
Abstract
Objective
The sedative effects of dexmedetomidine (Dex) are similar to natural sleep, with easy wakening following Dex administration, and Dex has minor effects on breathing, reducing emergence agitation in children. The aim of this study was to systematically evaluate the effects of Dex on recovery quality in children following general anaesthesia with sevoflurane, to aid clinical decision making.
Methods
Relevant randomized controlled trials published before August 2019 were searched and selected from databases. Two researchers independently screened the literature, extracted data, and assessed included studies for bias risk. Meta-analysis was performed using Stata 14.0 software.
Results
The study included 24 publications. Following general anaesthesia by sevoflurane, Dex was associated with reduced occurrence of emergence agitation (odds ratio [OR] 0.16, 95% confidence interval [CI] 0.11, 0.25) and nausea and vomiting (OR 0.40, 95% CI 0.24, 0.60), along with shortened eye-opening time (standardized mean difference [SMD] 0.72, 95% CI 0.41, 1.03), shortened extubation time (SMD 0.54, 95% CI 0.28, 0.81), and reduced duration of post-anaesthesia care unit (PACU) stay (SMD 0.29, 95% CI 0.08, 0.51) versus placebo.
Conclusion
Dexmedetomidine has positive effects on recovery quality in children undergoing general anaesthesia with sevoflurane.
Introduction
Sevoflurane has the advantages of limited respiratory stimulation and rapid onset and arousal time, and is widely used in paediatric anaesthesia. 1 However, emergence agitation is a common complication in children during the recovery period after general anaesthesia with sevoflurane, and can lead to unexpected injury. 2 Emergence agitation is a state of disturbance during recovery from general anaesthesia that includes hallucinations and delusions with convulsions, crying, swaying, and kicking in bed. These symptoms mainly appear within 30 minutes following surgery, particularly during the first 5–15 minutes. 2 Drugs that may be used to reduce agitation during general anaesthesia currently include propofol, midazolam and dexmedetomidine (Dex). 3 Propofol and midazolam can inhibit breathing and increase the risk associated with general anaesthesia in children.3,4 Dex acts on the α2-adrenergic receptors of the locus coeruleus and has sedative, analgesic and anti-sympathetic effects without inhibiting breathing. 3 Dex is reported to be safe and effective during general anaesthesia with sevoflurane in children,4–9 but this conclusion remains controversial due to a lack of large-scale, multicentre research. Although Amorim et al. 10 conducted a systematic review of studies published between 2000 and 2014, their analysis lacked rigor (only one database was screened), and the time to publication exceeded the Cochrane Collaboration regulation for systematic reviews (updated every two years); 11 Moreover, new RCTs have been reported since. Therefore, the aim of the present study was to systemically evaluate the effects of Dex on recovery quality following general anaesthesia with sevoflurane, to provide evidential support for clinical decision making.
Materials and methods
This review was conducted in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines and the recommendations of the Cochrane Collaboration.12,13 The study did not require approval from an institutional ethics review board, and as it did not involve human participants, informed consent was not required.
Search strategy
Relevant randomized controlled trials (RCTs) published before August 2019 were searched and selected from the Web of Science, EMbase, PubMed and Cochrane Library databases. Search keywords were ‘dexmedetomidine’, ‘children’ and ‘sevoflurane’, and searching was based on the combination of a single word and subjective word. There were no language restrictions. Once duplicates had been removed, all retrieved articles were screened by reading titles and abstracts. The full texts of the remaining potentially relevant studies were then examined for further suitable evaluations in the present meta-analysis. Furthermore, to identify additional eligible studies, the references of related studies were manually searched. The meta-analyses only included primary publications of studies, and did not include RCTs that had been reproduced in other studies.
