
Abstract
Objectives
To investigate the long-term mortality of acute coronary syndrome (ACS) patients with multivessel disease according to the level of completeness of revascularization (CR) and high-bleeding risk (HBR) status.
Design, Setting, and Participants
This retrospective study collected the data of ACS patients with multivessel disease who underwent percutaneous coronary intervention between May 2018 and February 2019. Complete to reasonable revascularization (CR) was defined by the residual Synergy Between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery score (RSS) of 0 to ≤8. The HBR was defined by the PRECISE-DAPT score ≥25.
Main Outcome Measures
The all-cause death at 36 months according to the CR and HBR status.
Results
A total of 209 patients with 743 lesions were included in the analysis. The median follow-up was 3.6 years. Patients with CR had lower event rates than ICR (4.5 vs. 11.5 per 100 patient-year, HR 0.39, 95% CI 0.22–0.70), p = 0.002). Similar observations were noted when compared between non-HBR and HBR (3.9 vs. 11.1 per 100 patient-year, HR 0.35, 95% CI 0.18–0.64, p < 0.001). Kaplan-Meier analysis revealed that all-cause death was highest among those in the ICR/HBR (40.5%) followed by ICR/non-HBR (28.6%), CR/non-HBR (28.3%) and the lowest among the CR/HBR group (7.1%), log-rank p = <0.001. No significant interaction was observed between the two factors regarding all-cause death (p = 0.10 for interaction).
Conclusions
In ACS patients with MVD, the achievement of CR was associated with reducing mortality rates and consistency irrespective of the HBR status. (Trial Registration: TCTR20211222003)
Introduction
Multivessel coronary artery disease (MVD) in patients with acute coronary syndrome (ACS) is common 1 and associated with unfavorable outcomes. 2 The benefits of complete revascularization (CR) in ACS patients were mainly driven by the reduction of repeat or urgent revascularization.3–6
The residual Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery (SYNTAX) score (RSS) was a method to quantify the complexity of residual stenosis after PCI. 7 The RSS was calculated by subtracting the score of each successfully treated lesion from the baseline SYNTAX score (BSS). Data from the SYNTAX study showed that subjects with RSS 0 to ≤8 after PCI had comparable five-year mortality. 8 However, a clear incremental value of RSS remains controversial in patients presenting with ACS. Some studies supported that RSS had prognostic information in predicting mid- and long-term mortality in ST-elevation myocardial infarction patients with MVD9,10 even with cardiogenic shock. 11
The Complete Revascularization with Multivessel PCI for Myocardial Infarction (COMPLETE) 12 trial demonstrated that CR in non-culprit lesions with a diameter of at least 2.5 mm and diameter stenosis ≥70% had reduced the composite endpoints of cardiac death or non-fatal myocardial infarction (MI) by 26% compared with culprit-lesion-only PCI at the one-year follow-up. 12 The RSS of the CR group and culprit-lesion-only PCI group in the COMPLETE trial were 7.2 ± 4.9 and 7.0 ± 4.7, respectively. Despite the non-significant difference in the RSS between the two groups, patients with CR benefited from a reduction of new, nonfatal MI compared with a culprit-lesion-only group.
Patients with high bleeding risk were associated with the adverse event after revascularization. Ando and colleagues reported that PRECISE-DAPT score (Predicting Bleeding Complications in Patients Undergoing Stent Implantation and Subsequent Dual Antiplatelet Therapy) ≥25 was associated with higher long-term mortality in patients with ACS. 13 In the Functional Assessment in Elderly MI Patients With Multivessel Disease (FIRE) trial, patients who met HBR criteria according to the Academic Research Consortium were at higher risk for the composite of death, MI, stroke, or revascularization at 1 year. 14 Nevertheless, the interaction between the completeness of revascularization and the HBR status on the long-term mortality in ACS patients with MVD remains uncertain. In the present study, we sought to investigate the impact of HBR status on long-term mortality in ACS patients who had MVD and received different levels of completeness of revascularization.
