
Abstract
Purpose
Chronic pain is a complex biopsychosocial experience, and rehabilitation helps people to manage pain, and restore valued life roles. Evidence suggests that more positive outcomes occur when clients perceive their rehabilitation to be meaningful. People with chronic pain describe rehabilitation as personally-meaningful when they develop a genuine connection with a credible therapist who they see as a guiding partner, and when rehabilitation holds personal value, is self-defined, and relevant to their sense of self-identity. This paper presents a qualitative study of therapists’ experience using an e-learning package on patient-defined, personally-meaningful rehabilitation.
Methods
A qualitative descriptive design was used to explore rehabilitation therapists’ experience of a prototype evidence-informed, online resource developed on the basis of eLearning and web-design principles. Semi-structured interviews and focus groups were conducted with a purposive sample of occupational therapists and physiotherapists, and inductive coding and thematic analysis of transcripts was completed.
Findings
Twenty-four therapists (12 occupational therapists, 12 physiotherapists) participated, representing a mix of gender and experience (early career; experienced; and specialist). Four themes and 12 sub-themes emerged from the analysis. The resource delivered a positive user experience, which added (translational) value to enhance learning, and participants were highly positive about the future potential of the resource to translate chronic pain rehabilitation research for early career, experienced, and specialist rehabilitation therapists.
Conclusion
Results suggest that the disparate learning needs of rehabilitation therapists from diverse professional backgrounds and experience, may be addressed through the one resource. Participant feedback provides evidence that the resource fits with current models of learning and behaviour change. This study demonstrates the importance of basing online resources on eLearning and web-design principles to translate complex biopsychosocial chronic pain rehabilitation research for rehabilitation therapists.
Keywords
Introduction
Chronic pain is a complex and personal experience, which involves interaction between biological, psychological, and social elements. 1 It can impair a person’s ability to engage in their usual roles and occupations, 2 reduce physical, social, emotional, occupational, and financial function,3,4 and has a negative socio-economic impact on a person’s significant others3,4 and broader society. 5 Rehabilitation is an important strategy to manage pain, regain function, improve quality of life, and restore meaningful or productive life roles. 6
Contemporary chronic pain rehabilitation often places emphasis on well-being7,8 and quality of life,9,10 over a sole focus on pain reduction. Clients are most likely to engage when rehabilitation is ‘goal oriented, meaningful and enjoyable’, 11 and this may lead to greater motivation to participate in rehabilitation, and potential for positive outcomes.12,13 A biopsychosocial approach is current best practice; 14 however, the rehabilitation professions are founded in a biomedical history and many rehabilitation therapists (RTs) may retain a primarily biomedical perspective. 15 Rehabilitation therapist entry-level training varies across professions, education programs, and countries and many RTs do not feel well-prepared to adopt contemporary chronic pain management practices.16,17 As chronic pain is a complex condition, RTs may need additional training at entry-level to achieve best practice. 18 Research disseminated through regular channels, such as peer-reviewed journal articles, is not always easy to access or understand 19 ; therefore, some RTs may also find it difficult to apply new evidence in practice settings.19,20 In Australia, there are calls for qualified RTs to undergo additional chronic pain training to strengthen their skills. 21
A 2019 concept analysis 22 found that chronic pain rehabilitation literature heavily privileged a clinician or researcher perspective, when using the term ‘meaningful’ in relation to rehabilitation. Out of this research, reflecting the patient perspective of meaningfulness in rehabilitation, the following definition emerged: ‘Patient-identified meaningfulness describes that which patients themselves select as being of value and relates to their personal sense of identity’. 22 A further qualitative descriptive study into the patients’ experience of meaningfulness in rehabilitation, 23 was conducted with Australian adults with chronic pain who had been exposed to physiotherapy or occupational therapy. Based on this study, rehabilitation is described as personally-meaningful by people with chronic pain, when it includes ‘a genuine connection, with a credible therapist, who can act as a guiding partner to address what the patient self-defines as personally valued and relevant to their self-identity’. 23 To optimize the outcomes of the rehabilitation experience, it follows that RTs need to understand this patient perspective.
Chronic pain currently affects around 20% of the Australian population 24 and, regardless of whether they have received specialist training, most RTs are likely to encounter people with chronic pain. In addition, RTs from different professions, such as occupational therapy (OT) and physiotherapy (PT), are exposed to different entry-level training in chronic pain, and some therapists may need to upskill.17,25,26 In order to deliver a service that their patients with chronic pain perceive to be meaningful, 23 more than ever access to convenient, low-cost education resources will be invaluable, to help RTs translate current research into their practice settings. 17 There is a considerable gap between the release of new research evidence and changes to practice,27,28 and this could limit uptake of research findings on personally-meaningful chronic pain rehabilitation. Various theories support knowledge translation (KT) processes29–31 to ensure that targeted activities achieve the intended outcomes in skills, attitudes, and beliefs of RTs. 32
Online learning appears to be an attractive option for easy-to-access, low-cost knowledge translation for a diverse RT audience. Online resources have been used successfully to improve health professional knowledge, 33 influence health professionals’ behaviour and improve patient outcomes, 34 and increase health professionals’ adherence to evidence-based guidelines. 35 Both clinician knowledge and patient outcomes improve following targeted KT activities.32,36–38 Many health professionals find online education cost-effective, 39 supportive of autonomous learning, 32 and convenient,40,41 with asynchronous delivery (self-directed learning) perceived to be the most convenient. 42 Once established, online resources are also often less time-intensive for trainers to deliver, 43 and can be as effective as conventional methods,33,43 whilst offering pragmatic benefits in audience reach, cost, and remote access. 43 Therefore, a logical solution is to develop an online KT resource on the topic of personally-meaningful chronic pain rehabilitation research. However, a background literature search found little evidence to demonstrate whether the concept of personally-meaningful rehabilitation could be effectively delivered online.
