
Abstract
Background:
Patients post-coronary artery bypass graft (CABG) can re-present with acute coronary syndrome (ACS); however, culprit lesion identification, as well as revascularization, is often challenging. Furthermore, the impact of revascularization in this patient group is relatively unknown.
Objectives:
The purpose of our study was to evaluate the efficacy of percutaneous coronary intervention (PCI) in patients with previous CABG surgery presenting with ACS.
Methods:
Using data from the Manitoba Center for Health Policy, we identified patients treated with CABG between April 1979 and March 2018, who subsequently presented with the primary diagnosis of ACS. Patients were divided into four groups: (1) managed medically and not investigated by cardiac catheterization and (2) investigated by cardiac catheterization and treated (2a) medically, (2b) with PCI, and (2c) with redo-CABG. Inverse probability treatment-weighted survival analyses were performed. Ethical approval was obtained from the local research board.
Results:
Nearly 20% of patients treated with CABG presented with ACS at a median of 7.2 years (age at the time of CABG: 66 years (interquartile range: 58–73 years); 75.6% male). Patients treated with PCI (N = 929) demonstrated improved survival compared to the patients investigated by catheterization but treated medically (N = 952; hazard ratio 0.87, 95% confidence interval 0.77–0.97, p = 0.02). Patients who underwent redo CABG (N = 171) experienced 13% mortality within the first year, but subsequently, demonstrated a trend toward improved survival.
Conclusion:
ACS is not uncommon following CABG. Revascularization is associated with prognostic improvement; however, such could be accounted for by inherent group differences, including comorbidities and coronary anatomy These findings should be validated in a prospective randomized study.
Plain language summary
Patients who have had coronary artery bypass graft (CABG) surgery can represent with acute coronary syndrome (ACS). Not only that culprit lesion identification is challenging, but the impact of revascularization remains relatively unknown in this setting. We have reviewed the provincial repository to identify outcomes among patients with previous CABG presenting with ACS and the impact of revascularization.
Introduction
Coronary artery disease is one of the leading causes of morbidity and mortality. Symptomatic patients with obstructive atherosclerotic coronary artery disease are treated with coronary revascularization, either by percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG) surgery. Patients with complex coronary artery disease are commonly treated with CABG. 1 As a result of progressive atherosclerosis, nearly 15% of internal mammary arteries and 40% of saphenous venous grafts (SVGs) become occluded 10 years after CABG surgery. 2 Such patients can present with an acute coronary syndrome (ACS), including unstable angina (UA), ST-elevation myocardial infarction (STEMI), or non-STEMI (NSTEMI).
Multiple studies have demonstrated a mortality benefit for revascularization, either by PCI or CABG, in patients (without previous CABG) presenting with ACS. 3 Identifying a culprit lesion in patients with STEMI is relatively straightforward, whereas such identification in patients presenting with NSTEMI or UA who have had a CABG remains challenging, as they often have complex coronary anatomy. Multiple studies have described worse outcomes after ACS in patients with previous CABG, in comparison to those without prior CABG4–7; however, one reported conflicting findings. 8 The management of ACS post-CABG is confounded by the fact that patients with previous CABG are more likely to have multiple medical comorbidities, an adverse cardiovascular risk profile, and have more complex coronary anatomy often not suitable for revascularization.7,9 The current European and American Cardiology Society guidelines support invasive cardiac catheterization and revascularization as the treatment of choice in patients presenting with ACS10,11; however, this is based on studies that excluded or enrolled only small numbers of patients with previous CABG.12–14 As a result, the precise impact of revascularization in patients with previous CABG, later presenting with ACS remains largely unknown. We aimed to assess the impact of revascularization in this patient cohort, using a provincial population-based administrative dataset.
Materials and methods
Study design
This is a retrospective, population-based, cohort study utilizing linked clinical and administrative databases collected and stored under the Manitoba Centre for Health Policy, a publicly funded, non-profit research unit, based at the University of Manitoba. These datasets contain a unique scrambled identifier allowing for data linkage to occur at the individual level, across multiple provincial government and healthcare agencies databases, including pharmacy, physician billing, and hospital discharge abstract databases. Such an approach has been described previously. 15 Informed consent was waived by the institutional review board and ethics committee.
Data sources
The Hospital Abstracts Database contains information on all hospital discharges in Manitoba, Canada, and includes an International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM), or International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Canada (ICD-10-CA) diagnosis code. This database also contains the ICD-9 Procedure and Canadian Classification of Health Interventions codes, identifying inpatient or day procedures performed at each healthcare facility in Manitoba. The Physician Claims Database contains fee-for-service billings submitted by physicians in the Province of Manitoba, with a catchment area of approximately 1.4 million people. Each submitted billing is also linked to an ICD-9-CM code. The Manitoba Health Insurance Registry contains information on individuals residing in the province of Manitoba, including their birthdate, biological sex, postal code of residence, and the date and reason for termination of their public health insurance coverage, such as death or emigration.
Inclusion criteria
Individuals aged 18 years or older who underwent CABG between April 1, 1979 and March 31, 2018, without a history of prior CABG or PCI, were included in this study. Patients who did not survive their initial hospital stay at the time of CABG were excluded from the analysis. Similarly, individuals investigated by cardiac catheterization following discharge from their initial CABG but before their ACS event were excluded from this analysis, as these individuals might have been treated with revascularization. The Hospital Abstracts Database was used to flag eligible individuals through the use of ICD-9 Procedure Codes and Canadian Classification of Health Interventions codes (Supplemental Table 1).
