
Abstract
Background
Breakthrough pain is common in life-limiting conditions and at end-of-life. Despite over 30 years of study, there is little consensus regarding the definition and characteristics of breakthrough pain.
Objective
This study aims to update and expand a 2010 systematic review by Haugen and colleagues to identify (1) all definitions of breakthrough pain and (2) all descriptions and classifications of breakthrough pain reported by patients, caregivers, clinicians, and experts.
Design
This rapid systematic review followed the Cochrane Rapid Review Methods Group guidelines. A protocol is published on PROSPERO (CRD42019155583).
Data sources
CINAHL, MEDLINE, PsycINFO, and the Web of Science were searched for breakthrough pain terms from the inception dates of each database to 26th August 2022.
Results
We identified 65 studies that included data on breakthrough pain definitions, descriptions, or classifications from patients (n = 30), clinicians (n = 6), and experts (n = 29), but none with data from caregivers. Most experts proposed that breakthrough pain was a sudden, severe, brief pain occurring in patients with adequately controlled mild-moderate background pain. However, definitions varied and there was no consensus. Pain characteristics were broadly similar across studies though temporal factors varied widely. Experts classified breakthrough pain into nociceptive, neuropathic, visceral, somatic, or mixed types. Patients with breakthrough pain commonly experienced depression, anxiety, and interference with daily life.
Conclusions
Despite ongoing efforts, there is still no consensus on the definition of breakthrough pain. A compromise is needed on breakthrough pain nomenclature to collect reliable incidence and prevalence data and to inform further refinement of the construct.
Introduction
Adults and children with cancer, life-limiting conditions, and those at end-of-life1,2 commonly experience continuous mild-moderate pain (background pain) and acute episodes of more severe pain, known as breakthrough pain. The definition of breakthrough pain varies in the literature, affecting reported prevalence. A systematic review reported pooled prevalence rates of 59.2% in adults with cancer. 3 Paediatric breakthrough pain prevalence estimates are limited to a small, retrospective narrative review of medical records 4 and a study reporting that 15 of 27 hospitalised children with cancer (57%) had experienced breakthrough pain in the previous 24-h. 5 Yet, anecdotal evidence suggests rates are much higher.4,6 Breakthrough pain management is often inadequate,5,7 causing significant detrimental effects on wellbeing, quality of life, and functioning.8–10 Continuous careful evaluation of a patient’s pain is essential for effective breakthrough pain management. 11
In 2010, Haugen and colleagues conducted a systematic review of the assessment and classification of cancer breakthrough pain. 12 Although the authors found broad agreement in cancer breakthrough pain definitions, they found no single, broadly accepted breakthrough pain definition, assessment tool, or classification system. Moreover, our recent systematic review found a lack of valid, reliable breakthrough pain assessment tools.13,14 Only the Breakthrough Pain Assessment Tool 10 could be recommended for use, but this is a self-report tool only validated to characterise breakthrough pain in adults with cancer.
Our research aims to update and expand Haugen and colleagues’ (2010) systematic review to identify breakthrough pain definitions, descriptions, and classifications of all types experienced by patients of all ages and with any medical condition. The current review was undertaken to identify (1) all definitions of breakthrough pain and (2) all descriptions, experiences, and classifications of breakthrough pain reported by patients, caregivers, clinicians, and experts. A great majority of clinicians and researchers, including the authors of this review, maintain the view that the current plethora of breakthrough pain definitions makes communication between professionals and families difficult, has significant adverse consequences for the clinical management of patients, and undermines reliable incidence and prevalence data collection. By providing a comprehensive and exhaustive summary of definitions of breakthrough pain, we hope this will serve as a small first step towards achieving an eventual consensus in a definition of breakthrough pain.
Methods
This rapid systematic review is part of a large multi-centre study (the BEACON study) aiming to develop a validated paediatric breakthrough pain assessment tool. PRISMA guidelines 15 were followed (Supplementary File 1) and the Cochrane Rapid Review Methods Group guidelines. 16 A detailed description of the methods, including the full search strategy, is included in our protocol 17 (PROSPERO: CRD42019155583). CINAHL, MEDLINE, PsycINFO, and Web of Science were searched from database inception to 26th August 2022. The reference lists of eligible articles were also screened. A search strategy was developed incorporating search terms in two blocks: 1. ‘breakthrough pain’ and 2. ‘definitions, descriptions, characteristics, experiences, and classifications’.
Quality assessment tool adapted from the LEGEND evidence appraisal of a single study (all domains; expert opinion) tool and the appraisal tool for cross-sectional studies (AXIS).