Methods
Study design and population
This single-center retrospective cohort study enrolled ACS patients who had MVD from May 2018 to February 2019 at Maharaj Nakorn Chiang Mai Hospital, Chiang Mai University, Chiang Mai, Thailand. The patients aged more than 18 years old who presented with ACS (ST-elevation myocardial infarction [STEMI] or non-ST-elevation myocardial infarction [NSTEMI]) and received PCI at the culprit lesions within 72 h after the onset were screened in the present study. The diagnosis of ACS was made based on the fourth universal definition of myocardial infarction. 15 Eligible patients were required to be compatible with MVD from angiography, defined as the presence of two or more native major epicardial vessels or their branches by coronary angiogram with visual assessment showing stenosis ≥50% of the diameter. The exclusion criteria were the patients who had terminal disease with a life expectancy of fewer than 12 months, planned surgical revascularization, had significant valvular heart disease indicated for concomitant valve surgery, pregnancy, uncertain culprit lesion from angiography, non-culprit lesion revascularization performed later than 45 days after culprit lesion revascularization, patients with bypass graft surgery, or presence of mechanical complication relating to MI.
Calculation of SYNTAX scores and residual SYNTAX scores
All coronary lesions with a reference vessel diameter (RVD) ≥1.5 mm and diameter stenosis ≥50% by visual estimation were scored using an online calculator (www.syntaxscore.com). The baseline SYNTAX score (BSS) was analyzed by a team of two experienced interventional cardiologists after successful PCI to the culprit lesions (P.S and P.P). The RSS was calculated by subtracting the score of each lesion that was successfully treated from the BSS. We divided the patients into two groups based on complete to reasonable revascularization (CR group: RSS 0 to ≤8) and incomplete revascularization (ICR group: RSS > 8). The ΔSYNTAX score (ΔSS) was defined as the difference between the BSS score and RSS, representing the disease burden removed by PCI. The SYNTAX Revascularization Index (SRI) was calculated using the formula (SRI = (ΔSS/BSS) × 100). 16
Bleeding risk assessment
The individual PRECISE-DAPT scores were calculated using a web calculator (http://www.precisedaptscore.com/predapt/webcalculator.html). Non-high bleeding risk (non-HBR) and HBR patients were defined by the values of the PRECISE-DAPT score of <25 and ≥25, 17 respectively. The duration of the dual antiplatelet therapy was left to the decision of the operators.
Study outcomes
The patients were follow-up until June 2022 for all-cause death. The vital status and/or dates of death of the patients were obtained through the medical records or by telephone interview with the patients or their relatives. Survival time was calculated from the procedural date to the last follow-up or date of death.
Statistical analysis
The continuous variables were expressed as mean ± standard deviation (SD) or median and interquartile range (IQR) when appropriate. The categorical variables were summarized as frequency and percentage. Comparisons between groups were performed using the χ2 test or Fisher's exact test for categorical variables and Student's t-test for continuous variables. Kaplan-Meier curves were used to demonstrate the time-to-event distribution of the primary outcomes between the groups and compared using the log-rank test. The interaction between the revascularization strategy and HBR status on the primary outcomes was assessed. A univariate and multivariate Cox proportional hazards model was analyzed to evaluate the factors associated with long-term mortality. The variables such as age, white blood cell count, hemoglobin level, and creatinine clearance were not tested in the Cox proportional hazard analysis as they were already included in the PRECISE-DAPT scores. To assess the additional values of the combination of RSS and the PRECISE-DAPT scores for predicting long-term mortality, the areas under the receiver operating curve (AUC) were also calculated. A two-sided p-value < 0.05 was considered statistically significant. Statistical analyses were performed using a statistical software package (SPSS ver. 25.0, IBM, Armonk, NY, USA) and STATA version 16.1 software (StataCorp LLC, College Station, TX, USA).
Results
Baseline characteristics
A total of 209 patients who were diagnosed with ACS and multivessel CAD were enrolled in this study. One hundred thirty-seven patients (65.6%) received complete or reasonable revascularization (RSS ≤ 8). Baseline characteristics were presented according to the revascularization and HBR status (Table 1
Characteristics of the patients at baseline.

Data shown in n(%) or median (interquartile 1st–3rd).
Abbreviation: CABG, coronary artery bypass graft; CR, complete revascularisation; HBR, high bleeding risk; ICR, incomplete revascularisation; LVEF, left ventricular ejection fraction; NSTEMI, non-ST elevation myocardial infarction; PCI, percutaneous coronary intervention; OAC oral anticoagulant; PRECISE-DAPT, predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy; RAS, renin-angiotensin-aldosterone system; RSS, residual SYNTAX scores; SRI, SYNTAX revascularization index; STEMI, ST-elevation myocardial infarction; SYNTAX, Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery; svRSS, small vessel residual SYNTAX score; ΔSS, delta SYNTAX score.
