between prehab exercise plus usual care and usual care on back pain at 3 months (MD: −2.3, 95% CI −8.86 to 4.26, n = 153) (Figure 2). At 6 months, however, there is very low certainty of evidence (downgraded due to risk of bias, inconsistency, imprecision, and publication bias) that there is a small effect favouring prehab exercise plus usual care (MD: −6.65, 95% CI: −13.25 to −0.05, n = 153) compared to usual care alone (Figure 2). Prehabilitation versus standard care effects on back pain (100-point VAS). Forest plot displaying the effects of exercise- and CBT-based prehabilitation on back pain at 3- and 6-month post-operative follow-up, measured by 100-point visual analogue scale.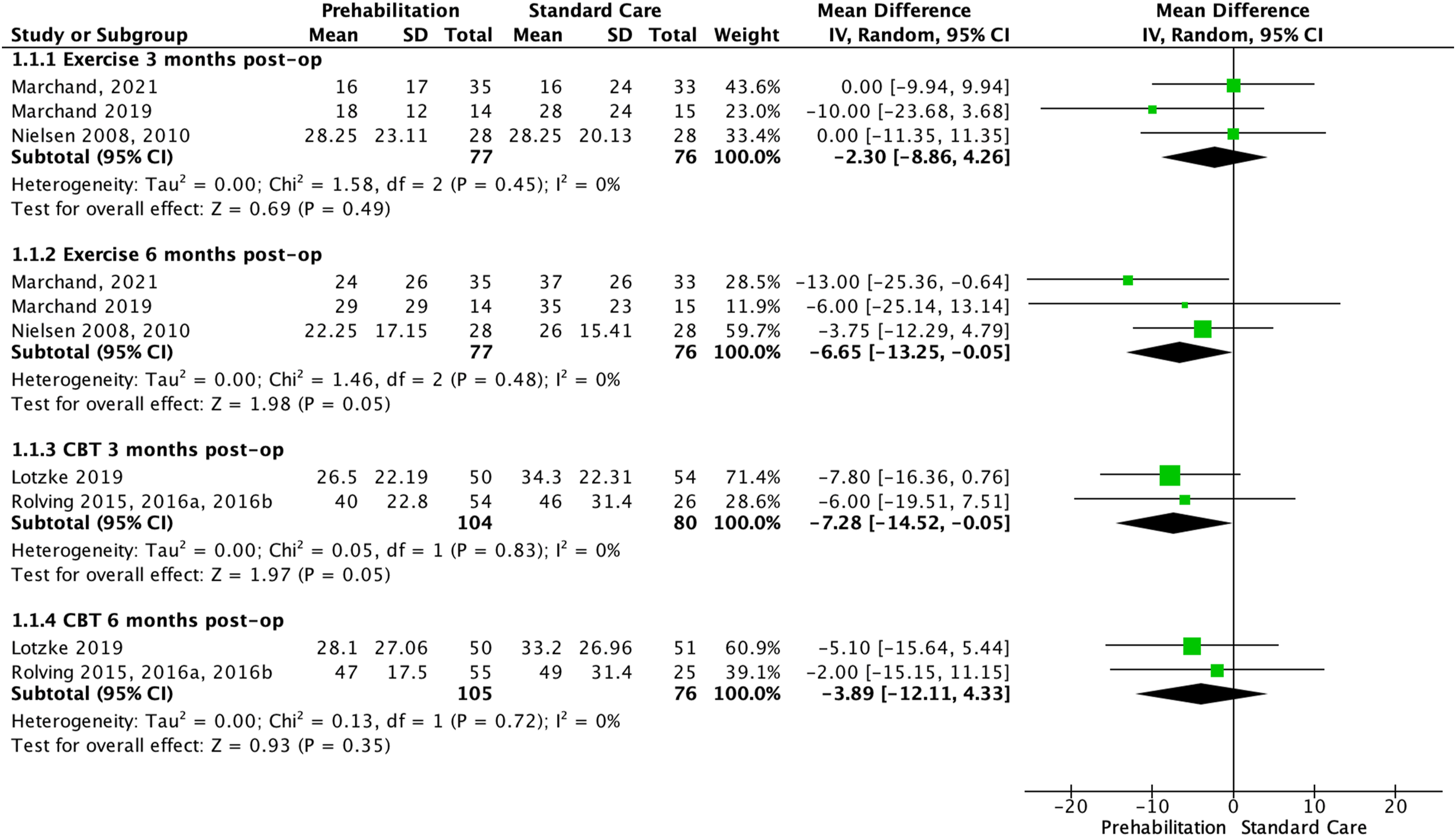
Leg pain
Three prehab exercise trials (four manuscripts)38–40 compared prehab exercise plus usual care against usual care on leg pain. Pooled results of the three trials37,38,40 found very low certainty of evidence (downgraded due to risk of bias, inconsistency, imprecision, and