
Abstract
Background
We hypothesized that 3 weeks of preoperative rehabilitation could improve postoperative pain in patients undergoing total knee arthroplasty (TKA). Aim: This study aimed to evaluate the effects of 3 weeks of preoperative rehabilitation on postoperative pain after TKA.
Methods
This prospective cohort study included 29 subjects (41 knees) divided into two groups: the preoperative rehabilitation group included 14 subjects (20 knees) and the control group included 15 subjects (21 knees). All subjects were scheduled for unilateral or bilateral TKA. The preoperative rehabilitation group completed a 90-min rehabilitation program 3 days per week for 3 weeks before their TKA. The rehabilitation included body weight exercise, resistance exercise, and cycle ergometer exercise. The control group did not undergo any rehabilitation prior to TKA. We assessed the patients using Western Ontario and McMaster Universities’ Osteoarthritis Index (WOMAC) and recorded their physical activity of walking, standing, sitting, and lying down at study entry and/or before TKA and 1 month after TKA.
Results
The WOMAC total and WOMAC pain scores were significantly lower after 3-weeks of rehabilitation, but before TKA and 1 month after surgery were significantly lower in the preoperative rehabilitation group than in the control group. The time spent walking, standing, sitting, and lying down for 12 h did not change after TKA in the preoperative rehabilitation group. In contrast, in the control group, the time spent in walking and standing positions decreased and the time in the sitting position increased after TKA (p < 0.05). Conclusion: We found that 3-week preoperative training reduced knee pain and helped maintain physical activity after surgery in patients with severe osteoarthritis who underwent TKA.
Keywords
Introduction
Osteoarthritis (OA) is both the most common joint disease worldwide 1 and a major cause of knee pain and disability.2–4 Knee replacement surgery is highly successful in relieving knee pain and improving knee function in people with advanced arthritis of the joint. 5 However, some patients with OA experience postoperative pain after knee replacement surgery6,7 which can decrease their activity after surgery and lead to deep vein thrombosis (DVT) and pulmonary embolism (PE). 8 Weakness of the knee extensor muscle is a common finding in patients with OA and is associated with knee pain as well as reduced functional performance and daily activity.9–11 Several studies have reported the benefits of 4–8 weeks of preoperative rehabilitation before total knee arthroplasty (TKA) including improved knee muscle strength and reduced pre-operative knee pain.12–16 In addition, postoperative pain was reduced by high-intensity strength training for 8 weeks before TKA. 15 Additionally, a previous study reported that a 3-week resistance training program significantly increased lower body strength in healthy people. 17 Therefore, we hypothesized that 3 weeks of preoperative rehabilitation would improve postoperative pain in patients after TKA. If postoperative pain after TKA was reduced by 3 weeks of preoperative rehabilitation, this rehabilitation regimen could be useful for patients with knee OA because patients would be better able to maintain their activities after TKA and decrease the risk of DVT and PE. To the best of our knowledge, no studies have reported the effects of a 3-week preoperative rehabilitation program before TKA. Therefore, the purpose of this study was to evaluate the effect of 3 weeks of preoperative rehabilitation before TKA on postoperative pain.
Methods
Preoperative rehabilitation program applied in this study.