The overall mean BSS and RSS were 19.9 ± 9.8 and 7.9 ± 8.1, respectively. Among the study populations, 36 patients (17.2%) had RSS = 0. The SRI was 62.5 ± 29.9. Patients with ICR significantly had higher PRECISE-DAPT scores, BSS, and RSS (Table 1). These similar observations were also noted in the HBR group. Non-HBR patients frequently received ticagrelor more than HBR patients (47.1% vs. 23.3, p < 0.001) (Table 1).
Lesion characteristics
A total of 743 coronary artery lesions were noted from the coronary angiography, 381 lesions (51.3%) were treated with PCI and the remaining 362 lesions (48.7%) were left untreated. The lesion characteristics in each group were summarized in Table 2. Despite the study population being diagnosed with ACS, radial access was used only 11.5%. The proportion of intravascular imaging (IVI)-guided PCI between the CR and ICR groups was not a significant difference (16.8% vs. 13.9%, p = 0.69). Fractional flow reserved guided PCI was only 4.3%. The culprit lesions and non-culprit lesions were treated in 94.3% and 31.9%, respectively. The number of lesions per patient was significantly higher in the ICR group than in the CR group. In addition, the ICR group frequently had triple vessel disease. The culprit lesion of patients in the HBR group frequently showed more complex lesions such as heavy calcification and bifurcation lesion than in the non-HBR group. There were no significant differences in the location of the culprit lesions among the groups (Table S2).
Lesion and procedural characteristics.

Data shows in n(%) or median (interquartile 1st–3rd).
Abbreviation: CABG, coronary artery bypass graft; CR, complete revascularisation; FFR, fractional flow reserve; HBR, high bleeding risk; ICR, incomplete revascularisation; LAD, left anterior descending artery; PCI, percutaneous coronary intervention.
Clinical outcomes
The median follow-up was 3.6 years (IQR 1st–3rd 3.4 to 3.9), 21 patients (15.3%) in the CR group had died, as compared with 25 (34.7%) in the ICR group (hazard ratio [HR], 0.41; 95% confidence interval [CI], 0.23 to 0.73, p = 0.003) (Figure 1(a)). In the HBR status comparison, the incidence of all-cause death was significantly lower among those without HBR than among those with HBR (non-HBR 13.5% vs. HBR 33.3%, HR 0.35; 95% CI, 0.19 to 0.65, p < 0.001) (Figure 1(b)). The percentage of the all-cause death rates was highest among those in the ICR/HBR (40.5%) followed by ICR/non-HBR (28.6%), CR/HBR (28.3%) and the lowest among the CR/HBR group (7.1%) (Figure 1(c)).

Cumulative incidence of the all-cause death stratified by the revascularization strategy and high bleeding risk status. Panels A, B, and C show Kaplan-Meier estimates of the cumulative incidence of all-cause death between patients who received complete revascularisation and incomplete revascularisation, high bleeding risk, and non-high bleeding risk, and according to intervention combination. Abbreviations: CI, confidence interval; CR, complete revascularisation; HBR, high bleeding risk; ICR, incomplete revascularization.
Table 3 summarizes the all-cause death rates per 100 patient-year according to the status of revascularization, HBR status, and both factors. Patients with CR had lower event rates than ICR (4.5 vs. 11.5 per 100 patient-year, HR 0.39, 95% CI 0.22–0.70), p = 0.002). Similar observations were noted when compared between non-HBR and HBR (3.9 vs. 11.1 per 100 patient-year, HR 0.35, 95% CI 0.18–0.64, p < 0.001). When the two factors were combined, patients in the CR/non-HBR groups had significantly lower event rates per 100 patient-year than CR/HBR (2.0 vs. 8.9 per 100 patient-year, HR 0.22, 95% CI 0.08–0.56, p = 0.001). The patients in the ICR/non-HBR group had numerically lower event rates than the ICR/HBR group, however, there was no significant difference in event rates between the group (8.9 vs. 14.4 per 100 patient-year, HR 0.61, 95% CI 0.27–1.37, p = 0.24).