Inclusion criteria for the present study: (1) publication type, RCT; (2) study population, children undergoing general anaesthesia with sevoflurane; (3) intervention, patients in the experiment group were administered a single or continuous intravenous infusion or nasal infusion of Dex during the perioperative period, and patients in the control group were administered saline instead of Dex; and (4) evaluation criteria, occurrence of emergence agitation, occurrence of nausea and vomiting, eye-opening time (or anaesthesia recovery time), extubation time (or mask-removal time) and duration of postanaesthesia care unit (PACU) stay.
Exclusion criteria comprised the following: (1) publications without relevant assessment criteria or acquirable data; (2) repeated publications; (3) single case reports; (4) systematic reviews and meta-analyses; and (5) animal experiments.
Data extraction
Two researchers (DWH and YLL) independently screened and reviewed the literature and extracted the data; if there was disagreement, a third researcher (WT) was consulted for advice. Data regarding author details, publication date, country, dose of Dex and administration method, number and age of patients, operation type, incidence of emergence agitation, nausea and vomiting, eye-opening time, extubation time, and duration of PACU stay were extracted.
Quality assessment
The risk of bias was assessed based on an evaluation method recommended in the Cochrane handbook for systematic reviews of interventions, version 5.1.0 (2011 update). The main procedure included the following items: (1) randomization strategy; (2) allocation concealment; (3) blinding (participants and personnel or outcome assessment); (4) incomplete data reporting; (5) reporting of selective results; and (6) origin of other bias. For each study, the items were marked as ‘high’, ‘low’ or ‘unclear’ risk.
Statistical analyses
Meta-analyses were performed using Stata software, version 14.0 (STATA Corporation, College Station, TX, USA). Statistical results from comparison of two-category data are presented as odds ratios (ORs) and 95% confidence intervals (CIs). Statistical results for continuous data are presented as standardized mean difference (SMD). Heterogeneity between the included studies was analysed using χ2-test (test level α = 0.1), and I2 was used to quantitatively determine the size of heterogeneity. When P < 0.1 and/or I2 > 50%, the random-effects model was used for the combined analysis; otherwise, the fixed-effects model was used for the combined analysis. Sensitivity analysis was used to assess the origin of heterogeneity. Subgroup analyses were performed based on overall sample size (<80 cases or >80 cases). The potential publication bias and small sample bias were evaluated by drawing a funnel plot, including Egger’s and Begg’s methods. All P values were two-sided, and a P value < 0.05 served as the threshold for statistical significance.
Results
Description of studies
A total of 537 articles were obtained through relevant database searches and article screening, and 82 duplicate articles were excluded. Titles and abstracts of the 455 remaining articles were screened, and 418 were excluded, leaving 37 full-text articles to be reviewed. A further 13 articles were excluded at this stage, resulting in 24 publications for inclusion in the present study, shown in the selection flow chart (Figure 1).4–9,14–31 All 24 studies were included in the qualitative synthesis and meta-analysis. Basic characteristics of the publications and risk of bias assessment results are shown in Table 1 and Figures 2 and 3. Two of the trials comprised four-arm tests,6,9 each of which was split into three lots of two-arm tests, and four of the trials comprised three-arm tests,7,23, 24 , 27 each of which was split into two lots of two-arm tests for the purpose of the present analyses. In addition, there were four5,14, 18 , 28 three-arm trials comparing the efficacy of Dex, other drugs and saline. The groups that investigated Dex and saline placebo were selected for the present study.