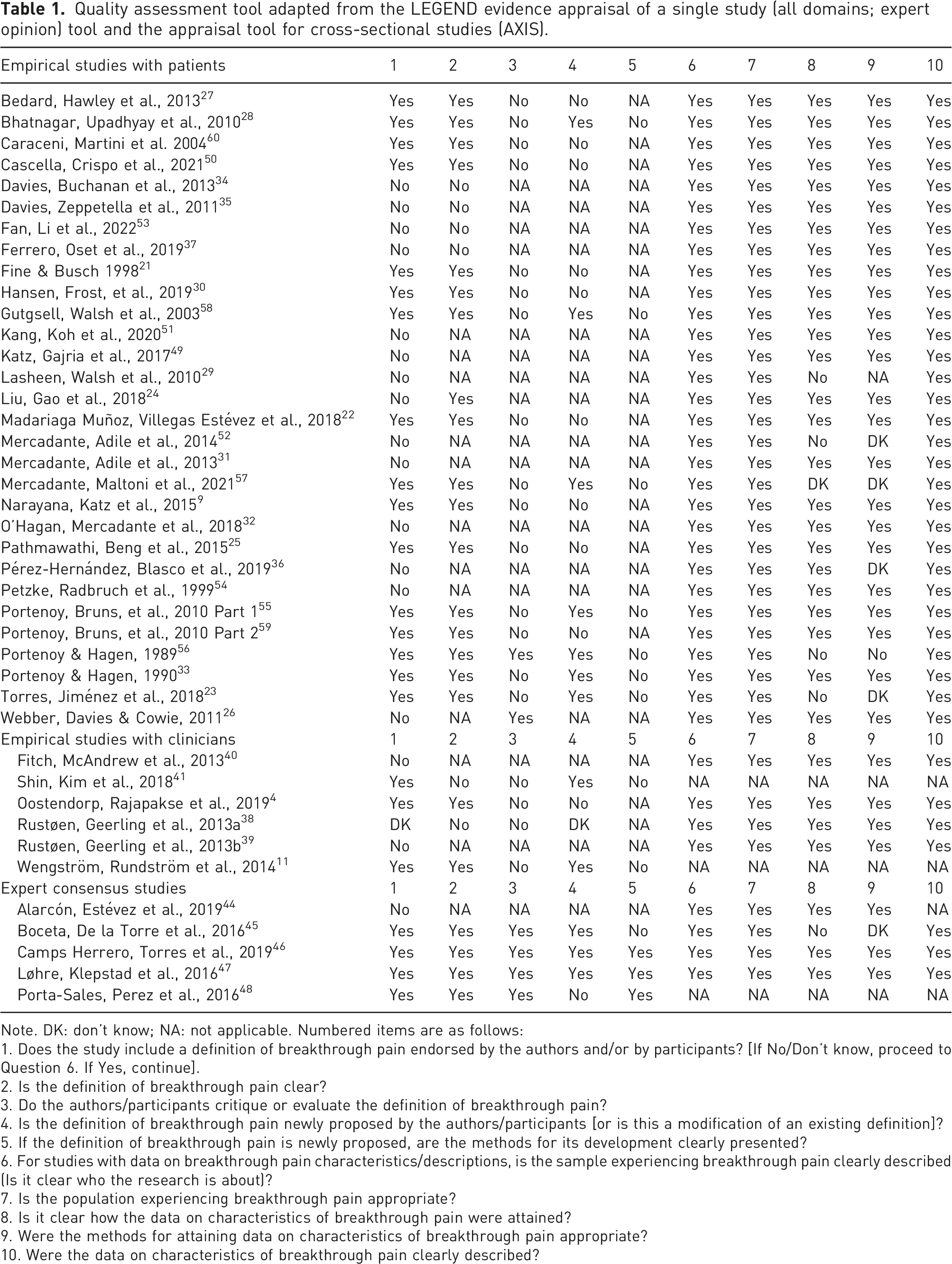
Note. DK: don’t know; NA: not applicable. Numbered items are as follows:
1. Does the study include a definition of breakthrough pain endorsed by the authors and/or by participants? [If No/Don’t know, proceed to Question 6. If Yes, continue].
2. Is the definition of breakthrough pain clear?
3. Do the authors/participants critique or evaluate the definition of breakthrough pain?
4. Is the definition of breakthrough pain newly proposed by the authors/participants [or is this a modification of an existing definition]?
5. If the definition of breakthrough pain is newly proposed, are the methods for its development clearly presented?
6. For studies with data on breakthrough pain characteristics/descriptions, is the sample experiencing breakthrough pain clearly described (Is it clear who the research is about)?
7. Is the population experiencing breakthrough pain appropriate?
8. Is it clear how the data on characteristics of breakthrough pain were attained?
9. Were the methods for attaining data on characteristics of breakthrough pain appropriate?
10. Were the data on characteristics of breakthrough pain clearly described?
Results
Sixty-five eligible studies were included (Table 1). No studies were found with data from caregivers and only one study involved children with breakthrough pain.