Biopsychosocially-based training may be inherently difficult to teach online,44,45 and a sound theoretical base is essential with a KT resource, to achieve the desired change in knowledge, skills, and attitudes. 46 Theoretically, learners should be better able to construct and retain knowledge when a resource is based on cognitive learning principles47,48 and intentional eLearning design.47,49,50 However, this assumption is untested with KT of personally-meaningful chronic pain rehabilitation research. For this reason, a prototype, evidence-informed, online resource was developed and tested, to answer the primary research question: “What is the experience of occupational therapists and physiotherapists using a prototype, evidence-informed online KT resource, to learn about patient-defined personally-meaningful chronic pain rehabilitation?”
Methods
Research design and theoretical stance
A qualitative descriptive design, 51 underpinned by a constructivist epistemology, 52 was used to explore RTs’ experience of the online KT resource. Research decisions were based on KT theory. 31 The COM-B Model of Behaviour, 31 and associated Behaviour Change Wheel, 31 were used to identify a suitable target translational activity and to guide the analysis. The COM-B Model of Behaviour Change 31 suggests that individuals will alter their behaviour when they experience a sufficient shift in physical or psychological capability; the opportunity presented by physical or social environments; and automatic or reflective motivation. A well-designed resource will target one of these elements or several concurrently. 31
Reflexive positioning
The first author (KL) is an occupational therapy clinician and academic with chronic pain management experience; AR is an academic-researcher specializing in motor learning and control; and CB is a rehabilitation scientist and occupational therapist with a program of research in pain meaning construction. Regular in-depth debriefing about study design, emergent data and iterative progress helped to maintain rigour, 53 and reflexive journaling improved confirmability of findings.53,54
Development of the knowledge translation resource
Examples of eLearning and web-design principles implemented in the online resource.
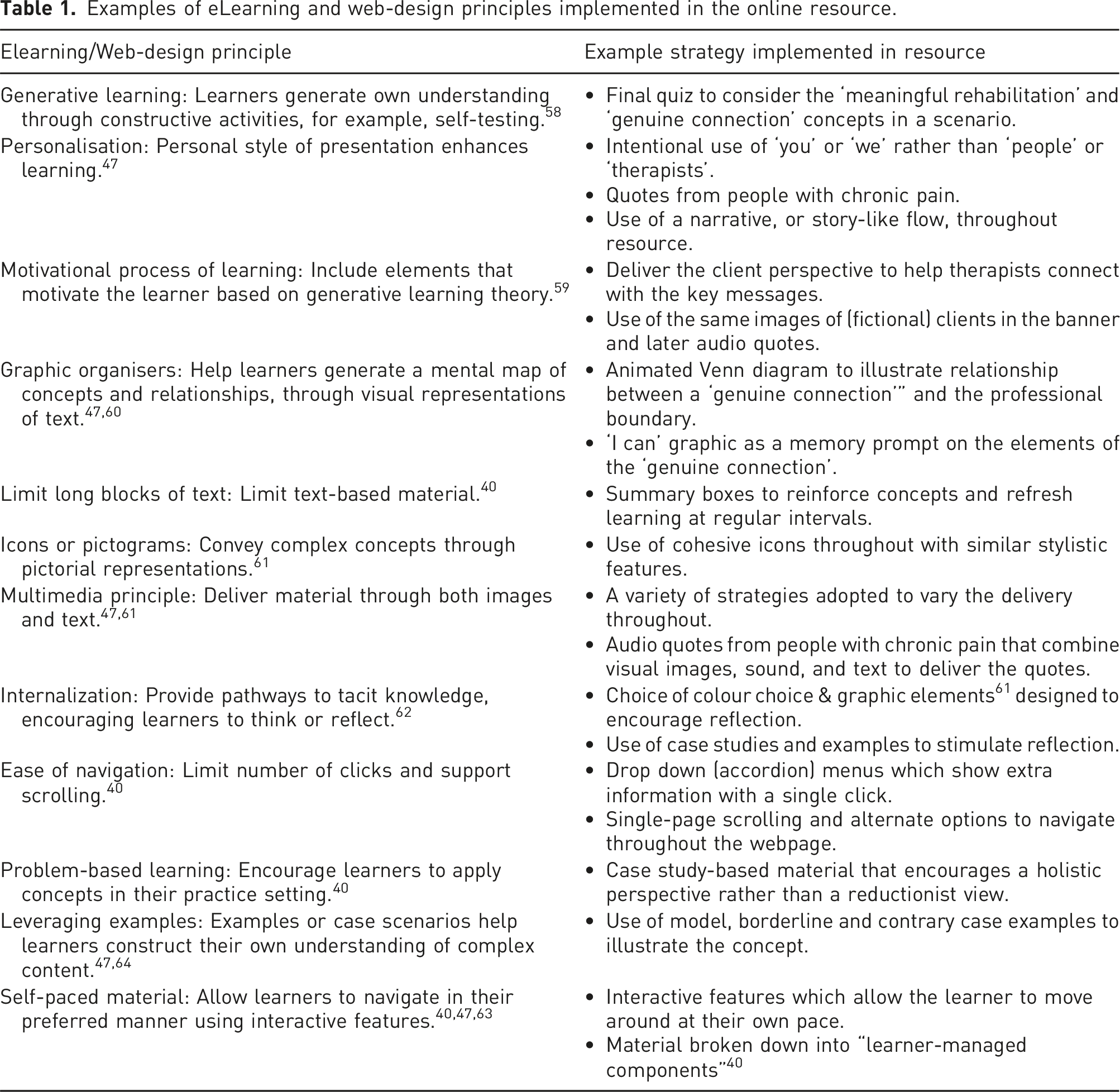
To improve access and navigation, the resource was pilot tested prior to release. The final resource included psycho-educational videos, interactive links and elements, summaries and translational messages, case-based reflective prompts, and a quiz. An example of one element within the resource is a graphic mnemonic, or memory prompt [Figure 1], on the concept of a ‘genuine connection’. The “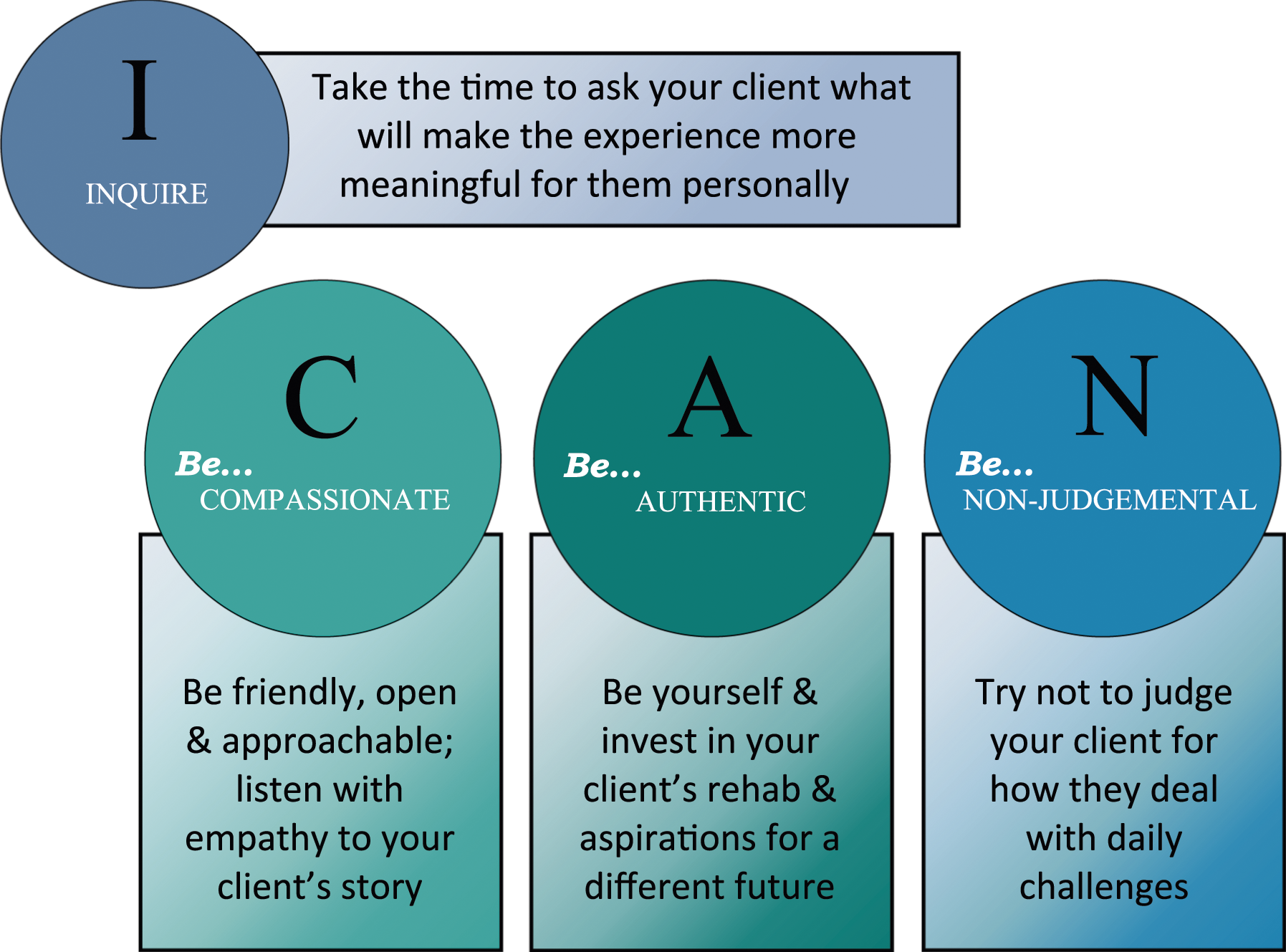