publication bias) of no statistically significant difference between prehab exercise plus usual care and usual care only at 3 (MD: 4.37, 95% CI −3.42 to 12.16, n = 153) and 6 months (MD: −6.31, 95% CI −15.29 to 2.67, n = 153)37,38,40 (Figure 3). Prehabilitation versus standard care effects on leg pain (100-point VAS). Forest plot displaying the effects of exercise- and CBT-based prehabilitation on leg pain at 3- and 6-month post-operative follow-up, measured by 100-point visual analogue scale.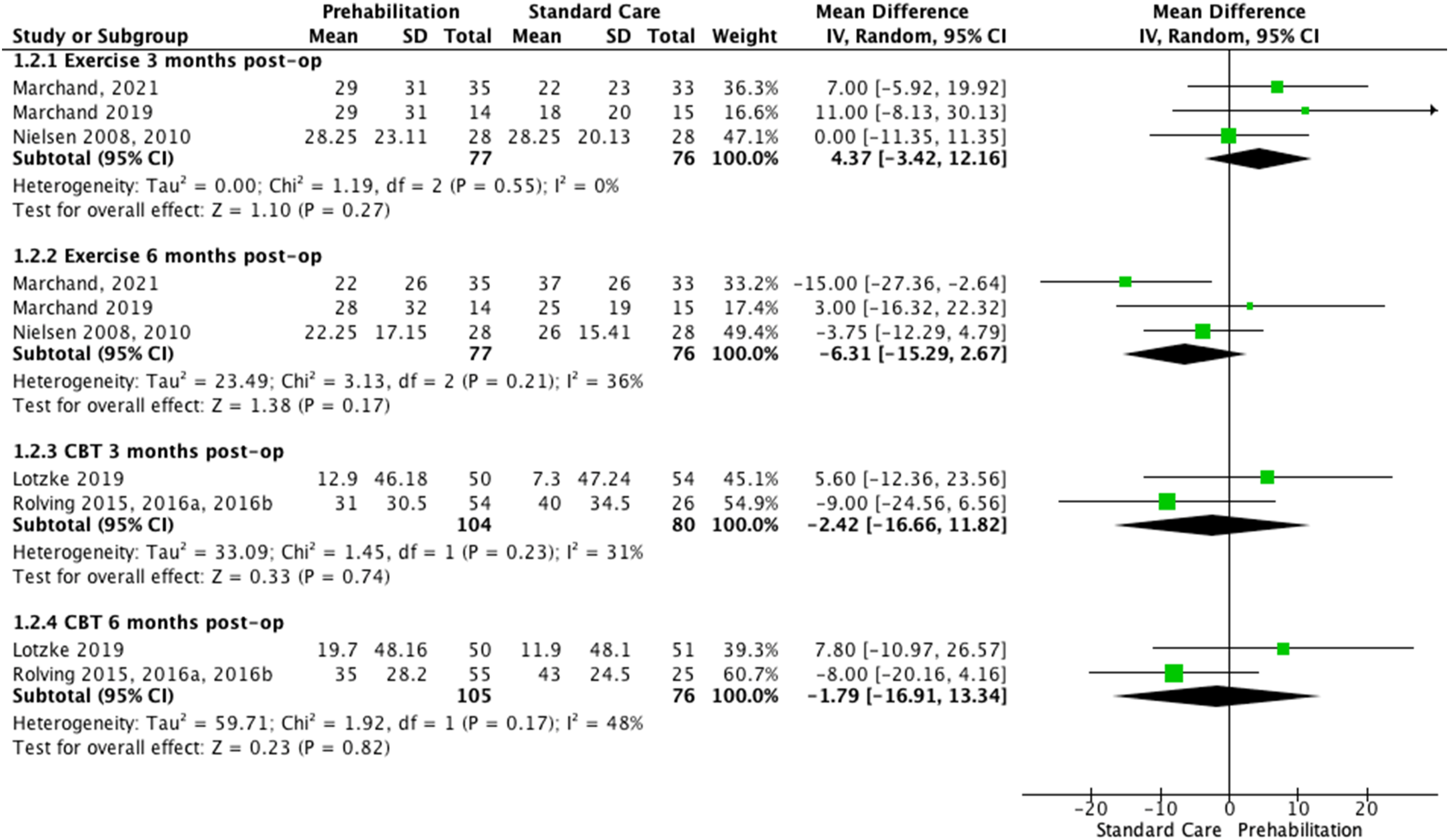
Physical disability and function
Four exercise trials (five manuscripts)33,37–40 comparing prehab exercise plus usual care against usual care reported disability outcomes. Pooled physical disability results found very low certainty evidence (downgraded due to risk of bias, imprecision, and publication bias) of a small statistically significant difference favouring prehab exercise intervention plus usual care against no usual care at 3 months (MD: −2.56, 95% CI: −4.98 to −0.15, four trials, n = 307), but not at 6 months (MD: −5.48; 95% CI −11.55 to 0.60, three trials, n = 128) (Figure 4). Exercise prehabilitation versus standard care effects on self-reported physical disability. Forest plot displaying the effects of exercise-based prehabilitation on self-reported physical disability at 3- and 6-month post-operative follow-up, measured by the Oswestry disability index or Rolland–Morris disability questionnaire.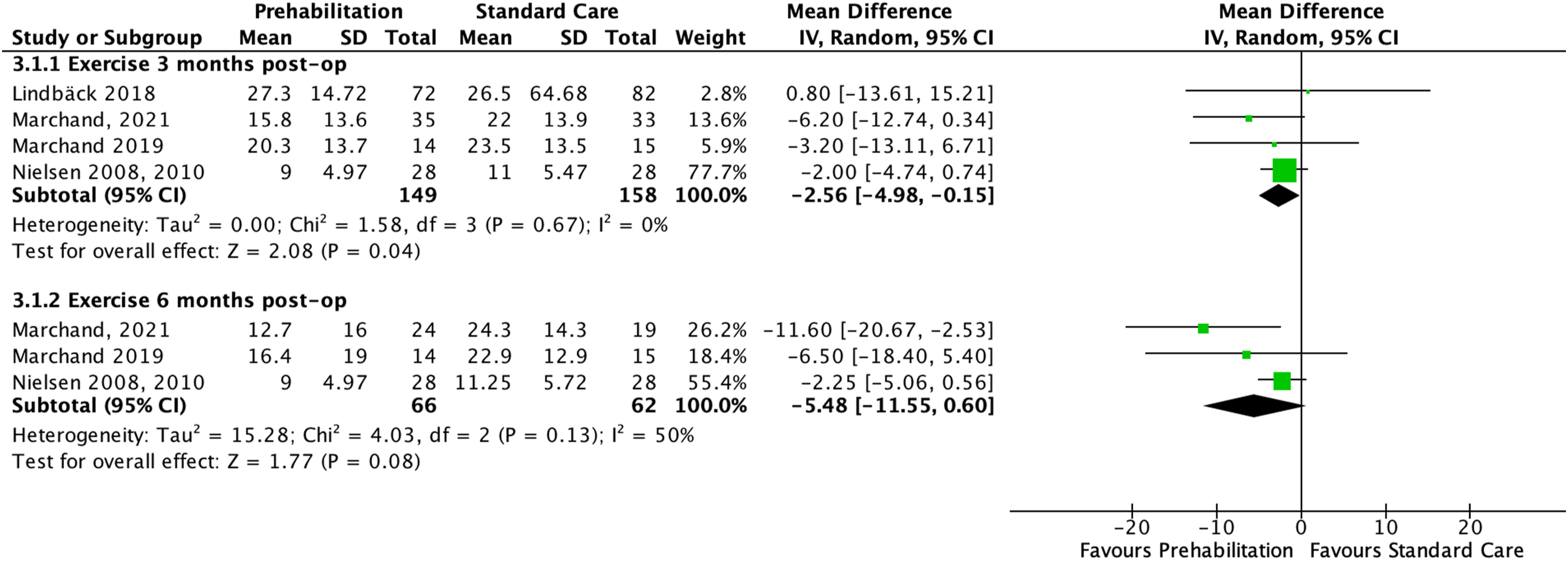
Walking capacity
One individual trial of prehab exercise plus usual care versus usual care assessed walking capacity as the ambulation time prior to the onset of symptoms and the total ambulation time (with or without symptoms) immediately post op and at 6 weeks post-op. 38 Results from this trial found very low certainty of evidence (downgraded due to risk of bias, imprecision, and publication bias) of no statistically significant differences between groups post-surgery (MD: 23.5, 95% CI −41.39 to 88.39, one trial, n = 51).