21
Figure 1 displays the flow diagram of search results. Inter-coder agreement between KG and DES for exclusion/inclusion decisions by article title and abstract was substantial (0.73 Cohen’s kappa coefficient). After discussion, KG and DES reached 100% agreement on all inclusion/exclusion decisions. Studies varied in quality, and for most both strengths and limitations were noted. For example, where applicable all studies clearly described an appropriate sample of patients experiencing breakthrough pain, and clearly described data on characteristics of breakthrough pain. However, a common limitation found with most studies was that the authors endorsed a breakthrough pain definition without critique or evaluation. Furthermore, of the 13 studies providing a newly proposed definition of breakthrough pain, only three presented methods for its development clearly. Complete quality appraisals for each individual study are displayed in Table 1. Data extraction tables are available in Supplementary File 2. A schematic representation of the key breakthrough pain terms found is provided in Figure 2. Flow of records for inclusion in a rapid systematic review of the definition, description, and classification of breakthrough pain by patients, caregivers, clinicians, and experts.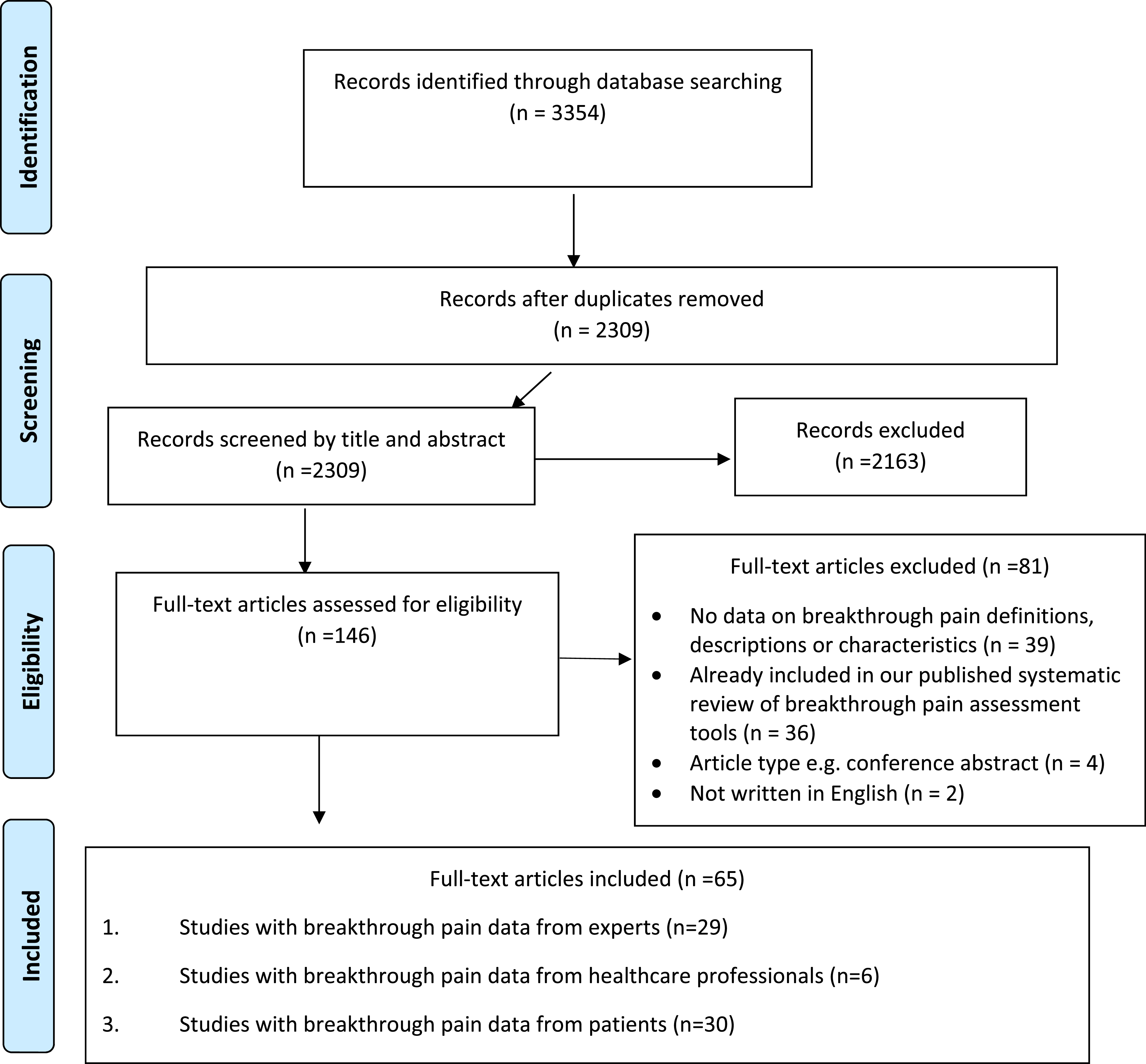
Empirical studies with patients
Thirty articles involved empirical studies with patients. Participants were adults with cancer (n = 26), adults or children receiving hospice care for cancer or other conditions (n = 1),
21
adults with chronic pain due to cancer or other conditions (n = 2),9,22 and adults with chronic lower back pain (n = 1).
23
These were quantitative survey studies (n = 26) and qualitative interview studies (n = 3).24–26 Only one study asked patients their views on the meaning of breakthrough pain.