Sampling & recruitment
Following Edith Cowan University Human Research Ethics Committee approval [no.21008], purposive sampling was used to recruit RTs via social media, and direct contact with practices and professional contacts, across all states and territories in Australia. PTs and OTs were recruited to three categories to maximise heterogeneity
65
of profession, gender, and experience, or degree of specialisation in the field of chronic pain: a. ‘early career’ therapists: < 5 years post-graduation b. ‘experienced’ therapists: > 5 years post-graduation, not specializing in chronic pain c. ‘specialist’ therapists: currently specializing in chronic pain
Procedure
The emphasis of the study was explained via email. Participants could explore the resource in their own preferred way and time, although 30 min was recommended, and take notes on their experience, response to design elements, feelings, or thoughts. Verbal consent was obtained at the start of focus groups and interviews.
Data collection
Data collection spanned late 2021 to late 2022 and, to be as inclusive as possible, included both focus groups 66 and key informant interviews.67,68 Video or audio calls were made using Microsoft Teams. 69 Auto-transcripts were captured and transcribed verbatim by either the lead author, or a transcription service.
Interviews and focus groups contained similar semi-structured questions such as: What was your overall experience of the online resource? How important was it to be able to click around within the resource? Did any specific element(s) make you more inclined to adopt the key messages? Further probing questions were used to generate richer detail, for example: What aspects of the resource do you think most encouraged you to reflect in the way you describe?
Data analysis
Transcripts were de-identified and pseudonyms assigned. Transcripts were read in detail multiple times, to ensure a rich understanding of the data. 70 Coding and inductive thematic analysis 70 were led by the primary researcher, and methodological decisions were tracked in a codebook. 71 In a coding audit of 10% of data from each participant group, the primary researcher and one other team member (AR) coded data independently, examined differences, and reached agreement on codes. Each data set (early career, experienced and specialist therapist) was coded separately. Codes were then compared across data sets to ensure consistent terminology.