Primary Outcomes.
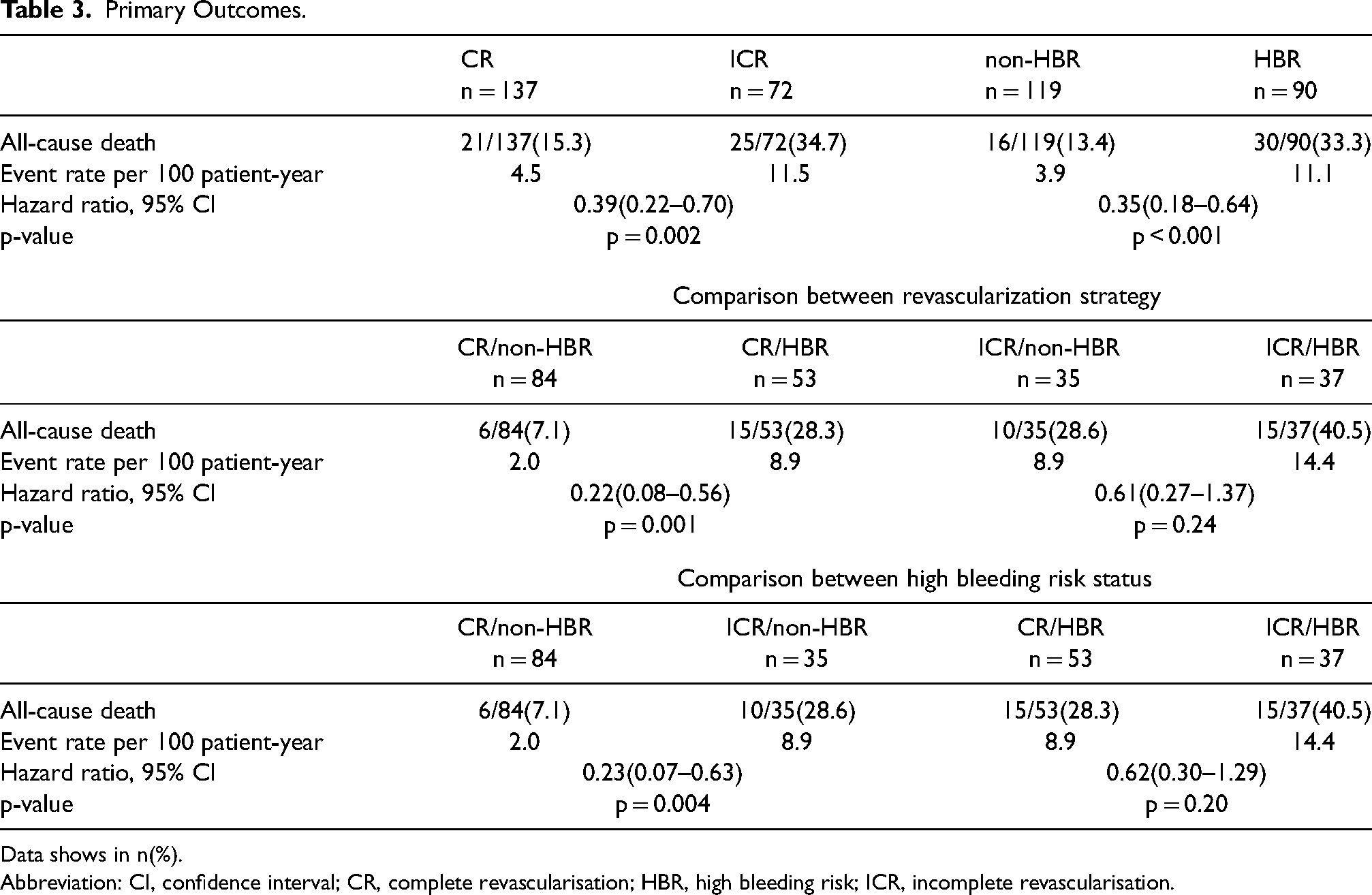
Data shows in n(%).
Abbreviation: CI, confidence interval; CR, complete revascularisation; HBR, high bleeding risk; ICR, incomplete revascularisation.