26
The term was not widely understood and some participants found it difficult to distinguish between background pain and breakthrough pain. Inclusion criteria for patients with breakthrough pain in each study are shown in Supplementary File 4. This was not clearly stated in eight studies.23,25,27–32 One
22
cited Portenoy & Hagen’s 1990 definition of breakthrough pain
33
as the inclusion criteria while five24,26,34–36 used the diagnostic algorithm developed by a task group of the Science Committee of the Association for Palliative Medicine of Great Britain and Ireland.
7
The criteria for breakthrough pain in one study
37
were pain rated as ≥5/10 on a visual analogue scale. The criteria for the remaining studies required patients to have both background pain (usually ‘controlled’) and transient peaks of more severe pain. Schematic representation of the key terms found in a rapid systematic review of experts’, clinicians’, and patients’ definitions of breakthrough pain. Coloured boxes with bold outlines indicate the most commonly used terms. White boxes indicate descriptions used only by a minority in the literature. Boxes with dashed outlines signify suggestions from experts for terms to replace ‘breakthrough pain’.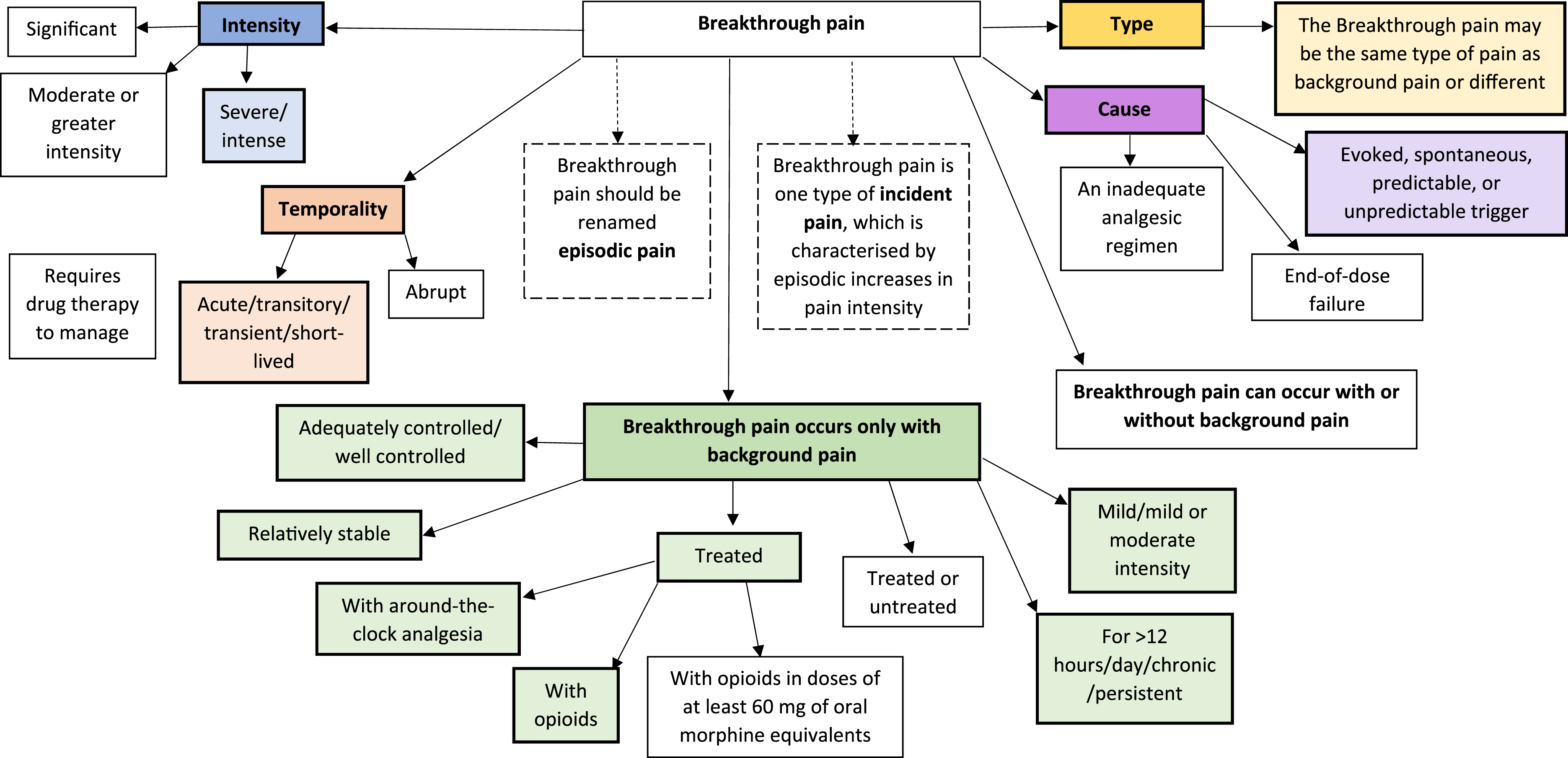
Empirical studies with clinicians
Six articles detailed four empirical studies with clinicians (three from the same study).11,38,39 Five were quantitative surveys with nurses11,38–40 or physicians 41 about breakthrough pain in cancer. One was a study exploring the feasibility of generating reliable information on breakthrough pain in children with life-limiting conditions from narrative clinical records. 4
In one study, 210 oncology nurses were given statements and asked to select which most accurately defined breakthrough pain. Most selected ‘episodic pain that breaks through the stable background pain’ and ‘pain that requires additional or adjustments to current pain medication’. 40 A study with 1241 oncology nurses 11 used similar methods and reported that 72.5% selected the definition ‘episodic pain that breaks through the stable background pain’, 42.2% chose ‘spontaneous pain/unpredictable incident’, 22.5% chose ‘predictable incident pain’, 4.2% reported ‘not sure’, and 3.5% reported ‘none of the above’ (some respondents selected more than one response). A study with 92 palliative care doctors 41 also asked participants to select between one of two breakthrough pain definitions. Most (66.3%) defined breakthrough pain as transient and exacerbating pain after control of background pain while 33.7% believed it was pain that occurred regardless of background pain.