Results
Participant demographics.
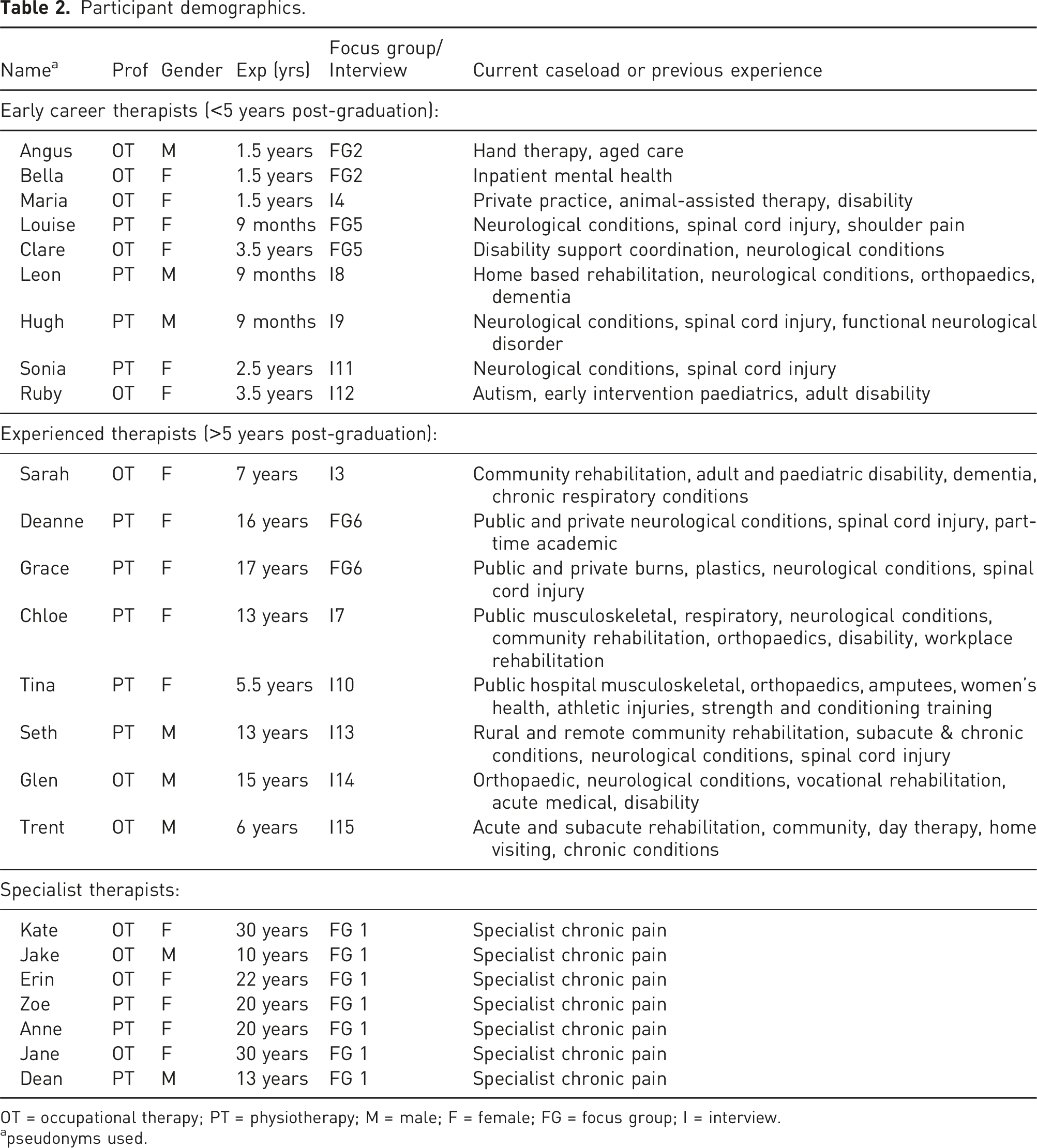
OT = occupational therapy; PT = physiotherapy; M = male; F = female; FG = focus group; I = interview.
apseudonyms used.
Twelve individual interviews and three focus groups were conducted online through video or audio calls. Participants were from various states across Australia with three participants located in remote parts of the country, or regional centres.