Flowchart of selection of studies for inclusion in qualitative review and meta-analysis.
Description of 24 randomised controlled trials included in the present systematic review and meta-analyses.

T, treatment group; C, control group; mo, month; y, years; Dex, dexmedetomidine.

Summary of proportional risk of bias in 24 randomised controlled trials included in the review.

Risk of bias in each of the 24 included randomised controlled trials; green circle with ‘+’ sign, low risk; yellow circle with ‘?’ sign, unclear risk.
Quantitative synthesis
Twenty-four RCTs reported the incidence of emergence agitation,4–9,14–31 I2 = 71.7% (P < 0.001), and these were combined using a random-effects model. Dex was found to be associated with reduced incidence of emergence agitation versus placebo (OR 0.16, 95% CI 0.11, 0.25; P < 0.001; Figure 4 and Table 2). There was no source of heterogeneity according to sensitivity analysis (Figure 5), which meant this result was relatively stable. Subgroup analysis revealed that sample size was the main source of heterogeneity (Table 3).

Forest plot showing the effect of dexmedetomidine on emergence agitation in children undergoing general anaesthesia with sevoflurane.
Analysis results of each outcome indicator.

PACU, post-anaesthesia care unit; R, random-effects model; F, fixed-effects model; OR, odds ratio; SMD, standardized mean difference; CI, confidence interval.
NS, not statistically significant (P > 0.05).
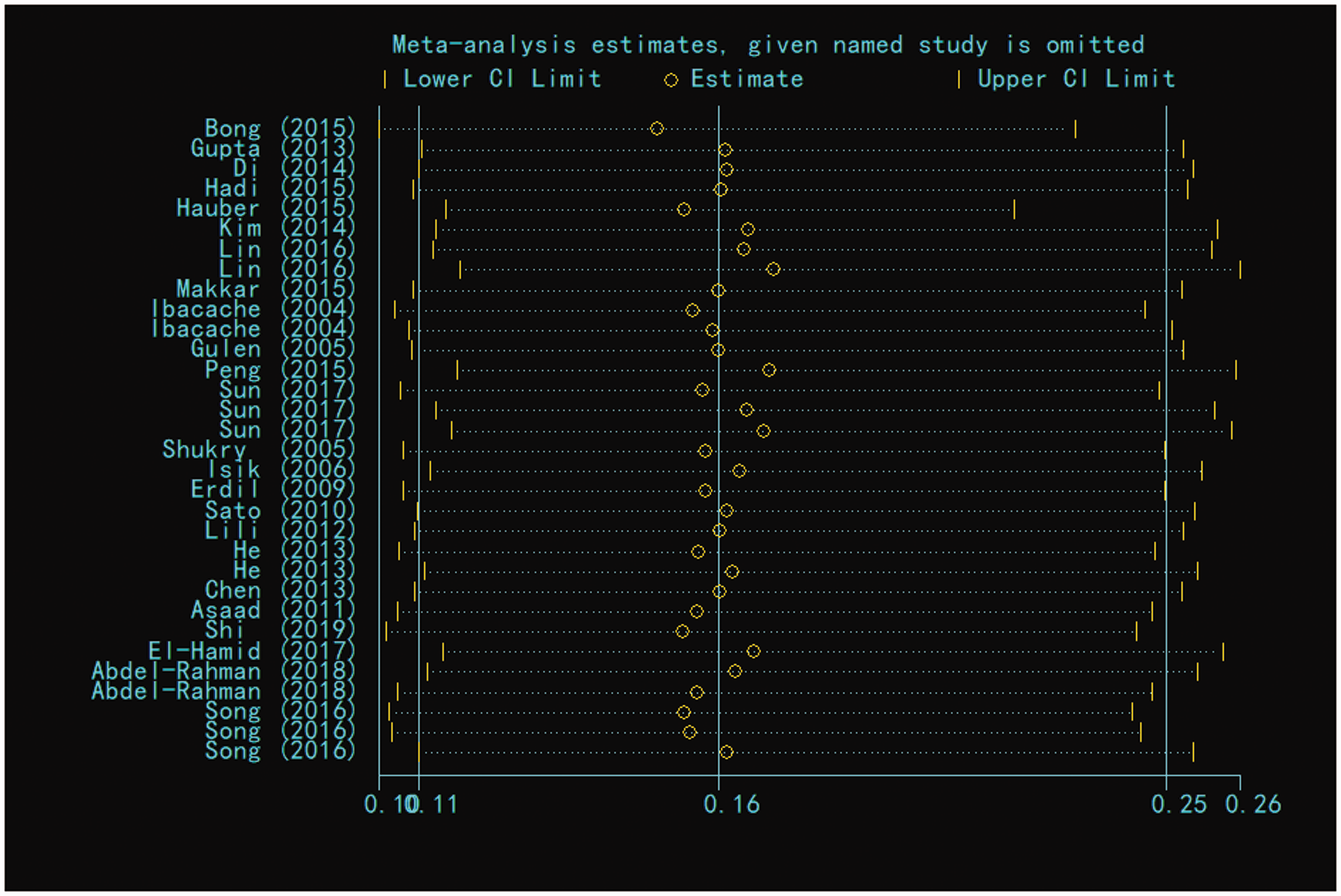
Sensitivity analysis for emergence agitation in children undergoing general anaesthesia with sevoflurane.
Subgroup analysis of each outcome indicator.
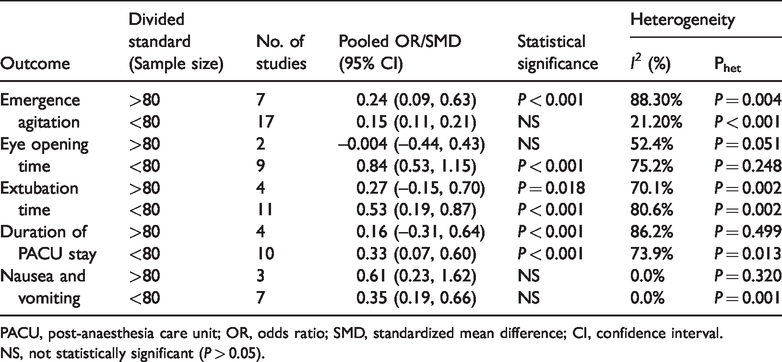
PACU, post-anaesthesia care unit; OR, odds ratio; SMD, standardized mean difference; CI, confidence interval.
NS, not statistically significant (P > 0.05).
Thirteen RCTs reported the eye-opening time, 5 , 7 , 9 , 14 , 15 , 18 , 19 , 24 , 25 , 28 , 29 I2 = 79.9% (P < 0.001), and these were combined using a random-effects model. Dex was found to be associated with reduced eye-opening time versus placebo (SMD 0.72, 95% CI 0.41, 1.03; P < 0.001; Figure 6 and Table 2). There was no source of heterogeneity according to sensitivity analysis (Figure 7), which meant this result was relatively stable. Subgroup analysis revealed that sample size was the main source of heterogeneity (Table 3).