In a feasibility study, 4 the authors endorsed the World Health Organization’s 42 definition of breakthrough pain as ‘a temporary increase in the severity of pain over and above the pre-existing baseline pain level’. Although a breakthrough pain data extraction instrument was developed, a pilot test showed poor agreement between raters when using it and there was no consensus on the terminology or definition of breakthrough pain to be used when reviewing paediatric narrative clinical records.
Expert group consensus studies
There were five expert group consensus studies, all using a 2-round Delphi method. 43 The experts involved were 64 pain specialists from pain units, palliative care, oncology, and geriatric medicine; 44 90 cancer pain experts from pain units, palliative/home care, and oncology; 45 69 oncology experts; 46 24 authors who had published three or more articles on breakthrough pain in cancer in the past 10 years; 47 and 76 cancer pain experts from pain units, palliative care, and oncology. Only one study, which was focused on breakthrough pain in older adults, 44 stated whether experts specialised in adults or paediatrics. The aim of the studies was to reach a consensus on the definition,45,47,48 diagnosis,45,48 and/or management44–46,48 of breakthrough pain in adults with cancer.
One study did not endorse a breakthrough pain definition. 44 One 48 reported that experts endorsed the Science Committee of the Association for Palliative Medicine of Great Britain and Ireland 7 definition of breakthrough pain as a transient exacerbation of pain that occurs either spontaneously or in relation to a specific predictable or unpredictable trigger, despite relatively stable and adequately controlled background pain. The experts believed that background pain controlled with around-the-clock (ATC) analgesics was a necessary diagnostic criterion for breakthrough pain. Experts in a more recent Delphi study 46 endorsed a similar definition of breakthrough pain as an ‘acute exacerbation of high intensity pain of short duration and rapid onset, suffered by a patient whose baseline pain is stabilised and controlled by opioids’.
Most experts in a 2016 Delphi study 45 endorsed the definition of breakthrough pain as ‘the occurrence of spontaneous or incidental exacerbations of pain’ on a background of controlled baseline pain though only 50% believed that patients must be taking regular analgesics to achieve this. Experts in this study did not believe that end-of-dose failure was a subtype of breakthrough pain and end-of-dose failure was not mentioned in the remaining Delphi studies.
In contrast to the other Delphi studies, the majority of the European Association for Palliative Care Research Network 47 reported that transient cancer pain exacerbation was possible without controlled background pain or without significant background pain at all. Thus, the network proposed that the term ‘episodic pain’ could be used as an overarching concept for all significant transient cancer pain exacerbations.
Narrative expert reviews
There were 24 expert narrative reviews concerning adult cancer patients (n = 5), patients with cancer (without specifying ages; n = 13), and patients with cancer or non-malignant conditions (n = 2). Four reviews did not state the population. Data on breakthrough pain definitions and descriptions endorsed in expert narrative reviews are shown in Supplementary File 5.