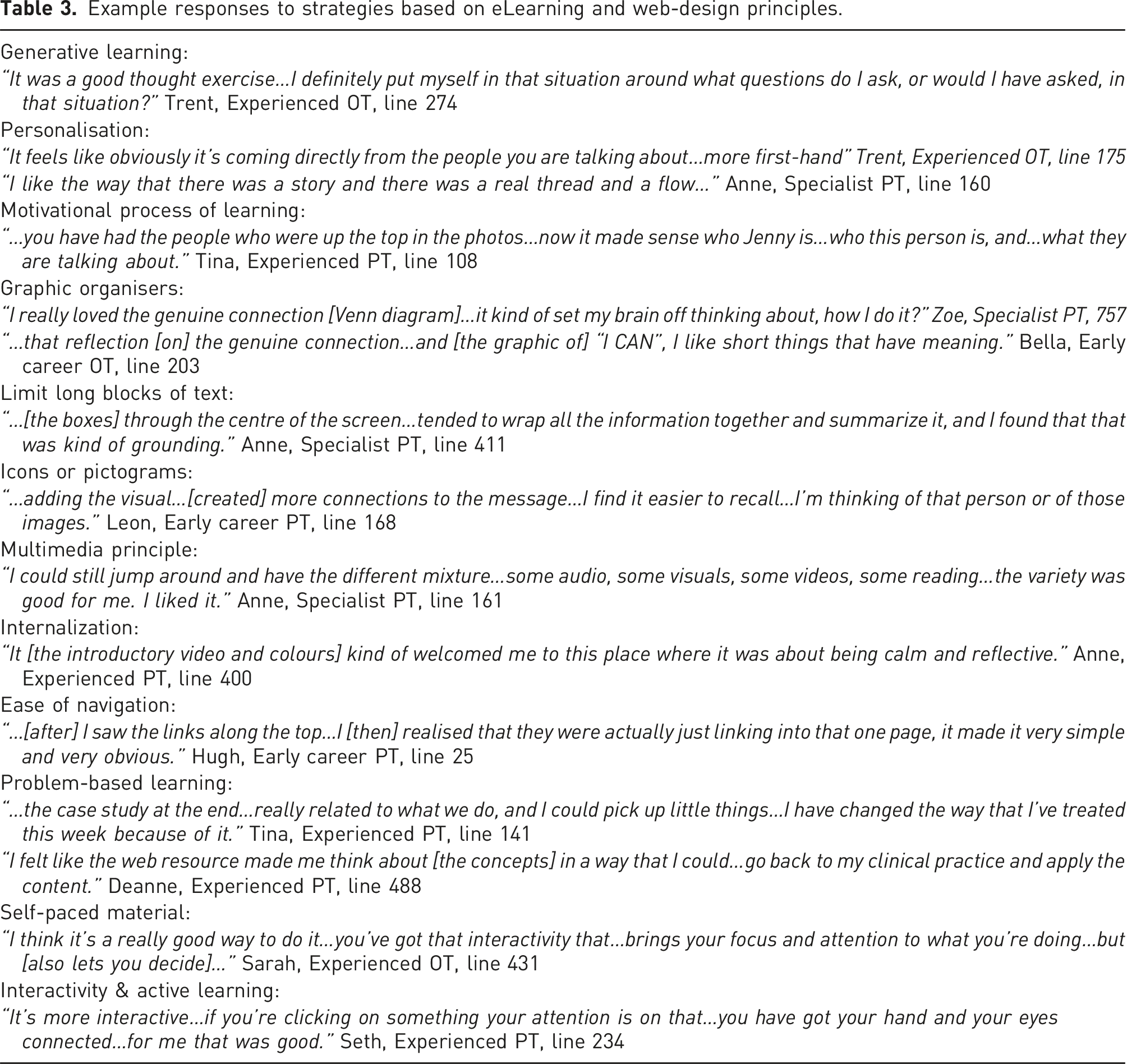
Example responses to strategies based on eLearning and web-design principles.
Four themes and twelve sub-themes emerged during analysis [Figure 2], with overlaps in theme boundaries. Themes indicate that the resource provided a positive user experience; which added (translational) value; and enhanced learning about research into personally-meaningful chronic pain rehabilitation. The fourth theme was the future potential offered by the resource for therapists in early career, experienced, and specialist stages of professional development. Themes and sub-themes. Broken lines indicate further relationships, and overlaps, in theme boundaries.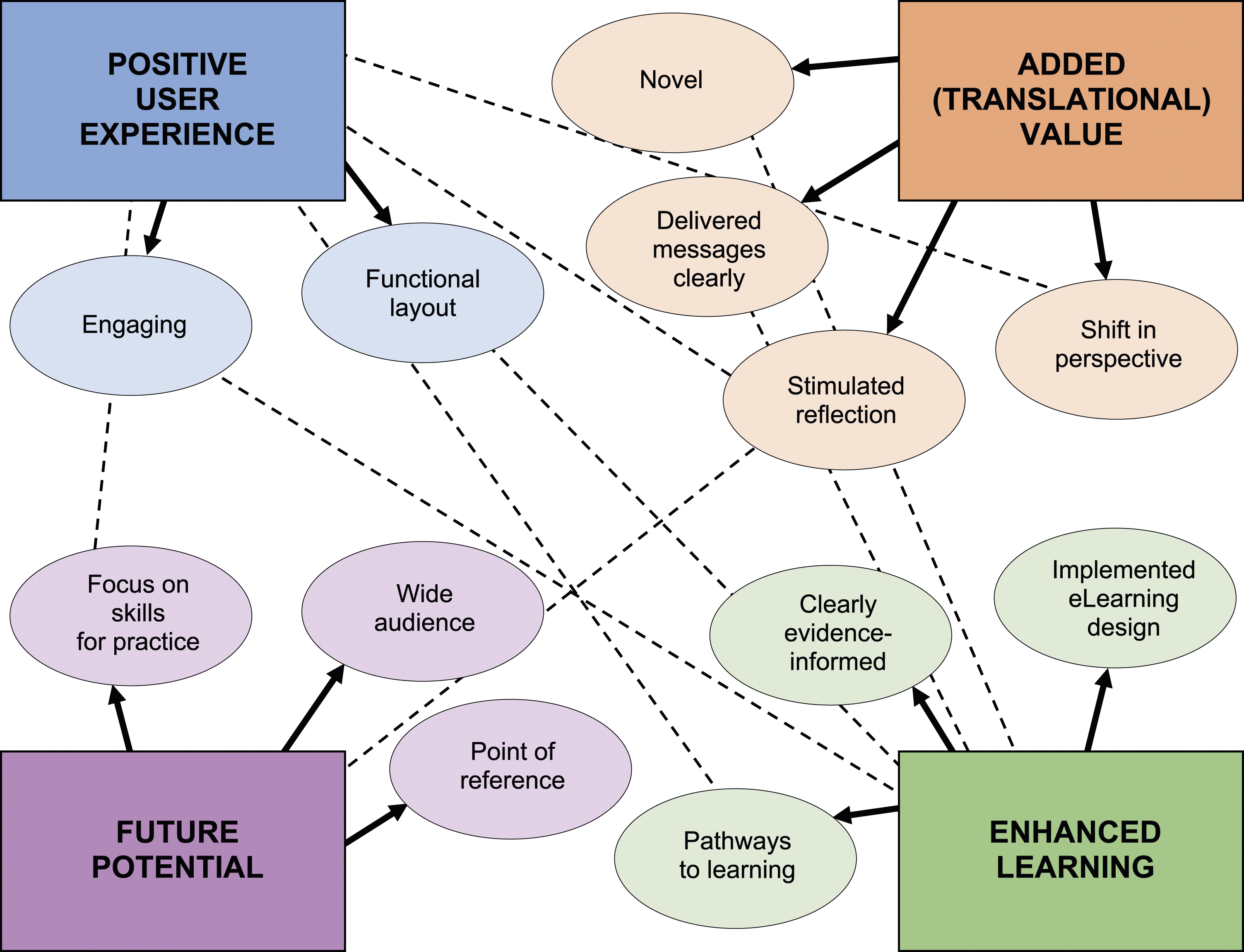
Theme 1: Positive user experience
Participants’ overall positive response to using the online resource was reflected in two sub-themes. Broadly, participants described an engaging experience where the method of delivery enhanced the uptake of key messages:
“…a lot of the pain education stuff comes in big fat whomping (sic) books or a huge text…having something that’s a bit more interactive might be the way to go for some people.”