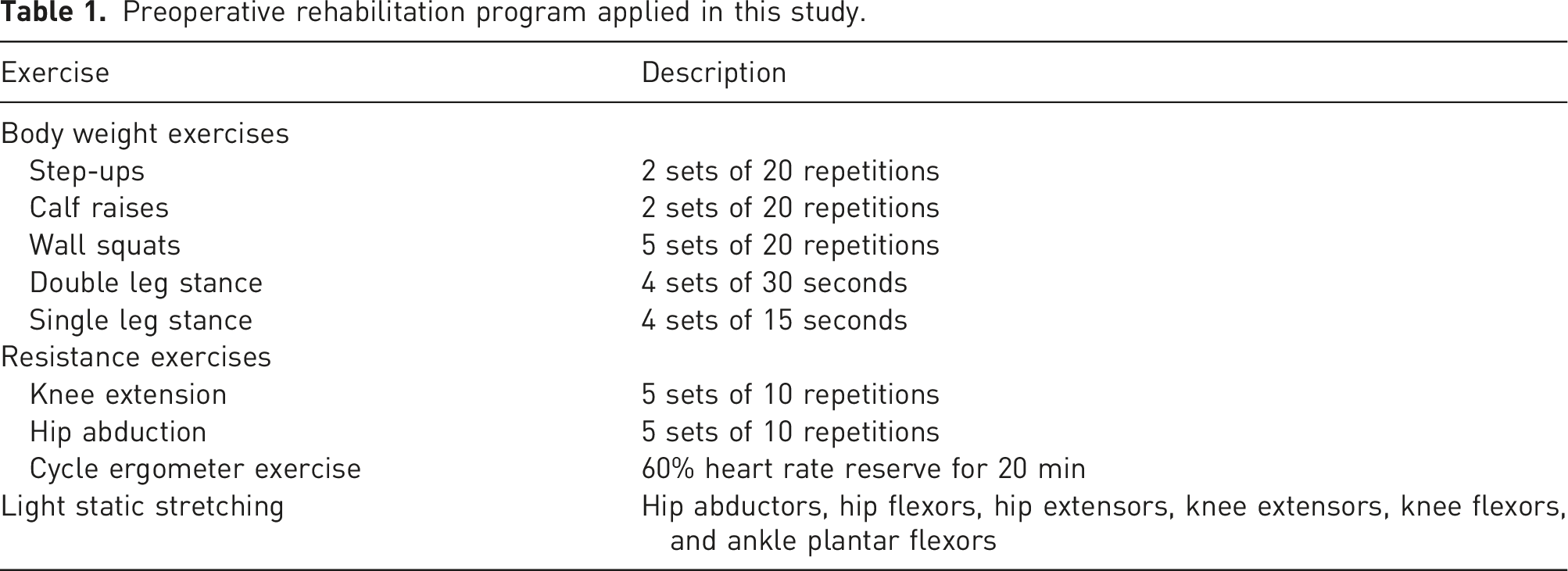
All TKAs were performed using the same surgical technique and were conducted by the same group of experienced orthopedic surgeons at our hospital. In all cases, the posterior cruciate ligament was removed, and surgery was performed using a tourniquet. After TKA surgery, all subjects received the same postoperative rehabilitation protocol at the hospital as part of the usual clinical care. The postoperative rehabilitation protocol was constructed according to the postoperative rehabilitation protocol shown in previous preoperative rehabilitation studies15,20 and the study described in TKA postoperative rehabilitation.
21
The subjects started the rehabilitation program within 24–48 hours after surgery. The subjects were mobilized out of the bed during the first rehabilitation. Mobilization (meaning all out-of-bed activities) was conducted and supervised by a physical therapist. Rehabilitation usually involved resistance