Forest plot showing the effect of dexmedetomidine on eye opening time in children undergoing general anaesthesia with sevoflurane.

Sensitivity analysis for eye opening time in children undergoing general anaesthesia with sevoflurane.
Fifteen RCTs reported the extubation time, 4 , 6 , 8 , 9 ,15–21, 25 , 26 , 29 , 31 I2 = 78.5% (P < 0.001), and these were also combined using a random-effects model. Dex was found to be associated with reduced extubation time versus placebo (SMD 0.54, 95% CI 0.28, 0.81; P < 0.001; Figure 8 and Table 2). There was no source of heterogeneity according to sensitivity analysis (Figure 9), which meant this result was relatively stable. Subgroup analysis revealed that sample size was the main source of heterogeneity (Table 3).
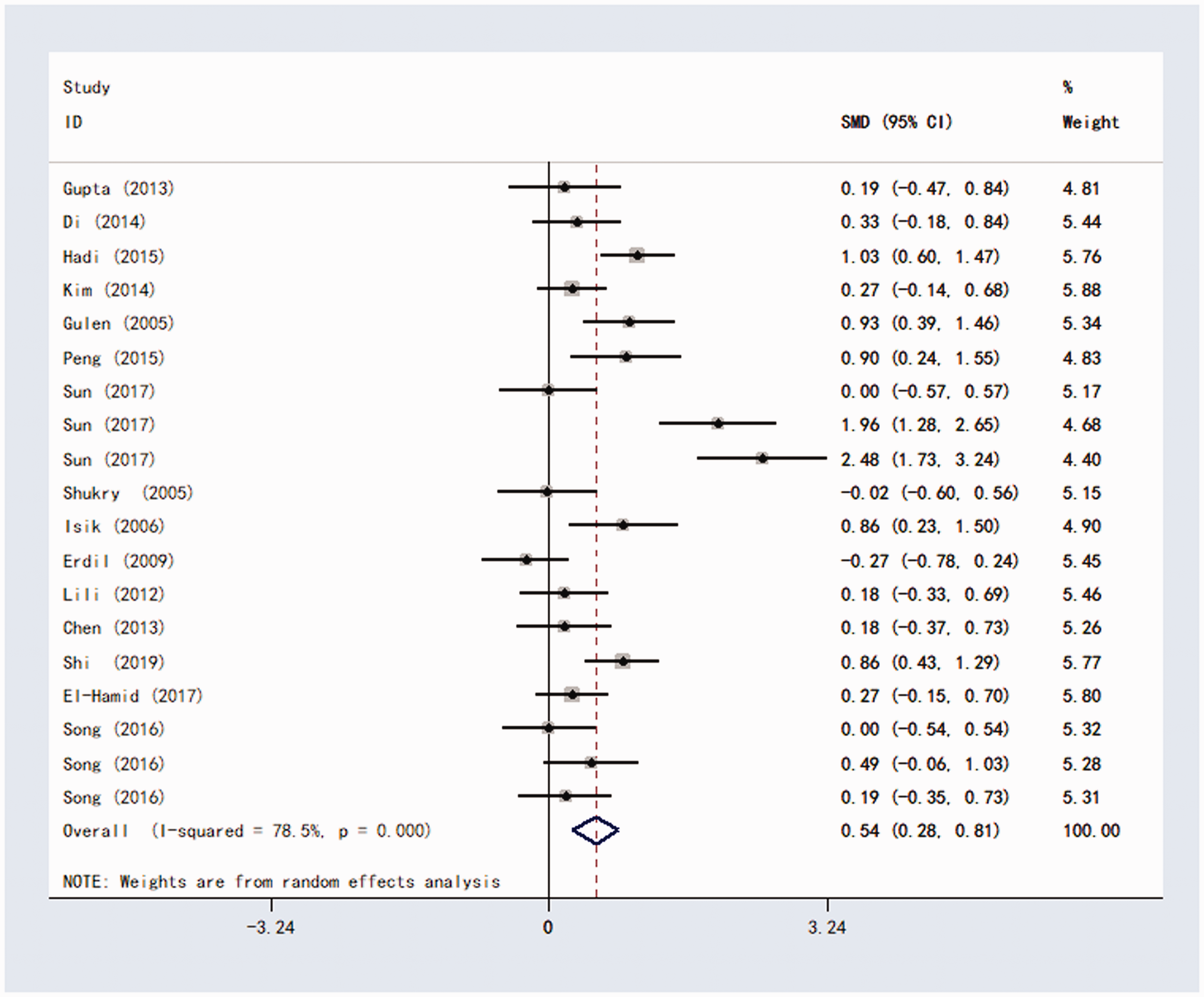
Forest plot showing the effect of dexmedetomidine on extubation time in children undergoing general anaesthesia with sevoflurane.