Sonia, early career therapist, line 351
Participants explained that the functional layout felt uncluttered and supported the learner to focus. The interactive elements and minimalist layout also allowed them to pace learning, and to avoid becoming overwhelmed. The resource offered several ways to access information (tabs across the top or a single scrolling page) which encouraged autonomy for learners, and the single-page scrolling format allowed some to feel continuously connected to the main home screen:
“…I think it made it more engaging…it gives you the option…if you feel like you know something already, or you can understand something already quite well, you can move onto the next part or keep moving…”
Trent, experienced therapist, line 150
Theme 2: Added (translational) value
When compared to other dissemination methods or educational resources, participants across all three groups felt that the resource added value for them as a research translation device. There were four sub-themes. Participants described the resource to be novel or different from other continuing professional education (CPE) resources or dissemination methods. This difference related to both the overall approach, and the layout used:
“I guess I don’t know if I have yet seen a lot of resources around, when I am looking up information and things, [that] are laid out in a similar way…I definitely felt like it was a good way to take [it] in…”
Trent, experienced therapist, line 92
As compared to a traditional journal article, participants found the resource required less time, was easier to access, and delivered the message through multiple methods. Participants explained they would, therefore, be more likely to return to the resource in future:
“…often research [papers] can be quite daunting…in terms of trying to digest it and interpret it and read it. So, it was in a really user-friendly…snapshot of what the important information was…It definitely felt like it was something I could take in and absorb…rather than [to] try and read a research paper”
Trent, experienced therapist, line 63
Part of the translational value of the resource was that it delivered key messages clearly. To help achieve this, the resource first reinforced participants’ current understanding of chronic pain, before extending into new knowledge:
“…whilst you were delivering…[a] message [consistent with my understanding of modern pain], I thought it was looking at pain with a different lens…I understand and embody client-centred practice, but the focus on ‘meaningful’ was something that I haven’t really encountered in various things that I’ve done, in terms of education on pain.”
Deanne, experienced therapist, line 454
The language and case scenarios helped to strengthen the key messages and participants felt this made the overall information more relevant to their own patients. In particular, early career and experienced therapists found the short summaries and take-away statements, which were repeated throughout, helped to deliver the messages and focus their attention:
“…the quote boxes were really useful I think because they were central, they were slightly bigger font, so it was obviously what you wanted to highlight as of quite big importance throughout the whole message...so that was good”
Trent, experienced therapist, line 187
In all three groups, the resource stimulated reflection for participants about their practice behaviours and attitudes, specific patients, or rehabilitation concepts. Some found the reflection was triggered by the overall experience, whereas others recognised that specific aspects of the resource encouraged them to challenge their past beliefs about chronic pain and clarify difficult concepts. Early career and experienced therapists found the case examples a helpful stimulus to reflect on aspects of their own practice, while the specialist therapists also perceived value in these case studies for junior staff:
“…these stories…help…bring that emotional side to it. [That]…forced me to reflect on my experience…and I feel like I gained a bit more understanding about…my early patients…when I was feeling probably a bit lost and a bit confused…you know, the joys of being a new grad?”
Angus, early career therapist, line 771
Through this reflection, participants saw a shift in perspective, triggered by elements such as videos, case scenarios, and the patient ‘voice’. Many participants said they became more aware of the genuine connection they currently shared, or felt they could strengthen, with some patients. There was also a shift in perspective to value a more holistic, biopsychosocial approach in practice, or at least allow a slower pace in order to strengthen the human connection with their patients during rehabilitation. Some participants recognised an immediate difference in their own practice behaviours as a result of the experience: “…this [client in the clinic] I noticed she started crying and I [was] almost like, ‘I’m really sorry’…and [then] still continue to type. [But because of reading that case study] I was like, ‘Stop typing. Your history taking right now is not that important’.” Tina, experienced therapist, line 192
Theme 3: Enhanced learning
Responses from participants suggest that the resource enhanced learning. The first of three sub-themes showed that learning was enhanced by those elements that implemented eLearning design principles. These elements included the timing, or length of sections and videos, the language used, the sense of narrative or flow, and the considered use of visual elements. The narrative feel helped the experienced and specialist participants to remain oriented, and kept them engaged as the ‘story’ of the research unfolded:
“…then when you saw the faces [from the website banner] down further through the screen and they had little audio grab for each of them talking about an aspect of what they look for in a therapist. That really grabbed me. I liked that.”