When comparing the event rate according to the HBR status, there was no statistically significant difference in the event rate among the patients with HBR regardless of CR achieved (CR/HBR 8.9 vs. ICR/HBR 14.4 per 100 patient-year, HR 0.66, 95% CI 0.30–1.29, p = 0.20). By contrast, among the patients without HBR, patients with CR had lower event rates than those with ICR (CR/non-HBR 2.0 vs. ICR/non-HBR 8.9 per 100 patient-year, HR 0.23, 95% CI 0.07–0.63, p = 0.004). The benefits of CR were consistently observed across the various subgroups, without significant interaction P values (Table S3).
After adjusting for covariables, left ventricular ejection function (LVEF) ≤ 40% and RSS ≤8, were associated with all-cause death, and their hazard ratios were 4.09 (95% CI 2.22–7.54) and 2.20 (95% CI 1.03–4.74), respectively. The details of the univariate and multivariate analyses for all-cause death are presented in Table S4.
Predictive performance of PRECISE DAPT score in addition to RSS
The C-index for all-cause death of the RSS and PRECISE-DAPT scores were 0.63 (95% CI 0.53–0.72) and 0.66 (95% CI 0.57–0.75). When these two scores were combined, the C-index slightly improved to 0.71 (95% CI 0.63–0.79). Figure 2 illustrates the difference in the C-index based on the area under the curve (AUC) of RSS, PRECISE DAPT score, and when the two scores were combined.

Receiver operating curves to predict all-cause death in patients with AMI. Abbreviations: PRECISE-DAPT, predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy; RSS, residual syntax score.
Discussion
The study aimed to assess the impact of the CR and the HBR status on long-term mortality in ACS patients with MVD. The main findings in this study are as follows: 1) about two-thirds of ACS patients with MVD could achieve complete or reasonable revascularization; 2) by using PRECISE-DAPT scores, 43.1% of ACS patients with MVD were identified as HBR patients; 3) the achievement of CR was associated with the reduction of mortality rates and consistent irrespective of the HBR status; 4) LVEF ≤40% and the RSS ≥ 8 were the independent predictors of the long-term all-cause death; 5) adding the PRECISE-DAPT scores to the RSS slightly improved the predictive performance of the all-cause death.
In the present study, ACS patients, MVD and HBR were noted in 43.1%, whereas the FIRE 14 trial contained HBR patients for 71%. The difference in the proportion of the HBR in the present study could be from the age of the inclusion criteria and the HBR definition. The present study did not use the Academic Research Consortium for High Bleeding Risk (ARC-HBR) 18 criteria due to the inadequate data to identify the patients at risk such as the history of previous bleeding, malignancy, cirrhosis, non-deferable surgery, and history of arterial vascular malformation. The comparison of performance between the ARC-HBR score and PRECISE-DAPT score in the Korean population showed that the discriminate ability of both scores was not significantly different for predicting all-cause death and bleeding events at one year. 19 However, the discriminating ability of both scores in the long-term remains unknown. Considering that the PRECISE-DAPT scores were easier to use with only five variables required, we used PRECISE-DAPT scores in the present analysis.
Recently, a pre-specified analysis from the FIRE 14 trial investigated the benefit of physiology-guided complete revascularization (either angio- or wire-based FFR) vs. a culprit-only strategy in 1445 patients with HBR, ACS, and MVD. It was reported that physiology-guided CR effectively improves outcomes and decreases complication rates, irrespective of HBR status. The present analysis aligned with the findings of the FIRE trial as no interaction between the CR and HBR status was observed despite using different HBR definitions and revascularization based on coronary angiography.