Breakthrough pain descriptions and classifications
Empirical studies with patients
Location
Across studies, patients indicated that they most commonly experienced breakthrough pain in their back.9,21–23,36,49 Other locations included head/face/mouth,9,21,22 abdomen,21,22,24,25,36 leg(s),9,21–23,25 arm(s),9,21,22 neck/shoulder(s),9,21,22 glutes/hip(s)pelvis,21,23,25 rectum or anus, 21 feet, 21 and ribs/chest.22,25
Severity
In most studies, severity was rated on a 0–10 numerical rating scale. Most patients rated their pain as 7–8/10.21,23,27,28,30,31,37,49–52 In three studies, the average pain intensity for most patients was <7/10 (4–6/10, 51 5.9/10 9 and 6/10 53 ). Average pain intensity was 8.5/10 in one study. 36 When patients were asked to rate whether their breakthrough pain was mild, moderate, or severe, the vast majority rated this as severe.22,33–35,54–56 In qualitative studies,25,26 patients described their pain as ‘severe’, ‘excruciating’, and one described difficulties rating their pain on a numerical rating scale. 26
Quality
The most common breakthrough pain descriptors were sharp, burning, and stabbing.21,27,32,36,49 Other descriptions included pressure/squeezing/tight,21,49 aching,21,49 radiating/shooting,21,49 crampy,21,49 throbbing,21,25,49 penetrating, 30 heavy,30,36 splitting, 36 spasm, 49 squeezing, 49 crushing, 25 and pressing. 49 One patient stated that breakthrough pain feels like ‘pulling, like my nerves are being stretched’ (p.55525). Some patients used more emotional terms such as exhausting, 30 punishing-cruel, and fearful. 36
Temporality
The most common average number of breakthrough pain episodes/day was 2–3.21,36,49,51,52 However, patients in other studies reported on average 1.3, 55 2,9,50 3,34,35 3–4,22,28 4,29,33,53 4–5, 57 5, 54 or 6 56 episodes/day. Episodes typically lasted between 11 and 60 min though many patients experienced episodes of shorter or longer duration.23,36,37,51,52,56 Average episode lengths included 30,33,49 32.1, 54 40.6, 22 45, 9 47.5, 57 52, 21 60,34,35 and 81.2 min 55 The average time to peak intensity ranged from <5 to 30 min 37 (including 1–2, 55 within 3, 33 109,34 or up to 10 min, 50 and 15 min)35,49 but was most commonly 5–10 min36,52,57 When asked to describe onset, more patients stated that their breakthrough pain had a gradual than a sudden onset in three studies25,28,56 while the reverse was found in one other study. 22
Subtypes
In seven reviews,21,22,34–37,49 patients’ breakthrough pain was described as incident, spontaneous, or a combination, of which incident breakthrough pain was the most common followed by spontaneous. Authors of three reviews28,29,58 included a third subtype; end-of-dose failure, which typically only occurred in a minority of patients. In three studies, incident breakthrough pain was subclassified into predictable, unpredictable, or a combination, with the majority being unpredictable.22,49,57 Four studies classified incident breakthrough pain (from most to least common) into volitional, non-volitional, a combination, and procedural.34–37 Patients’ breakthrough pain was classified into nociceptive (somatic or visceral), neuropathic, or a combination in eight studies,22,23,33,36,50,51,56 of which nociceptive or a combination was the most common.
Exacerbating factors
Patients cited the following exacerbating factors: movement/walking,25,27,33,36,49,54,56 standing,27,36,59 lying down,25,36,52 sitting,25,36,52,59 household/everyday activities,27,49,57 eating,24,52,57,59 bodily movements (e.g. swallowing, urination, and defecation),54,57 non-volitional activities such as coughing,25,28,33,36,54,56 touch, 54 stress/anxiety,54,59 cold/the weather, 59 treatment side-effects,24,28,54 the disease process,28,52,59 or an unidentifiable reason.8,27,28,54,59 The most commonly cited of these were walking/movement, coughing, and no identifiable reason.
Impact of breakthrough pain
Most patients reported breakthrough pain stopped them doing things and interfered with every aspect of life.32,34,35 Patients reported moderate-high interference in everyday life from breakthrough pain (when a 0–10 scale was used to measure this, the mean score was 5–10/10) for general activity,9,27,35,36,49,59,60 walking,9,27,35,36,49,59,60 work,8,9,27,36,49,59,60 relationships,8,9,27,36,49,59,60 sleep,8,9,27,36,49,59,60 mood,8,27,35,36,59,60 and enjoyment of life.8,9,27,35,36,49,59,60 Physical functioning was significantly worse for patients with breakthrough pain versus without breakthrough pain 59 and was worse in breakthrough pain patients with more frequent and/or longer lasting episodes. 51 Patients with breakthrough pain also reported higher levels of anxiety9,49,59 and depression9,59 and worse mental wellbeing32,49 and quality of life 22 compared to those without breakthrough pain. In qualitative studies, patients reported having to change their lifestyle and limit their movement to reduce the pain.24–26 They described feeling sad, depressed, hopeless, helpless, and even suicidal.24–26 In one study, patients reported a lack of control over their body. 26
Empirical studies with clinicians
No empirical studies with clinicians included data on breakthrough pain location, subtypes, or classifications. Nurses in two studies estimated breakthrough pain severity as moderate-severe (7 or 8/10 40 ) or as not severe (0.1%), mild (0.6%), moderate (19.5%), or severe (75.5%). 38 The quality of breakthrough pain was described by clinicians in one study as ‘increased pressure in head’, pins and needles, achiness, headache, cramps, spasms, or stiffness. 4
Half of nurses in one study estimated that breakthrough pain occurred at least twice a day, 13% estimated one episode or less per day and 37% were unsure. The majority estimated time to peak intensity of 11–20 min with episodes lasting 31–60 min but many unsure. 40 Another study with nurses reported that they had patients who experienced breakthrough pain less than once a day (9%), once a day (13.9%), 2–3 times a day (46.6%), or >3 times a day (16.4%); 14.1% did not know. 38 Clinicians in a study that involved generating information from paediatric narrative clinical records noted that pain might be breakthrough pain if it has a rapid onset. 4
Exacerbating factors noted in one study by nurses included movement, the existing condition, treatment, and eating, 38 Data on interference due to breakthrough pain was present in the two studies with nurse participants. Nurses reported breakthrough pain caused some (55.2%) or complete (43.6%) interference with patients’ everyday activities 40 and that it specifically interfered with patients’ enjoyment of life, work, mood, sleep, movement, general activity, and relationships. 38 In both studies with nurse participants, breakthrough pain was viewed as having a significant impact on quality of life.38,40 Clinicians in the only paediatric study felt that descriptors that could indicate breakthrough pain included ‘disturbed sleep’, ‘unsettled’, ‘irritation’, and ‘distress’. 4
Expert group consensus studies
Breakthrough pain location, quality, subtypes, exacerbating factors, interference, and psychological issues were not mentioned in the expert group consensus studies. One consensus study 45 specified the level of pain severity (≥7/10 on a 0–10 rating scale) for pain to be diagnosed as breakthrough pain. In another study, 47 experts agreed that breakthrough pain intensity must be more than two points higher than background pain on a 0–10 rating scale but did not agree that breakthrough pain can best be assessed by an increase in pain score to a predefined number.