Health-related quality of life
HRQoL was reported in two prehab exercise trials.33,40 Pooled results from these two trials33,40 at 3 months post-op (n = 210) found very low certainty evidence (downgraded due to risk of bias, imprecision, and publication bias) of no difference between the pre-operative exercise interventions plus usual care and usual care alone (MD: −0.14, 95% CI −0.51 to 0.23, two trials, n = 210) (Figure 5). Exercise prehabilitation versus standard care effects on health-related quality of life. Forest plot displaying the effects of exercise-based prehabilitation on health-related quality of life at 3-month post-operative follow-up, measured by the EQ-5D or 15D questionnaire.
Length of hospital stay
Length of hospital stay was reported in two prehab exercise trials.37,40 Results from these exercise trials were not pooled due to statistical heterogeneity (I2 = 75%). One individual trial (n = 40) demonstrated very low certainty evidence (downgraded due to risk of bias, imprecision, and publication bias) and suggested no significant differences in length of stay between a pre-operative exercise plus usual care and usual care alone. 37 In contrast, another individual trial (n = 60) showed very low certainty evidence (downgraded due to risk of bias, imprecision, and publication bias) that the length of stay was statistically significant lower in the prehab exercise intervention plus usual care than usual care alone (MD: 3.0 days, 95% CI: 2.0 to 4.0 days). 40
Health-related costs
Two trials39,40 (one manuscript, n = 60) reported health-related costs. We found very low certainty evidence (downgraded by risk of bias, inconsistency, imprecision, and publication bias) that healthcare costs were significantly lower in the prehab exercise plus usual care compared usual care 6 months after surgery (MD: €2572.8, 95% CI: €1963.0 to €3182.5), but no statistically significant differences were found 1 year after surgery. 39
Prehabilitation CBT interventions plus usual care versus usual care alone
Back pain
Two CBT trials (four manuscripts)34,41–43 comparing prehab CBT plus usual care against usual care reported back pain outcomes. Pooled results found very low certainty of evidence of a small effect (downgraded due to risk of bias, imprecision, and publication bias) favouring prehab CBT plus usual care at 3 months (MD: −7.3, 95% CI: −14.5 to −0.05, two trials, n = 184). At 6 months, however, there is very low certainty of evidence (downgraded due to risk of bias, imprecision, and publication bias) that there is no statistically significant difference between pre-operative CBT plus usual care and usual care alone(two trials, n = 181) (Figure 2).
Additionally, an individual trial 34 reported back pain at 1 month only and demonstrated very low certainty evidence (downgraded by imprecision and publication bias) of a small effect favouring the prehab CBT group at 1-month post-op (MD: 16.3, 95% CI: 7.0 to 25.5, one trial, n = 118) compared to usual care.
Leg pain
Pooled results from the prehab CBT trials35,41,42 on leg pain showed very low certainty of evidence (downgraded due to risk of bias, imprecision, and publication bias) of no statistically significant differences between prehab CBT plus usual care and usual care alone at 3 (n = 184) or 6 months (n = 181) post-op (Figure 3).
Moreover, an individual trial 34 reported leg pain at 1 month only and showed very low certainty evidence (downgraded by imprecision and publication bias) of a small effect in favour of prehab CBT group at 1-month post-op (MD: 16.3, 95 CI%: 7.0 to 25.5, n = 118) compared to usual care.