exercise, stretching exercises, exercises of daily living, aerobic training, and gait training. This postoperative rehabilitation program was performed daily (Monday to Saturday) twice per day during the hospital stay (3–4 weeks), and each session lasted 1 h. Of the 49 subjects screened (71 knees), 29 subjects (41 knees) were included in the study (insert Figure 1). 20 subjects were excluded: 18 because they declined to participate in this study or informed consent for this study was not obtained. Some of them declined because the measurements such as physical activity were complicated. One subject was hospitalized with other diseases, and one subject withdrew from the study after an accident with bone fracture. Finally, the preoperative rehabilitation group included 14 subjects (20 knees), and the control group included 15 subjects (21 knees). Flow diagram of the progress through the study.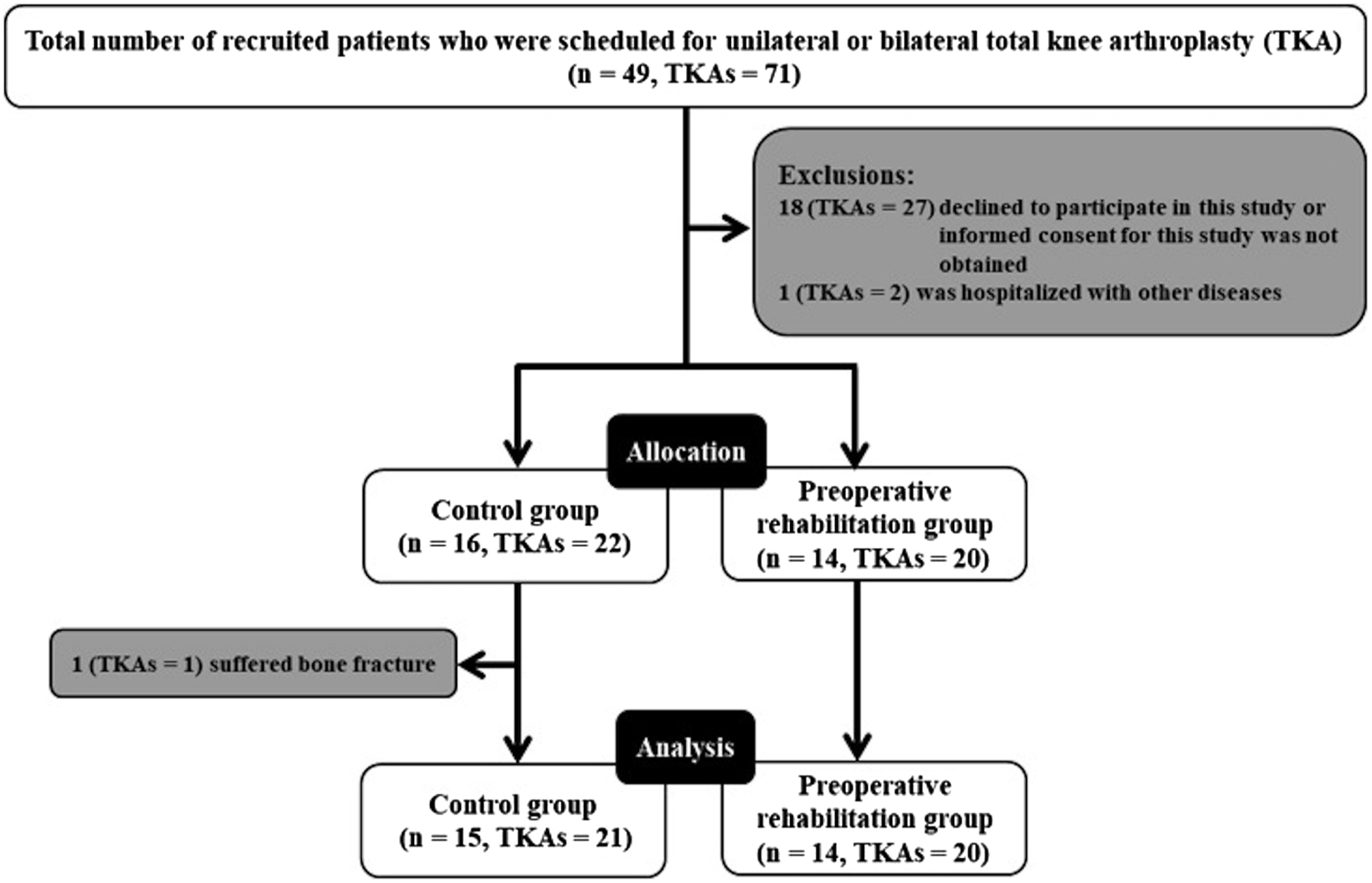
Demographics of the sample population.