Sensitivity analysis for extubation time in children undergoing general anaesthesia with sevoflurane.
Fifteen RCTs reported the duration of PACU stay, 6 , 7 , 9 , 15 , 16 , 21 , 22 , 24 , 25 , 27 , 29 , 31 I2 =76.1% (P < 0.001), which were combined by using a random-effects model. Dex was found to be associated with reduced duration of PACU stay versus placebo (SMD 0.29, 95% CI 0.08, 0.51; P = 0.008; Figure 10 and Table 2). Sensitivity analysis suggested that Hauber et al (2015) 22 was a source of heterogeneity. After checking the basic publication information, this study was found to have a relatively larger sample size, which was the reason for heterogeneity (Figure 11), and subgroup analysis revealed that sample size was the main source of heterogeneity (Table 3).
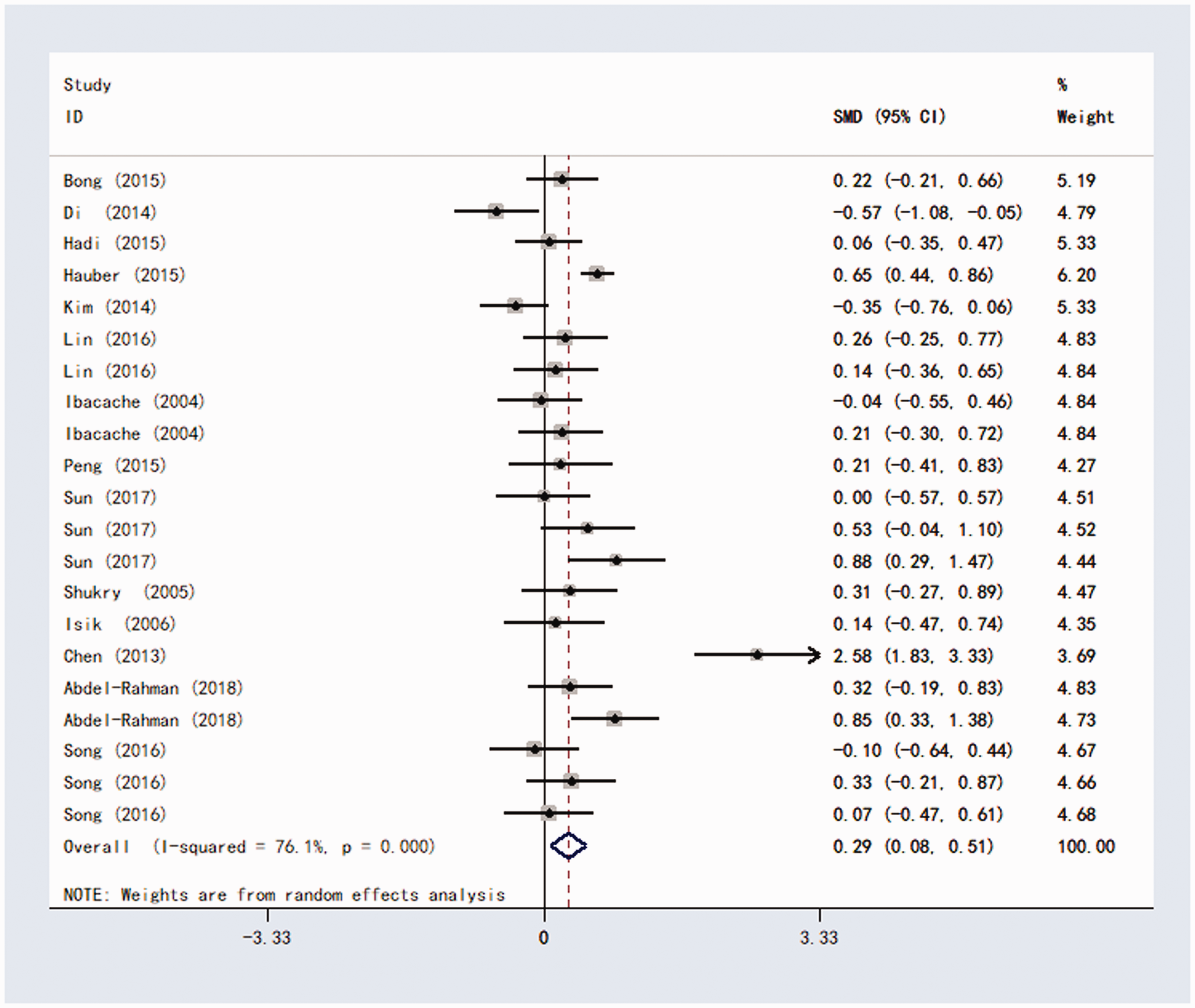
Forest plot showing the effect of dexmedetomidine on duration of post-anaesthesia care unit stay in children undergoing general anaesthesia with sevoflurane.