Physical disability & function
Two CBT trials (three manuscripts)34,41,42 reported physical disability using the ODI scores. Results from CBT trials46,47 at 3- and 6-months post-op were not pooled due to statistical heterogeneity (I2 = 75–90%). There is very low evidence (downgraded by risk of bias, inconsistency, imprecision, and publication bias), based on one trial (n = 90), 46 which found a small statistically significant reduction in favour of the prehab CBT intervention at 3 months (MD: 16.1, 95% CI: 8.2 to 24.0) and 6 months (MD: 14.1, 95% CI: 7.6 to 20.7). However, the other trial (n = 118) found very low evidence (downgraded by risk of bias, inconsistency, imprecision, and publication bias) of no difference between groups at 3- (MD: 0.04, 95% CI −0.34 to 0.43) and 6-month (MD: −0.16, 95%CI −0.55 to 0.23) follow-ups. 34
An individual trial (n = 118) assessed function using the Patient Specific Functional Scale, and compared a prehab CBT physiotherapy intervention plus usual care versus usual care alone. There is very low evidence (downgraded by risk of bias, inconsistency, imprecision, and publication bias) of no statistically significant differences between groups at 3 (MD: 0.30, 95% CI −10 to 0.70) and 6 months (MD: 0.17, 95% CI −0.25 to 0.59) after surgery. 48
Walking capacity
Four trials (two manuscripts)34,41–43 of prehab CBT plus usual care versus usual care assessed walking capacity using different measures at 3- and 6-months post-op. Results from an individual study (n = 118) showed very low certainty of evidence (downgraded by risk of bias, inconsistency, imprecision, and publication bias), suggesting no statistically significant differences between a prehab CBT intervention plus usual care versus usual care on steps per day at 3- (MD: −0.09, 95% CI −0.50 to 0.32) and 6-month post-op (MD: 0.25, 95% CI −0.16 to 0.66), on 5-min walk distance at 3 (MD: 0.05, 95% CI −0.35 to 0.45) and 6-month post-op (MD: 0.0, 95% CI −0.4 to 0.41), and on 15-m walk time at 3- (MD: −0.04, 95% CI −0.44 to 0.36) and 6-months post-op (MD: −0.12, 95% CI −0.53 to 0.28). 34
In contrast, another individual trial (n = 90) presented a very low certainty evidence (downgraded by risk of bias, inconsistency, imprecision, and publication bias) of a statistically significant higher steps per day (MD: 1000.9 steps, 95% CI: 153.4 to 1848.4) and 5-min walk distance (MD: 135.2 m, 95% CI: 67.8 to 202.7 m) in favour of the prehab CBT intervention plus usual care at 6 months post-op when compared to usual care alone. 41
Timed up and go (TUG)
TUG scores (seconds) were reported in one prehab CBT trial (n = 118). 34 There is very low certainty of evidence (downgraded by risk of bias, inconsistency, imprecision, and publication bias) suggesting no statistically significant difference between a prehab CBT intervention plus usual care and usual care alone at 3- (MD: 0.19, 95% CI −0.21 to 0.59) and 6-months (MD: 0.05, 95% CI −0.35 to 0.46).
Length of hospital stay
Length of stay was reported in only one prehab CBT trial (n = 90), in which very low certainty evidence (downgraded due to risk of bias, imprecision, and publication bias) of no significant difference between the pre-operative CBT plus usual care and usual care alone was found. 42
Health-related quality of life
HRQoL was reported by one CBT trial only 34 (n = 118) This CBT trial showed very low certainty evidence (downgraded due to risk of bias, imprecision, and publication bias) of small statistically significant improvements in the EQ-5D at 8 weeks post-op in favour of the prehab CBT intervention plus usual care compared to usual care alone (MD: 0.09, 95% CI: 0.01 to 0.17). 34
Prehabilitation pain education intervention plus usual care versus usual care alone
Back pain
One pain education trial (two manuscripts)35,36 comparing prehab pain education plus usual care against usual care reported back pain outcomes. This individual trial (n = 67) demonstrated very low certainty evidence (downgraded due to imprecision and publication bias) of a small statistically significant difference in back pain (MD: 12.3, 95% CI: 0.9 to 23.7) in favour of the prehab pain education intervention at 1-month post-op. 35
Leg pain
One pain education trial (two manuscripts35,36 comparing prehab pain education plus usual care against usual care reported leg pain. This individual trial (n = 67) found very low certainty evidence (downgraded due to imprecision and publication bias) of a small statistically significant difference in leg pain (MD: 14.5, 95% CI: 2.2 to 26.8) favouring the prehab pain education intervention at 1-month post-op. 35 They also showed very low certainty evidence (downgraded due to imprecision and publication bias) of a significant improvement favouring the prehab pain education intervention in leg pain at 3 years post-op (MD: 5.9, 95% CI: 0.6 to 11.2). 36
Physical disability & function
The only pain education trial35,36 reported no statistically significant post-op differences in ODI scores at any of the follow-ups.