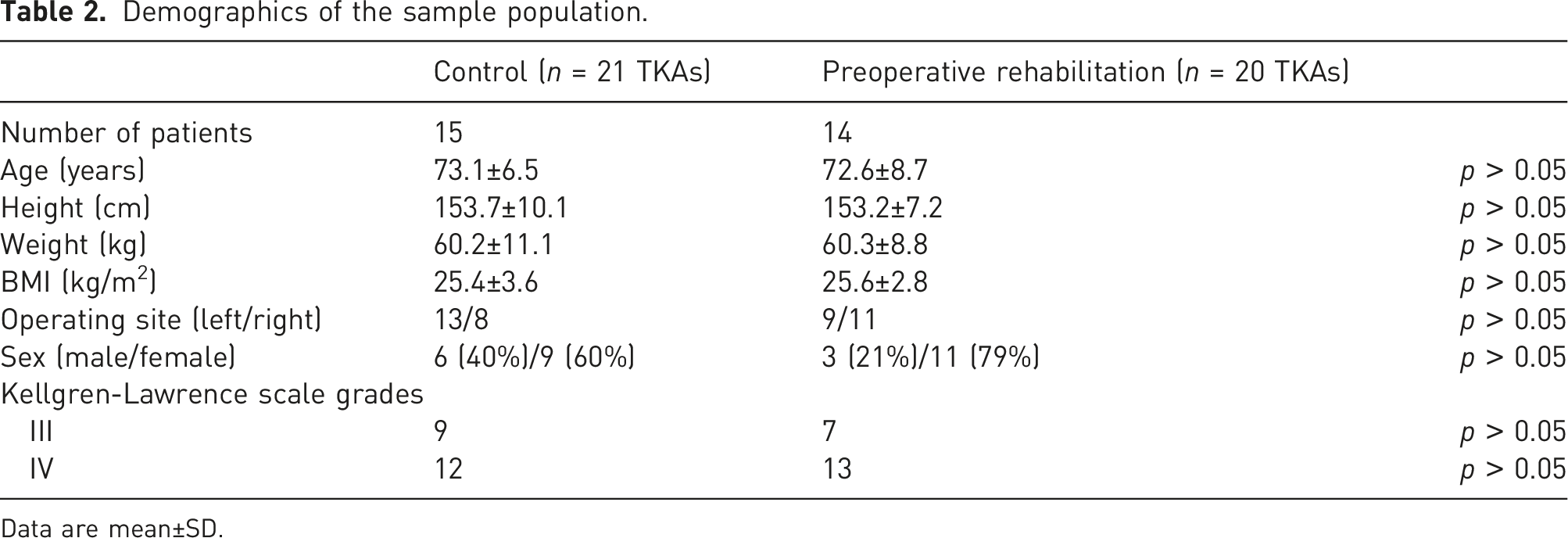
Data are mean±SD.
Scores of all physical measures.
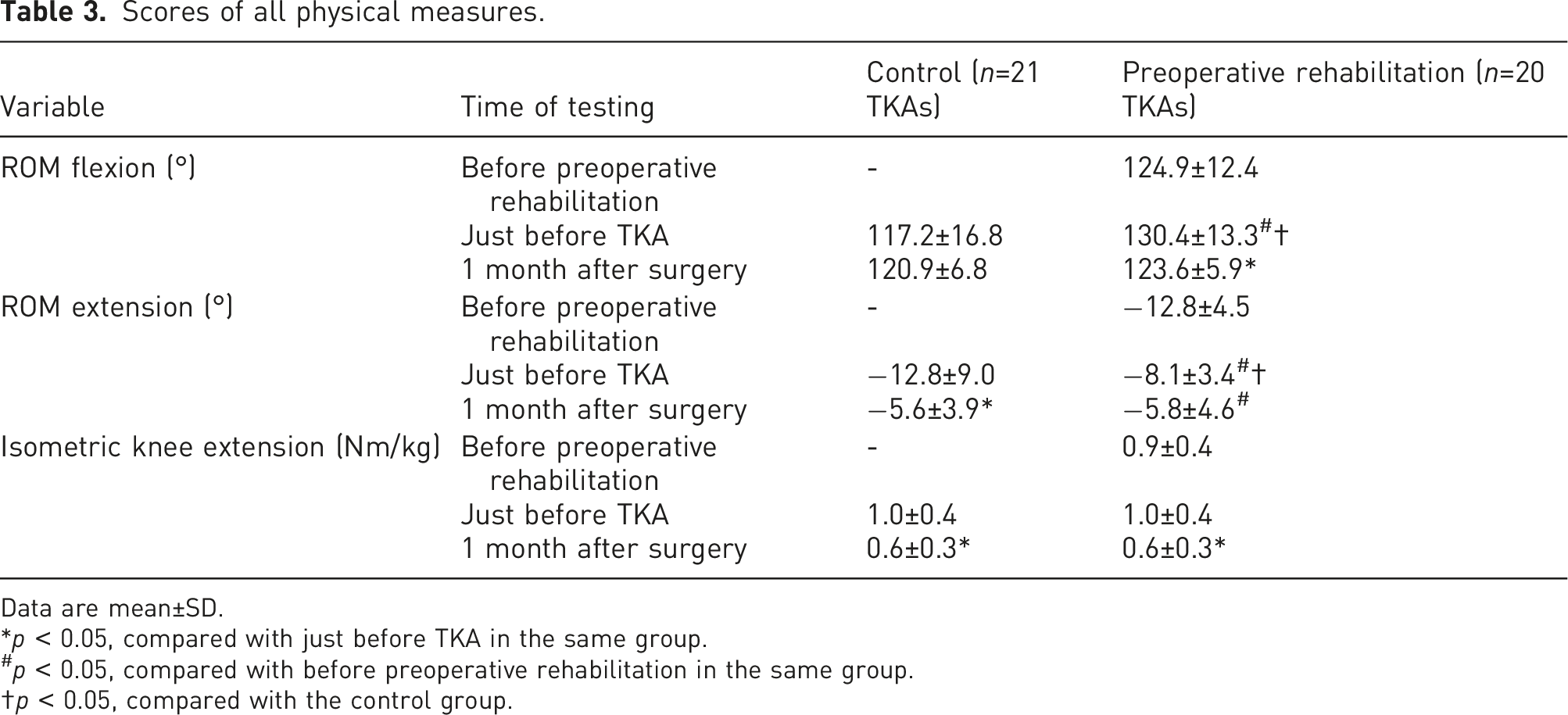
Data are mean±SD.
*p < 0.05, compared with just before TKA in the same group.
#p < 0.05, compared with before preoperative rehabilitation in the same group.
†p < 0.05, compared with the control group.
Scores of all questionnaires.
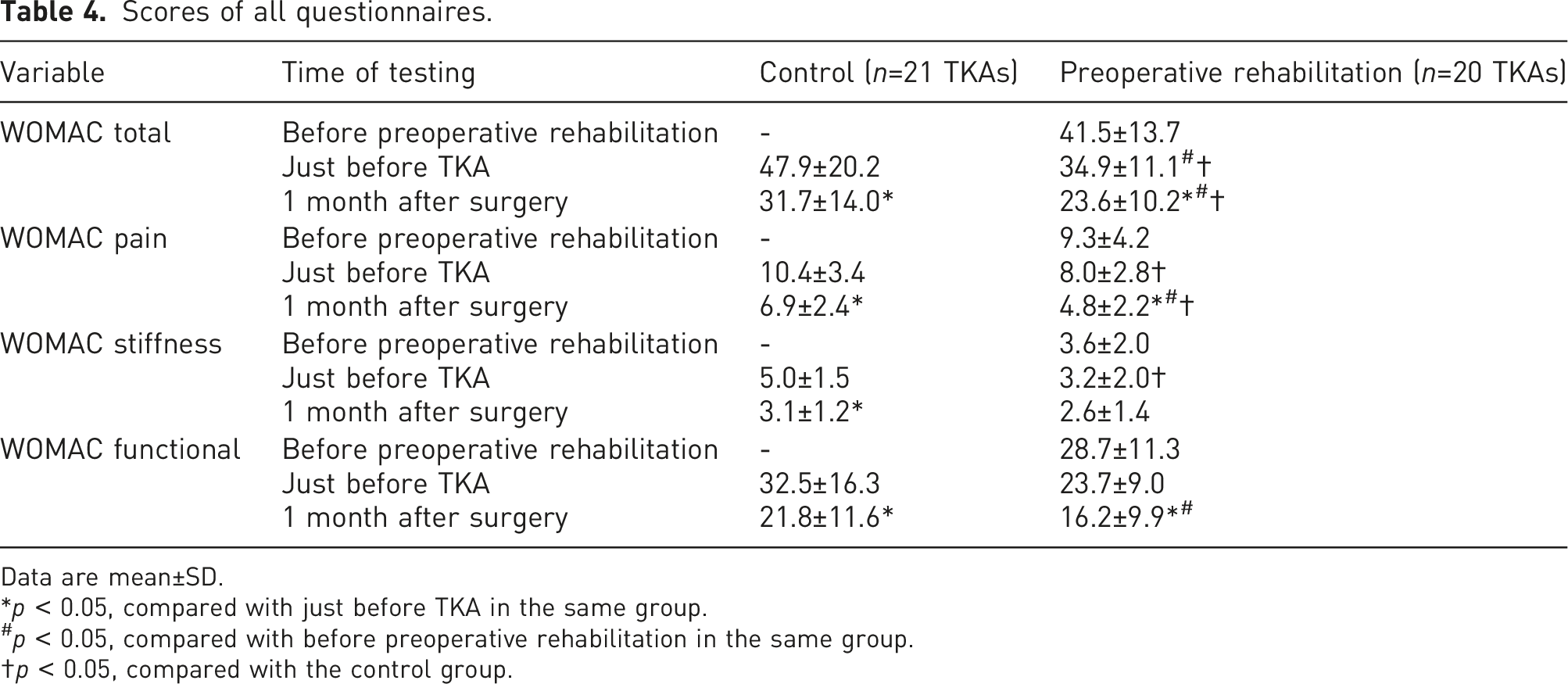
Data are mean±SD.
*p < 0.05, compared with just before TKA in the same group.
#p < 0.05, compared with before preoperative rehabilitation in the same group.
†p < 0.05, compared with the control group.
Scores of all physical activity.

Data are mean±SD.
*p < 0.05, compared with just before TKA in the same group.
Results
The demographics of the subjects are summarized in Table 2.
There were no significant differences between the groups. Passive knee ROM flexion and extension were significantly different before and after 3-weeks of preoperative rehabilitation and just before TKA in the preoperative rehabilitation group (Table 3).