Statements on the frequency of breakthrough pain episodes were rated in only one study. 46 Consensus was not reached regarding whether breakthrough pain diagnosis requires >4 episodes/day, though experts’ comments suggested that they did not agree with establishing a minimum number of episodes since a single episode could be diagnosed as breakthrough pain. Experts in one study 45 agreed that breakthrough pain episodes last <60 min. Episode length was not discussed in the remaining studies.
Discussion
This rapid systematic review aimed to update and expand upon Haugen and colleagues’ 12 review of cancer breakthrough pain assessment and classification. We identified 65 highly heterogenous studies of varying quality that included data on breakthrough pain definitions, descriptions, and classifications reported by patients (n = 30), clinicians (n = 6), and experts (n = 29). These were five expert group consensus studies, 24 expert narrative reviews, and 37 empirical studies.
In only one study 26 were patients asked about their views on the meaning of breakthrough pain, the term was poorly understood and they found it hard to distinguish breakthrough pain from background pain. In eight studies, the definition of breakthrough pain used as patient inclusion criteria was not operationally defined.
In empirical studies with clinicians, most endorsed the broad definition of breakthrough pain as a severe, rapid-onset, and short-lived pain occurring in patients with controlled mild-moderate background pain. However, results showed that a lack of knowledge and confidence in defining breakthrough pain was common in oncology nurses and palliative care doctors. There was also poor consensus in identifying breakthrough pain in paediatric clinical records by clinicians. 4
Across studies, experts typically endorsed the broad definition of breakthrough pain above. Breakthrough pain can be incident, spontaneous, predictable, or unpredictable and may be the same pain as background pain, or different. Exceptions to this definition included two expert narrative reviews proposing that breakthrough pain could be only moderate-severe61,62 and one suggesting that breakthrough pain could occur in patients with treated or untreated background pain. 63 Significantly, the European Association for Palliative Care Research Network 47 proposed that breakthrough pain could occur without any background pain and thus the term ‘episodic pain’ should be used instead to cover all significant transient cancer pain exacerbations. The EAPC Research Network 64 also suggested ‘episodic pain’ should replace ‘breakthrough pain’, while an expert review proposed the term ‘incident pain’ should be used instead. 65 However, these changes have been debated66,67 and not yet been implemented in the literature.
Breakthrough pain descriptions and characteristics were broadly in alignment across studies though temporal features varied widely. For example, the average length of a breakthrough pain episode was stated as ranging between <5 min to ‘many hours’ by experts, while the average length stated by patients ranged from 11 to >80 min. Similarly, the average number of episodes per day ranged from 1 to 7.44 (experts) and 1–6 (patients) with some experts stating that >4 episodes/day indicated poorly controlled background pain rather than breakthrough pain. Many patients with chronic cancer or noncancer pain on ATC opioids experience end-of-dose pain and an enduring debate in the literature is whether end-of-dose failure is actually a type of BTP. However, few studies mention end-of-dose pain explicitly and a systematic review to examine how the frequency of end-of-dose pain is linked to the formulations of long-acting opioids had to use ‘breakthrough pain’ as a surrogate parameter. 68
As this was a rapid systematic review, study quality assessment focused only on the review’s primary objectives, using a bespoke study quality assessment based on previous tools.18–20 Quality assessment outcomes may be different if a more in-depth assessment tool was used. While the current review did not aim to identify BTP assessment tools, we conducted an extensive systematic review of BTP assessment tools in 2021.13,14 The current review expanded on Haugen and colleagues’ work by including all types of BTP, not just cancer-related BTP. Moreover, 30 of the 65 included studies in the current review were published after the first BTP review, indicating the growth of this field and the need for an updated review.