Health-related costs
Health-related costs were reported in one prehab pain educational intervention trial (n = 67).35,36,39,42 There is very low certainty evidence (downgraded by risk of bias, inconsistency, imprecision, and publication bias) suggesting a statistically significant difference in the sum of direct and indirect healthcare system costs in favour of a pain education plus usual care versus usual care alone 1 year after surgery (MD: $2154.9 USD, 95% CI: $578.0 to $3731.8 USD), but not at the 3-year follow-up after surgery. 35
Discussion
In this systematic review of prehab interventions in adults undergoing elective spine surgery, we found inconsistent and very low certainty evidence of the beneficial effects of prehab interventions as compared to usual care alone across all outcomes and time points. Prehab that included predominantly exercise interventions plus usual care might be superior to usual care for disability at short-term, back pain at intermediate-term, and health-related costs at intermediate -term. However, no superior effect was found favouring prehab exercise interventions compared to usual care for back pain at short-term, leg pain at short- and intermediate-term follow-ups, and disability and health-related costs at long-term. Prehab CBT interventions plus usual care were shown to be more effective than usual care for back pain, disability, and HRQoL at short-term, for disability at intermediate-term, and for health-related costs at long-term follow-up. However, no difference between groups was found for leg pain, physical function, walking capacity, and TUG at short-term, and for back and leg pain, physical function, walking capacity, and TUG at intermediate-term follow-up. For prehab education interventions plus usual care, small effects in favour of the prehab interventions were found for back and leg pain at short-term, and leg pain and health-related costs at long-term. However, no difference between groups was found for disability at any of the follow-ups.
The results of our study varied depending on the type of prehab intervention used (i.e., exercise, cognitive behavioural therapy, or education), as well as the outcome measures and follow-up periods. Although there were some positive results in favour of prehab interventions, no clear trend was found when analysing the results to allow conclusions about whether prehab provided faster recovery for some specific outcomes or not. Additionally, the effects found were small, and the confidence intervals were wide, which led to uncertainty regarding the estimates. Therefore, more studies evaluating prehab interventions for adults undergoing elective spine surgery need to be conducted in order to increase our confidence in the estimates and provide more definitive conclusions.
Clinical practice guidelines recommend a multifaceted approach for managing low back pain, which can involve education, exercise, and psychological approaches like CBT.49–51 A previous prehab review mainly focused on CBT interventions concluded that incorporating exercise into CBT interventions may potentially improve post-operative outcomes. 21 Our review found insufficient evidence to support any of these therapies as standalone treatments. Therefore, to better inform health care professionals and patients on the most effective ways to manage back pain after surgery, it is crucial to conduct robust randomized controlled trials comparing the effectiveness of different prehab program components versus each other, as well as evaluate whether a combination of these approaches would yield any additional benefits. Further, not all participants may require all components of a prehab program and thus, mechanisms to identify who needs what intervention need to be identified and incorporated.
In addition to the studies including different types of interventions (i.e., CBT, exercise), the studies also varied in dosage, frequency, intensity, and timing.32,33,37,40 For instance, one study administered a 9-week prehab intervention twice a week, 33 while another delivered only four sessions in total. 41 Although the optimal dosage of prehab programs has not been established yet, it is crucial to identify the best parameters to decrease the variability of prehab interventions across studies to facilitate more robust comparisons and enable evidence-informed approaches for prehab interventions in adults undergoing elective spine surgery.