The passive knee ROM just before TKA was significantly better in the preoperative rehabilitation group compared to the control group. The questionnaire data from the WOMAC are displayed in Table 4. The WOMAC total showed significant improvement between the assessments conducted before preoperative rehabilitation and just before TKA in the preoperative rehabilitation group (Table 4). The WOMAC total and WOMAC pain scores just before TKA and 1 month after surgery were significantly lower in the preoperative rehabilitation group than in the control group (Table 4). The effect sizes of WOMAC pain just before TKA and 1 month after surgery were 0.771 and 0.913, respectively. These results seemed to be large by Cohen’s 27 guideline.
Physical activity is displayed in Table 5. The time spent walking, standing, sitting, and lying down for 12 h did not change after TKA in the preoperative rehabilitation group. In contrast, the time the control group spent in walking and standing positions decreased and time in the sitting position increased after TKA (p < 0.05) (Table 5). Physical activity was not significantly different between the two groups.
Discussion
The purpose of this study was to evaluate the association between 3 weeks of preoperative rehabilitation before TKA and postoperative pain following TKA. The two major findings of this study were: 1) WOMAC pain scores before surgery and 1 month after surgery were significantly lower in the preoperative rehabilitation group than in the control group. 2) The post-TKA activity level did not change in patients in the preoperative rehabilitation group, whereas it decreased in the control group. These findings suggest that preoperative rehabilitation reduces postoperative knee pain and does not attenuate daily activities.