Anne, specialist therapist, line 716
The learning was enhanced by hearing the ‘patient voice’ through audio quotes and case examples, and this also made the experience more engaging. Participants felt that the case study-based, professional development quiz motivated them to learn, or to solidify prior knowledge. Some were initially surprised at the lack of right/wrong answers in the quiz; however, others felt this conveyed a feeling of a safe and non-judgemental learning space:
“…when I…saw the answers, I am like, ‘Oh, wow I have to think about this a little bit’. [But] it’s not ridiculously difficult and the fact that it gave me answers at the end…it was a good reflection…[and] I didn’t feel…judged…”
Tina, experienced therapist, line 257
Participants widely discussed the translational value of the ‘I CAN’ mnemonic and graphic [Figure 1], sharing that it helped them recall the core ‘genuine connection’ message while they read case studies, or while later talking with their own patients. Summary boxes and take-home messages, that were placed at regular intervals throughout the resource, also helped participants to relate the research findings to their practice: “…I really liked…there were…some phrases through the centre of the screen…and they tended to wrap all the information together and summarize it and I found that that was kind of grounding.” Kate, specialist therapist, line 291
Most participants deemed the timing, or length of design elements like text or videos was appropriate to their needs, and the succinct delivery helped to minimize their time commitment and learning burden. The specialist therapist focus group held robust discussion about whether the videos were short enough, or too short. They did not alight on any agreement, and some shared the strategies they personally adopted in relation to this time commitment, such as seeking out a transcript, looking for a listed time required to watch a video, or playing the video at 1.75 speed. Overall, participants’ response to videos was positive, and they explained that videos broke up the learning material, helping to introduce complex concepts in a less burdensome way.
“I really loved the [video on] genuine connection. I can remember…having a bit of a look and [thinking]…I didn't want to see anything else. That was enough. I liked it and it kind of set my brain off thinking about…how I do it?”
Zoe, specialist therapist, line 757
The evidence-informed visual elements, for example, the colour palette, use of icons versus photographic images, and the custom-created graphics, elicited a range of responses. Participants generally perceived the colour scheme to be calm and reflective, although one participant said it made the online resource feel outdated. Participants perceived that their learning was supported by visual elements such as images of real people and icons to navigate topics. Many appreciated the use of animations and visual analogies to illustrate complex concepts, such as an animated Venn diagram to explain the relationship between the ‘genuine connection’ and professional boundaries, or a traffic light to convey the concept of pain as a biopsychosocial phenomenon. Whilst the response overall was highly positive, a small number also noted certain elements that caused them to briefly disconnect, for example, one participant noted that the patterned background in a video was distracting and would be better with a single block colour.
Participants generally believed that the resource was clearly evidence-informed, and they held a positive view of the popup citations as a simple but non-disruptive method to convey this. Some participants assumed that the resource was current and evidence-informed, either because of the overall appearance, or their assumption about authorship. Some commented that knowing the resource was evidence-informed helped to validate their own approach to chronic pain: “I found it validating that the time and the energy and the effort that I put into my consultations, and being one on one with them, being in an individual room and taking that time to listen, you’ve just told me that the research says that that is the right thing to do.” Erin, specialist therapist, line 1014
In all three groups, participants said the online resource made good use of pathways to learning, supported their personal learning style, and gave them control over the learning experience. Many participants knew their own learning styles, for example, visual, auditory, or kinesthetic, and felt that the online resource catered well to their needs: “I’m a very visual learner as well, but I liked the idea of being able to read something and then if I didn’t quite get the message from reading it, I had the opportunity to look at something that was more visual, like a video.” Hugh, early career therapist, line 77
Overall, participants appreciated the elements that allowed them to self-pace learning, focused their attention to keep them engaged, or helped them to feel less overwhelmed by the complexity of the topic.
Theme 4: Offers future potential
The final theme showed that participants saw future potential in the resource, and this provided valuable insight into what the researchers could include in future iterations. All three groups of participants saw potential for the resource to act as a point of reference, and a trigger to change, or reinforce, their approach in practice. Despite their considerable chronic pain experience, even specialist participants valued the resource as a way to validate their own approach, and to support junior staff. Some participants explained that the experience highlighted their currently unmet need for a single, regularly updated, and reputable source for chronic pain rehabilitation research translation. “When you’re working with people with such extreme [circumstances]…for a long period of time…it was just a good reminder [that] the science is there [about the genuine connection] to say, ‘Yes, what I'm doing is correct’.” Kate, specialist therapist, line 1134
Although opinions varied within, and across, the three groups, participants generally saw the resource as relevant for a wide audience of health professionals from multiple disciplines beyond physiotherapy and occupational therapy, and at all levels of experience, or working in broad fields of rehabilitation beyond just chronic pain. All participants said they had already or would be keen to share the resource with colleagues, and many recognised a potential benefit of the resource for rural and remote RTs, or those working in non-pain specific fields who might not prioritise funds, or time, to attend chronic pain CPE. One experienced therapist felt that a particular benefit was the interdisciplinary nature of the resource, and that it delivered a consistent message to all types of RTs. “…the simplicity of just giving these younger therapists…exactly what we, as more experienced therapists…know [to do as] a good therapist…we [hopefully] know how to engage clients and I don’t think that’s always obvious to work backwards…I thought [the web resource] captured…really simply for the junior therapist to go ‘It’s not just experience, these things can be learnt, skills…can be taken from [this]’.” Erin, specialist therapist, line 202
A small number of participants felt the resource would be useful for patients, however, most decided that it would not be appropriate with the current format and language. Some believed that there was an unmet need, however, for a shared resource about personally-meaningful rehabilitation, to bring patients and therapists together in a place of greater understanding.