The proportion of HBR patients who received only culprit lesions in this study was higher than that of non-HBR patients. This could be explained by the age and kidney functions, which were major contributors to the PRECISE-DAPT score. Consequently, operators avoided PCI to the non-culprit lesions in the HBR patients due to concern of contrast-induced nephropathy and frailty. However, Hwang et al. 20 reported that patients with CKD who achieved CR (RSS = 0) had better outcomes than those with CKD but did not achieve CR. Hence, CR should be encouraged for all ACS patients with MVD due to the outstanding benefits in reducing the composite outcomes of death and MI from medium-4,21 to long-term 22 follow-up. To date, complex PCI can be performed with the ultra-low contrast protocol that consumes a contrast volume/estimated glomerular filtration ratio of ≤1:1. Shrivastava and colleagues reported that this protocol was feasible, safe and reduced the incidence of contrast-induced nephropathy. 23 The new generation of interventional cardiologists must learn new techniques and become familiar with IVI-guided PCI to improve the patient outcomes. Adherence to guideline-directed medical treatment is also important, as we found that LVEF ≤ 40% was one of the independent predictors for all-cause death in our population. Titration of the four pillars of heart failure reduced ejection fraction therapy, 24 including an angiotensin-converting enzyme inhibitor (ACEI) or an angiotensin receptor blocker (ARB) or an angiotensin receptor–neprilysin inhibitor (ARNI), a beta-blocker, a mineralocorticoid receptor antagonist (MRA), and a sodium-glucose cotransporter 2 inhibitor (SGLT2i), will certainly improve the long-term clinical outcome.
RSS has been tested to combine with clinical factors in ACS patients to predict all-cause mortality at 5 years. 25 It demonstrated that the high score of the RSS plus clinical factors had a C-statistic of 0.82 for all-cause mortality. 25 PRECISE-DAPT scores were also widely adopted to predict in-hospital outcomes 26 and long-term prognosis. 13 Ando and colleagues reported that the AUC values of PRECISE-DAPT score for all-cause mortality (mean follow-up 1424 days) in patients with acute myocardial infarction was 0.78 (95% CI 0.71–0.85). 13 The AUC of the present study was lower than the earlier reports. It might be explained by the different proportion of STEMI patients that was lower than in the previous publications.
Limitation
There were several mentionable limitations in this study. Firstly, due to the nature of the retrospective study, the completeness of the patient's data was the major limitation, especially, the data on the bleeding events that were not available. Secondly, this is a single-centre study with a small sample size led to an underpower to identify all significant associations. This limited the generalizability of our findings to other populations. Thirdly, PRECISE-DAPT scores were not systematically calculated in all patients, therefore, the DAPT duration was not adjusted to be concordance with patients’ bleeding risk. Fourthly, despite IVI-guided PCI improving the prognosis of the patients, as previously shown in the randomized controlled trial 27 and meta-analysis, 28 the PCI procedure in the present study was mainly angiographic-guided PCI. Only 15% of the patients were treated with IVI-guided PCI. Finally, despite adjusting multiple variables that could potentially be confounders to determine the independent effect of CR, there may be other factors that were not included in the model due to the low event rates.
Conclusion
In ACS patients with MVD, complete revascularization or reasonable revascularization with the target RSS ≤ 8 could reduce long-term mortality. The benefit of CR is consistent, irrespective of the HBR status.
Supplemental Material
sj-docx-1-cvd-10.1177_20480040241283152 - Supplemental material for Impact of the completeness of revascularization and high bleeding risk status in acute coronary syndrome patients with multi-vessel disease: A retrospective analysis
Supplemental material, sj-docx-1-cvd-10.1177_20480040241283152 for Impact of the completeness of revascularization and high bleeding risk status in acute coronary syndrome patients with multi-vessel disease: A retrospective analysis by Tanawat Attachaipanich, Phasakorn Putchagarn, Tasalak Thonghong, Krit Leemasawat, Panupong Pota, Aekapat Phoksiri, Srun Kuanprasert and Pannipa Suwannasom in JRSM Cardiovascular Disease
Footnotes
Acknowledgments
The authors thank their colleagues at the Division of Cardiology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand.
Authors’ contributions
PS contributed to the conception, data interpretation, drafting, and revising of the manuscript. TA, PP, and PS contributed to the conception and drafting of the manuscript. TA, KL, and PS performed the statistical analysis, interpreted the data, drafted, and revised the manuscript. KL, TT, SK, PP, and AP contributed to the data collection, interpretation, and manuscript drafting. All authors approved the publication of the manuscript.
Availability of data and materials
Materials are available on request from the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study protocol was approved by the Research Ethics Committee of the Faculty of Medicine, Chiang Mai University (reference number: REC-25621105-18088) and registered with the Thai Clinical Trials Registry (TCTR), number TCTR20211222003. Informed consent was waived as the data collection was retrospective and without patient identifiers. Study data were collected and managed using REDCap electronic data capture tools hosted at Chiang Mai University.
Funding
This project received a research grant from the Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.