Sensitivity analysis for duration post-anaesthesia care unit stay in children undergoing general anaesthesia with sevoflurane.
Ten RCTs reported the incidence of nausea and vomiting, 4 , 6 , 8 ,15–20, 30 I2 = 0.0%, P = 0.898, and their results were combined using a fixed-effects model. Dex was revealed to be associated with reduced incidence of nausea and vomiting versus placebo (OR 0.40, 95% CI 0.24, 0.60; P = 0.001; Figure 12 and Table 2). Sensitivity analysis revealed that this result was relatively stable (Figure 13), and subgroup analysis found no change in I2 (Table 3).

Forest plot showing the effect of dexmedetomidine on nausea and vomiting in children undergoing general anaesthesia with sevoflurane.

Sensitivity analysis for nausea and vomiting in children undergoing general anaesthesia with sevoflurane.
Publication bias
Publication bias was evaluated using Egger’s and Begg’s methods. Bias was found regarding emergence agitation and eye-opening time, however there was no bias found in relation to nausea and vomiting, extubation time or duration of PACU stay (Figures 14–18 and Table 2).

Begg’s funnel plot of studies showing the effect of dexmedetomidine on emergence agitation in children undergoing general anaesthesia with sevoflurane.
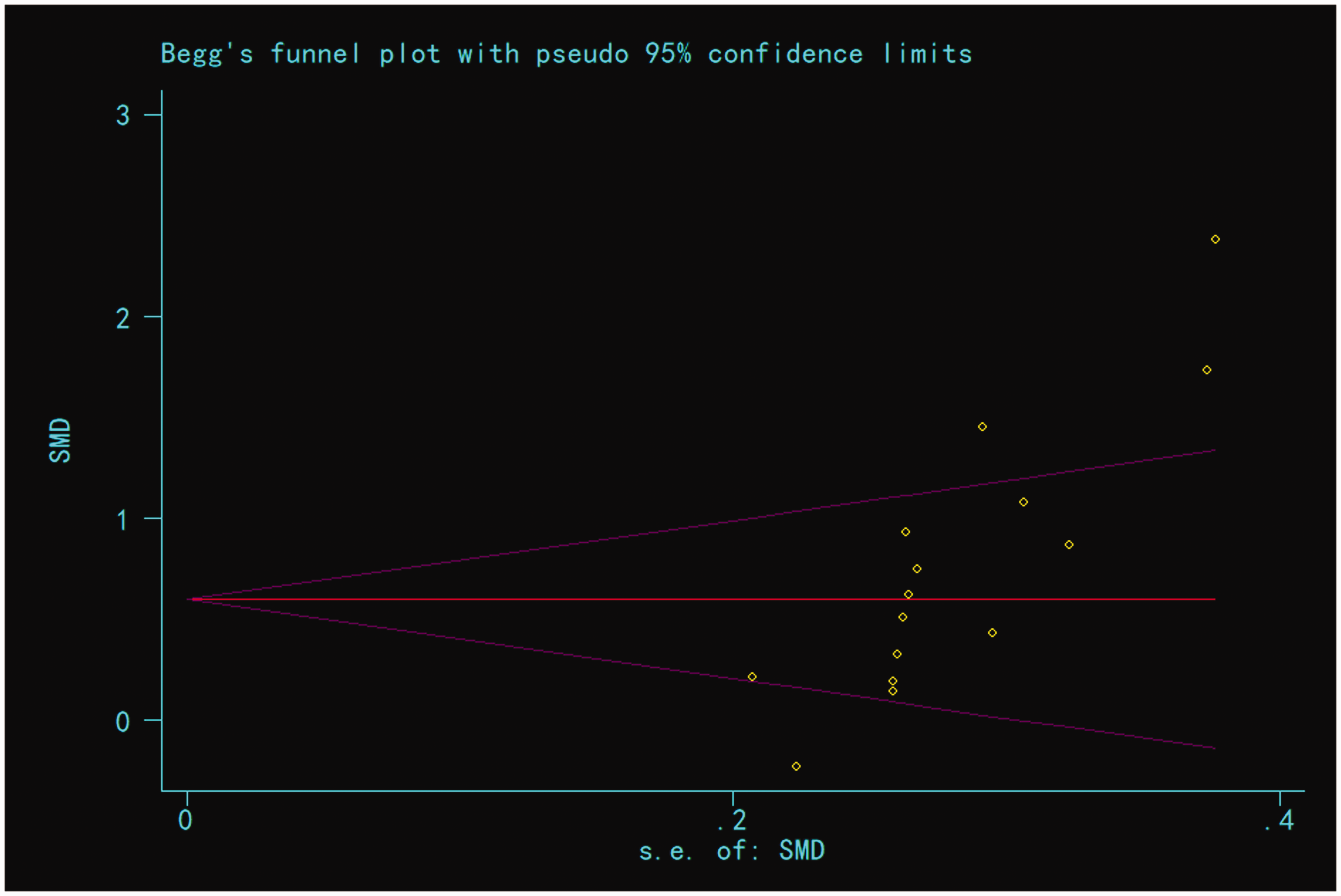
Begg’s funnel plot of studies showing the effect of dexmedetomidine on eye opening time in children undergoing general anaesthesia with sevoflurane.

Begg’s funnel plot of studies showing the effect of dexmedetomidine on extubation time in children undergoing general anaesthesia with sevoflurane.

Begg’s funnel plot of studies showing the effect of dexmedetomidine on duration of post-anaesthesia care unit (PACU) stay in children undergoing general anaesthesia with sevoflurane.