Participants’ felt there was a pragmatic focus on skills for practice that helped move concepts from research directly into practice. This perspective was not unique to early career and experienced participants, and specialists also felt that their practice skills would be validated, and strengthened, through the experience:
“…a lot of my experience is [that] juniors have more intuitive skill in this area than some of the seniors who get quite set in their ways…I think limiting this to just inexperienced physios is actually limiting this opportunity for a lot of people to learn.”
Anne, specialist therapist, line 602
Discussion
As the incidence of chronic pain rises in Australia, 72 there are increasing calls for health professionals with varied backgrounds and experience to learn how to provide more effective interventions for the condition.21,73 Evidence, including recent work regarding personally-meaningful rehabilitation, 23 suggests that RTs need to engage with a more person-centred74–76 and biopsychosocial approach. 14 The change to a more biopsychosocial approach requires a shift in beliefs about chronic pain and holistic care.14,75,77 Despite this, many health professions still lean towards a traditional biomedical lens 15 and it can be difficult to change long-standing beliefs and behaviour. 78
Online education is thought to be underutilized for knowledge translation, 29 despite offering flexible,40,41 low-cost, easy access training,39,79,80 while demonstrating similar engagement, uptake of knowledge, and learner satisfaction to traditional methods. 39 This study demonstrated that a prototype, evidence-informed resource was able to deliver a positive user experience, added (translational) value to enhance learning, and offer future potential to shift RT understanding of what people with chronic pain find personally-meaningful in their rehabilitation. These findings provide promising early evidence that a single resource can deliver relevant knowledge to a diverse RT audience, when underpinned by eLearning and web-design principles, and behaviour change theory.
In order to compete with the dense general flow of online and social media traffic, contemporary online education needs to both inform and engage. 81 The intentional design of this KT resource was essential to achieve both of these goals. According to participants, the resource met both engagement and information needs, and they described a positive user experience, enjoying the functional layout and engaging elements that were based in eLearning and web-design. Engaging online delivery is known to increase uptake of research into practice, 31 although there is an important distinction between the impact of simple behavioural engagement, such as clicking and interacting with the resource, and cognitive engagement, which leads to learning. 47 Participants also felt the resource met their needs, regardless of personal learning style or capabilities, as information was delivered through multiple sensory channels, 82 and concepts were repeated in multiple ways. 83 This approach also offered the benefit of variety, which is known to be well-received by health professionals, 45 with case illustrations, audio quotes, regular summaries and take-home messages, graphics, and mnemonic memory prompts. Interactivity provided dual benefits of being engaging, whilst offering the option to pace learning according to prior knowledge and experience. This also enabled the resource to better meet the learning needs of a diverse RT audience.25,26
This study demonstrated that a KT resource can both inform and engage; however, there is an ethical responsibility to ensure KT resources deliver appropriate messages. In this study, the sense of narrative, or flow, throughout the resource helped participants invest in the messages, oriented them within the ‘story’ of the research, and built the argument for personally-meaningful chronic pain rehabilitation. Dissemination of research through a more narrative style has been explored in other literature, such as the positive influence of a narrative style of delivery on beliefs, attitudes, behaviours and intentions, 84 risks and benefits of blogs for healthcare professionals, 85 or as an effective method to relay challenging cognitive concepts. 86 The exciting opportunities presented by developments in generative artificial intelligence, 87 may entice researchers to ‘sell’ their findings through engaging, and easily-developed, online education resources. The findings of this study demonstrate that, when building KT resources, it is important to rigorously apply eLearning, web design, and behaviour change evidence, and then investigate the response of the intended recipients.
As the transdisciplinary approach to chronic pain increases, training resources must meet the needs of multiple professions. Participants from both OT and PT saw future potential in this resource as a point of reference to translate research for RTs with all levels of experience, along with a wider, multi-disciplinary audience such as social workers, exercise physiologists, and speech pathologists. PT training is traditionally more biomedically based15,88 and many PTs report discomfort with psychosocial care, 77 whereas in contrast, OTs traditionally receive fairly extensive entry-level training in a biopsychosocial approach. 89 Encouragingly, as a result of their experience with the resource, both OT and PT participants said they would now incorporate more of the personally-meaningful rehabilitation concepts in their own practice. Both PT and OT participants expressed a desire to share the resource with others or had already shared it. This supports the finding that the resource created a positive learning experience regardless of previous training.
Limitations
A pragmatic decision was made to limit the sample, so this study does not reflect the experience of RTs in other countries, or other RT healthcare professionals such as exercise physiologists, psychologists, and chiropractors. The chronic pain landscape is changing rapidly, and as the biopsychosocial approach becomes more instinctive and familiar, this resource may not meet training needs of all RTs.
This sample was recruited purposively with the intention of a more diverse representation. Participants came equally from OT and PT, with various levels of experience, and from different states across Australia, working in both metropolitan and rural and remote areas. One limitation of the study is that participants were not asked whether their background, or the institutional context of their work, had any influence on their experience with the resource. For example, this study has not captured whether hospital-based RTs have a different experience or learning needs to private practitioners. Future research should examine barriers at policy and institutional level.
Participants shared their ideas for future iterations of the resource, and the potential to partner the resource with other KT strategies, such as workshops. This study did not explore the relationships between behaviour change elements and the resource, however, participants’ responses were highly positive, and findings suggest this may be worthy of further investigation.
Conclusion
This study supports the premise that a well-designed, evidence-informed, online KT resource is able to deliver key messages about personally-meaningful chronic pain rehabilitation, as a person-centred, biopsychosocial approach to chronic pain rehabilitation. Investment in an evidence-informed KT process using eLearning, web-design, and behaviour change theory paid dividends in the positive response from participants.
Footnotes
Acknowledgements
We would like to acknowledge the generous participants who gave their time and their perspectives; and Professor Mandy Stanley for guidance on aspects of the project, particularly expert knowledge about descriptive thematic analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Edith Cowan University (PhD support for web development).