WOMAC pain scores before surgery and 1 month after surgery were significantly lower in the preoperative rehabilitation group than in the control group. Previous preoperative studies reported no differences in knee pain reduction between groups20,28–31; however, our 3-week preoperative rehabilitation regimen induced significant reductions in knee pain. While previous studies have shown that knee pain is related to muscle strength,5,32 our findings showed no improvement in isometric strength of the knee extensors. Thus, we assume that muscle strength did not directly contribute to the reduction in knee pain. Previous studies have suggested that exercise suppresses inflammatory response.33,34 Myokine elevation from skeletal muscle after exercise may be related to the attenuation of inflammatory response.34,35 In this study, the rehabilitation program was designed to train the lower limb. Therefore, this rehabilitation program for knee function might be effective in producing myokines from the muscles of the large lower limbs. Accordingly, it is possible that our 3-week preoperative rehabilitation program played a role in the suppression of the inflammatory response. Furthermore, in the preoperative rehabilitation group, knee pain improved both before and 1 month after surgery. Preoperative rehabilitation for 3-weeks might attenuate the inflammatory response before surgery and reduce knee pain 1 month after surgery due to the effects of preoperative rehabilitation and TKA.
The physical activity of patients undergoing TKA can be improved. However, there are no reports on the changes in the physical activity of patients who undergo preoperative exercise training. To our knowledge, this is the first study to analyze the amount of physical activity done by patients who underwent preoperative exercise training. In the preoperative rehabilitation group, the time spent walking, standing, sitting, and lying down did not change after TKA. In the control group, after TKA the time spent walking and standing decreased, and that spent sitting increased. In other words, the activity levels decreased after TKA in the control patients, but not in those who received preoperative rehabilitation. Previous studies have shown that knee pain is related to physical activity.10,11 The study reported the origin of pain is inflammation and the inflammatory response. 36 Previous studies have suggested that exercise suppresses inflammatory response.33,34 In this study, preoperative rehabilitation exercise may have reduced inflammation, which may have reduced pain. On the other hand, pain scores might be significantly lower in the preoperative rehabilitation group than in the control group due to the lack of effect of suppressing inflammation caused by exercise. Our study suggests that the ability to maintain the same physical activity in the preoperative rehabilitation group may be related to reduced knee pain.
The present study demonstrated that 3 weeks of training effectively improved ROM, WOMAC total, and WOMAC functional scores. Previous studies have described the application of a preoperative training period of 4–8 weeks.12-16 In our study, the preoperative rehabilitation group completed the rehabilitation program 3 days per week for 3 weeks before surgery demonstrating the effectiveness of this shorter program in improving various functional parameters. Therefore, it may be effective for patients’ QOL and knee pain to train mainly on the lower limbs for 3 weeks.
Our preoperative rehabilitation program may be beneficial since exercise-based programs are efficacious in reducing knee pain, increasing functional performance, improving QOL, and maintaining physical activity.8,37,38 Previous studies have reported that physical activity is related to the incidence of early loosening. 37 Other studies have concluded that low physical activity was associated with lower muscle strength 11 and that physical activity is a significant factor that protects against poor function. 38 Based on these findings, this preoperative rehabilitation regimen can potentially prevent postoperative complications and maintain long-term function.
Study limitations
The present study has some limitations. First, there was no difference in physical activity between the two groups, although there was a significant difference within each group. Further research is required in this regard. Second, physical activity on the recorded days might not always reflect typical days. Patients participating in a research study on physical activity could change their normal behavior, and the obtained measurements might not always reflect their actual activity. However, all subjects were instructed to wear the monitor for 12 h while awake; accordingly, we believe that this method recorded almost all physical activities. Other factors, such as dosing, may be considered for physical activity. Future studies should assess other factors. In addition, we think it is necessary to carry out highly accurate research such as RCT in the future.
Conclusions
The present study examined the effects of 3 weeks of preoperative training on the lower limbs in patients with severe OA. After preoperative training, knee pain in patients with OA was reduced both before surgery and 1 month after surgery. The post-TKA activity level did not change in patients in the preoperative rehabilitation group, but decreased in the control group. Therefore, this rehabilitation program for knee function might be effective in reducing postoperative knee pain and maintaining physical activity.
Footnotes
Acknowledgments
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclaimers
The views expressed in the articles are that of the authors and not their institutions.