Begg’s funnel plot of studies showing the effect of dexmedetomidine on nausea and vomiting in children undergoing general anaesthesia with sevoflurane.
Discussion
A total of 24 RCTs were included in the present meta-analysis.4–9,14–31 The results showed that, compared with placebo, Dex was associated with positive effects on recovery quality in children undergoing general anaesthesia with sevoflurane, reducing nausea and vomiting and shortening the eye-opening time, extubation time, and duration of PACU stay. Unlike the present study, Amorim et al. 10 reported that Dex reduced the incidence of emergence agitation while prolonging the duration of PACU stay and eye-opening time. A potential explanation for this discrepancy is that the meta-analysis reported by Amorim et al. 10 only screened one database, so that only a limited number of publications were included; additionally, the sample size was relatively small. In a 2015 study that compared the effects of 0.3 µg/kg Dex, 1 mg/kg propofol and placebo on recovery and compliance in patients undergoing general anaesthesia, 5 the incidences of emergence agitation were found to be 42.5% (17/40), 33.3% (13/39) and 41.5% (21/41), respectively, and Dex or propofol did not significantly reduce the incidence or severity of emergence agitation, which was distinct from the former meta-analysis. The present meta-analysis used an updated systematic evaluation, included relevant RCTs from 2004–2019, and evidenced the positive effects of Dex on recovery quality in children undergoing general anaesthesia with sevoflurane.
Emergence agitation occurs during the beginning of anaesthesia recovery, and its clinical manifestations are related to various risk factors, such as age, paediatric anaesthesia behaviour score, surgery type, and anaesthesia duration. 32 Many anaesthesiologists have found that use of sevoflurane has a strong relationship with the occurrence of agitation, 15 and a previously published meta-analysis also confirmed that the incidence of agitation in patients who received sevoflurane was higher than in patients who received propofol. 33 It has been shown that the incidence of agitation in the recovery period following general anaesthesia with sevoflurane is 17–83%. 34 Although the duration of emergence agitation in children is short, emergence agitation increases the risk of self-harm and delayed discharge in children. 35
Dex is a highly selective agonist of α-adrenergic receptors, having sedative, analgesic and anxiolytic effects at clinical doses without affecting the patient’s breathing, 30 and it has been widely applied for anaesthesia in children. 7 , 8 , 36 Dex induces the activation of α2 receptors and stimulates blue-spot receptors, which can then affect the endogenous sleep pathway, mimicking the sedation that occurs in natural sleep. 37 , 38 Furthermore, α2 receptors in the spinal cord can also have certain analgesic effects, which will improve the recovery quality after general anaesthesia, probably by mainly reducing the occurrence of agitation during recovery. 31 The present meta-analysis revealed that, compared with placebo, the administration of Dex in children undergoing general anaesthesia was associated with a lower incidence of emergence agitation, and this result concurs with many previous studies. 6 , 8 , 10 , 30 , 31 Dex has limited effects on breathing, and as an adjunct to anaesthesia, Dex can reduce the amount of anaesthetic drugs, 39 to shorten the recovery time following general anaesthesia. The present meta-analysis found that eye-opening time, extubation time and duration of PACU stay were significantly reduced compared with placebo. In addition, the incidence of nausea and vomiting associated with sevoflurane anaesthesia is reported to be as high as 30%. 40 The present meta-analysis showed that the incidence of nausea and vomiting was significantly lower in the Dex group than in the placebo group, and these results were similar to those reported in the meta-analysis by Amorim et al. 10
The results of the present study may be limited by several factors. The meta-analysis mainly included publications in English, as there were few studies in other languages, and some valuable studies may have been ignored. Egger’s and Begg’s methods were used to assess publication bias, and bias was found. There was heterogeneity in the meta-analysis; and although an attempt to eliminate heterogeneity was made through subgroup analysis and sensitivity analysis, heterogeneity still existed. Due to the variations in patient age, surgery type, administration methods and drug dose in the included RCTs, heterogeneity is unlikely to be eliminated. Although the quality of the publications included in this meta-analysis was very high, the RCTs were conducted in different countries and hospitals; there were some differences in the choice of anaesthesia, surgical techniques, anaesthesia management and postoperative care; and the factors affecting the operations were distinct. Moreover, the time and method of administration also varied, and there was unavoidable bias. As such, the present results should be interpreted with caution, and further studies are required to validate the findings.
In conclusion, the present meta-analysis revealed that Dex is associated with positive effects on recovery quality in children undergoing general anaesthesia with sevoflurane, reducing nausea and vomiting and shortening the eye-opening time, time to extubation and duration of PACU stay compared with placebo. Dex was shown to have a positive effect on the quality of general anaesthesia recovery, however, due to the study limitations that may affect the strength of the arguments, this conclusion should be regarded with appropriate caution.