Thirteen years after Haugen and colleagues review, 12 it is striking that a very similar range of overlapping but different breakthrough pain definitions were found, with no single broadly accepted definition. This is despite proposals for a universal definition from expert groups including the European Association for Palliative Care Research Network. 47 Breakthrough pain is a significant problem for the majority of patients with cancer and those at end-of-life1,2 As findings from this review demonstrate, it has a profound impact on patients’ functioning, mental, and physical wellbeing. However, clinicians demonstrate a lack of confidence in defining breakthrough pain, which likely leads to underdiagnosis and undermanagement. Minor variations to the definition and a reluctance to endorse one definition in the literature perpetuate these problems.
The current review found no studies asking caregivers on their views on breakthrough pain, and only one that included paediatric patients. There is a need for more research on paediatric breakthrough pain since it is not clear if or how breakthrough pain may differ in children versus adults. Evidence suggests it is common in children with life-limiting conditions, including cancer, and at end-of-life.4,6 Moreover, children and their families report that breakthrough pain is a major concern, often describing it as ‘intolerable’ or ‘out of control’. 69
A compromise on breakthrough pain nomenclature achieved via appropriate methodology is needed to reach a consensus, defined in this context as the position generally agreed upon at a given time by most scientists specialised in a given field, based on their interpretation of the available evidence. 70 There are three best known consensus methods that try to push a field towards consensus on important clinical issues, that is, the Delphi process, the nominal group technique (also known as the expert panel), and the consensus development conference. In the case of breakthrough pain, despite the fact that some of these methods have been employed, as our systematic review clearly demonstrates, no consensus has been achieved and researchers and clinicians continue to endorse different definitions in their everyday clinical practice, research, and writing. 70 The current review showed a minimum level of agreement on the definition in the literature that aligns closely with the definition of breakthrough pain as ‘a temporary increase in the severity of pain over and above the pre-existing baseline pain level’. 42 A universal working definition would allow for the collection of reliable incidence and prevalence data, inform the development and validation of breakthrough pain assessment tools for different patient populations, allow for further refinement of the construct if needed and ultimately, and improve breakthrough pain diagnosis and management. To summarise, the present systematic review is a small first step towards achieving eventual consensus in a definition of breakthrough pain by demonstrating the magnitude of the problem and providing a comprehensive and exhaustive summary of different definitions. Future research such as BEACON is now needed involving all key stakeholders, that is, patients, caregivers, clinicians, and researchers, in order to achieve a universal working definition.
Supplemental Material
Supplemental Material - A rapid systematic review of breakthrough pain definitions and descriptions
Supplemental Material for A rapid systematic review of breakthrough pain definitions and descriptions by Katie Greenfield, Daniel E Schoth, Richard Hain, Simon Bailey, Christine Mott, Dilini Rajapakse, Emily Harrop, Kate Renton, Anna-Karenia Anderson, Bernie Carter, Margaret Johnson, and Christina Liossi in British Journal of Pain
Supplemental Material
Supplemental Material - A rapid systematic review of breakthrough pain definitions and descriptions
Supplemental Material for A rapid systematic review of breakthrough pain definitions and descriptions by Katie Greenfield, Daniel E Schoth, Richard Hain, Simon Bailey, Christine Mott, Dilini Rajapakse, Emily Harrop, Kate Renton, Anna-Karenia Anderson, Bernie Carter, Margaret Johnson, and Christina Liossi in British Journal of Pain
Supplemental Material
Supplemental Material - A rapid systematic review of breakthrough pain definitions and descriptions
Supplemental Material for A rapid systematic review of breakthrough pain definitions and descriptions by Katie Greenfield, Daniel E Schoth, Richard Hain, Simon Bailey, Christine Mott, Dilini Rajapakse, Emily Harrop, Kate Renton, Anna-Karenia Anderson, Bernie Carter, Margaret Johnson, and Christina Liossi in British Journal of Pain
Supplemental Material
Supplemental Material - A rapid systematic review of breakthrough pain definitions and descriptions
Supplemental Material for A rapid systematic review of breakthrough pain definitions and descriptions by Katie Greenfield, Daniel E Schoth, Richard Hain, Simon Bailey, Christine Mott, Dilini Rajapakse, Emily Harrop, Kate Renton, Anna-Karenia Anderson, Bernie Carter, Margaret Johnson, and Christina Liossi in British Journal of Pain
Supplemental Material
Supplemental Material - A rapid systematic review of breakthrough pain definitions and descriptions
Supplemental Material for A rapid systematic review of breakthrough pain definitions and descriptions by Katie Greenfield, Daniel E Schoth, Richard Hain, Simon Bailey, Christine Mott, Dilini Rajapakse, Emily Harrop, Kate Renton, Anna-Karenia Anderson, Bernie Carter, Margaret Johnson, and Christina Liossi in British Journal of Pain
Footnotes
Author contributions
CL conceived the idea; KG, DES, and CL planned and designed the study protocol, search strategy, data extraction and quality assessment, and wrote the first draft; RH, SB, CM, DR, EH, KR, A-K A, BC, and MJ provided critical insights. All authors have approved and contributed to the final written manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Great Ormond Street Children’s Charity (grant number: V5118 and V4421).
Supplemental Material
The Supplementary Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.