Our systematic review identified some heterogeneity among the included studies in terms of diagnosis and surgical procedures. Studies enrolled participants with chronic low back pain and radiating pain, 34 radiculopathy,35,36 LSS32,33,37,41–43 and even grade 4 spondylolisthesis. 32 These differences in diagnosis pose challenges that make it difficult to clearly identify and understand what conditions would need prehab interventions and what the most effective intervention designs would be for each condition. In addition, different conditions and severity require different surgical approaches, which can significantly impact post-surgical recovery. Future RCTs should enrol in more homogeneous lumbar diagnoses or include large enough samples to conduct subgroup analysis, which may clarify the specific needs and trajectories of each patient group.
In the current literature, there are some well-known modifiable and non-modifiable predictors of post-surgical pain and disability outcomes among low back pain patients. These factors include body weight, muscle strength, walking capacity, smoking status, baseline pain, and other psychosocial factors.11–15 However, it is still unknown what absolute reduction values these modifiable factors may have on back pain outcomes. Two of our included studies found a potential mediating effect of catastrophizing behaviours, anxiety, depression and kinesiophobia on the improvement of disability at 6 months follow-up.46,48 Therefore, more studies need to be conducted measuring to evaluate mediating and moderating effects to shed lights into mechanisms of action and potentially tailoring of the interventions.
Strengths and limitations
This review gives us a more updated and enhanced overview of the current evidence on prehab interventions than the other three previously conducted reviews,19–21 as it included more studies, focused on the effectiveness of prehab interventions, and presented meta-analyses of predetermined outcomes. Some of the strengths of our study include the use of valid and reliable tools to evaluate risk of bias (Cochrane Risk of Bias Tool 2.0), completeness of intervention reporting (TIDieR), and certainty of evidence (GRADE). Additionally, the pre-registered protocol increases the transparency of our study, while the inclusion of a meta-analysis improves the ability to deduce conclusions from pooled results.27–29
The limitations of our review stem from the inclusion of methodologically heterogeneous trials with small sample sizes, leading to inconclusive, and very low certainty of effect estimates. Due to the small number of included studies, subgroup analyses according to back pain diagnosis or surgery type could not be performed, which may provide a limitation in understanding how prehab may provide different outcomes in different contexts (e.g., fusion vs laminectomy alone). In addition, our review did not analyse the psychological outcomes known to mediate surgical recovery, although available evidence is limited. 52 One limitation that arose across the methods of included trials includes the predominant use of self-reported measures of physical function and disability (ODI, RMDQ), which are subject to various measurement biases such as recall and participant bias. 53 To circumvent this limitation researchers of trials may also include the assessment of performance-based measures such as 6-min walk distance. 54
The current systematic review identified a lack of high-quality evidence for the effectiveness of prehab interventions for lumbar spine surgery patients. Given the uncertainty in the results derived from low-quality RCTs, we cannot provide definitive recommendations for clinical practice. However, based on the available evidence, prehab exercise interventions may improve disability and back pain in the short- and intermediate-term follow-ups, respectively. Conversely, these programs may not have an effect on post-operative back and leg pain and health-related quality of life (HRQoL). Moreover, prehabilitation based on CBT may improve back pain and disability at short-term, and disability at intermediate-term follow-up. It is suggested that future trials should include larger sample sizes and well-defined populations and interventions. Furthermore, future research should compare outcomes after different types of surgeries, as outcomes may differ for different types of surgical procedures. By addressing these research gaps, we can better inform clinical practice and optimize outcomes for patients undergoing lumbar spine surgery.
Supplemental Material
Supplemental Material - Effects of prehabilitation on outcomes following elective lumbar spine surgery: a systematic review and meta-analysis
Supplemental Material for Effects of prehabilitation on outcomes following elective lumbar spine surgery: a systematic review and meta-analysis by Lisandra Almeida de Oliveira, Julian Anthony Vitale, Jasmeet Singh Sachdeva, Srikesh Rudrapatna, Sava Ivosevic, Najih Nuradin Ismail, Anthony Cubello, YV Raghava Neelapala, Nora Bakaa, Diego Roger-Silva and Luciana Macedo in British Journal of Pain.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The first author (LA) has received the Patricia Salomon Scholarship at McMaster University. The other authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.