ACS diagnosis
ACS was defined using ICD-9-CM and ICD-10-CA codes found in the Hospital Abstracts Database (Supplemental Table 2). Primary diagnosis codes of UA and Myocardial Infarction (MI) were flagged for all individuals in the final study cohort who were discharged alive from their initial CABG procedure and experienced the ACS event following their CABG discharge date.
Baseline characteristics
Baseline characteristics were determined using a combination of the data sources mentioned above. These characteristics were assessed for each patient in the study cohort immediately preceding their index CABG procedure, as well as, at the time of their subsequent ACS event. Individual patient household income was extracted by linking the Manitoba Insurance Registry to publicly available household income data from Statistics Canada. This neighborhood-level average income value was then assigned a neighborhood-level income quintile (for urban and rural postal codes, respectively) at the Manitoba Centre for Health Policy. Comorbidities were assessed using the Charlson Comorbidity Index (CHCI)16–19; as well, important cardiovascular risk factors not part of the CHCI, such as hypertension and dyslipidemia status were assessed for the patient population. Physician Claims and the Hospital Abstracts Database were used to flag the relevant ICD-9 and ICD-10 codes for these comorbidities (Supplemental Table 3).
Statistical analysis
Baseline patient characteristics were summarized using medians and interquartile ranges (IQRs) for continuous variables and counts and percentages for categorical variables. The incidence rates of ACS following discharge from the hospital after the initial CABG procedure were estimated via a cumulative incidence curve, with mortality considered as a competing risk. In addition, factors associated with the time to ACS event were evaluated via a cause-specific Cox Proportional Hazards Model, again considering mortality as a competing risk. Fine and Gray’s method was applied to estimate the rates of ACS. 20 The treatment modalities of those who experienced an ACS event following their initial CABG were explored further to examine mortality trends in this patient cohort. Baseline characteristics of patients investigated by cardiac catheterization following their ACS event were compared to those who did not undergo cardiac catheterization using a Mann–Whitney test for continuous variables, and a Chi-square test for categorical variables. For individuals who underwent cardiac catheterization following their ACS diagnosis, the factors associated with survival time were assessed using a Cox-Proportional Hazards Regression Model. This model considered the treatment decision following catheterization (medical management/PCI/CABG) as a time-dependent covariate. Survival rates by treatment decision were visualized using a Kaplan–Meier survival curve. To further evaluate treatment decisions following ACS diagnosis post-CABG in a more contemporary cohort, a subgroup analysis was performed on those who had their ACS diagnosis occur between January 1, 2000 and March 31, 2018. Inverse Probability Treatment Weights (IPTW) were calculated for those who underwent cardiac catheterization followed by medical management and those who underwent cardiac catheterization and subsequent PCI in this cohort of contemporary patients. Unweighted and weighted standardized mean differences were calculated for both cohorts to evaluate the performance of the IPTW. The effect of undergoing PCI following cardiac catheterization on survival time in this cohort was then evaluated by performing an IPTW-adjusted Cox-Proportional Hazards Regression Model, with PCI treatment considered as a time-dependent covariate. In addition, an IPTW-adjusted survival curve was generated to estimate survival rates in these two cohorts of patients. A similar IPTW analysis was conducted to compare survival in the contemporary subgroup of patients who underwent cardiac catheterization and were treated with PCI to those who did not undergo cardiac catheterization.
A final analysis to compare the survival of CABG patients who experienced an ACS (from January 1, 2000 onwards) and were treated with PCI to the general CABG non-ACS population was also performed. A 1:10 propensity score match utilizing a greedy matching algorithm was performed to match one ACS/PCI-treated case to 10 CABG (non-ACS) patients post-discharge. Following this, all cases that had at least two out of 10 matches, and whose follow-up time from their initial CABG discharge was greater than or equal to the number of days from the ACS case’s initial CABG discharge date to their subsequent PCI, were included. For all cases included, two randomly selected controls were considered in the final survival analysis. Follow-up time in this survival analysis was the total follow-up time minus the time from CABG discharge to index PCI. A Kaplan–Meier curve was generated and compared using a log-rank test. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc. Cary, NC, USA).
Results
Between April 1, 1979 and March 31, 2018, 20,297 patients without prior coronary intervention were treated with CABG, forming the eligible CABG population (Figure 1). The baseline characteristics of the patients at the time of index CABG surgery are shown in Supplemental Table 4. The majority (75.6%) of patients were male with a median age of 66 years (IQR 58–73 years); 17.1% of patients had two or fewer grafts, 38.9% had three grafts, and 37.4% had four or more grafts. Of this population, 4102 (20%) patients presented with an ACS at a median of 7.2 years (IQR 3.4–11.5 years) post-CABG (Figures 1 and 2). Of these, 757/4102 (18%) patients with CABG who presented with ACS were excluded from subsequent analysis, as they underwent cardiac catheterization prior to ACS diagnosis (Figure 1). Predictors of ACS in patients with previous CABG included increased age, female sex, lower income, rural residence, previous MI, peripheral vascular disease, peptic ulcer disease, diabetes without complications and dyslipidemia (Supplemental Table 5).

CONSORT diagram describing the study cohort.

Incidence of acute coronary syndrome following coronary artery bypass graft surgery.
Post-CABG ACS patients undergoing cardiac catheterization
Of the patients with previous CABG who presented with an ACS, 2052/3345 (61%) were investigated by cardiac catheterization. Subsequent treatment was medical management (N = 952; 46.4%), PCI (N = 929; 45.3%), or redo CABG (N = 171; 8.3%; Figure 1). Baseline patient demographics for each treatment group investigated with catheterization are displayed in Table 1. Patients treated with redo-CABG were younger (median age 63 years) than those patients treated with PCI (median age 69 years) or medical management (median age 69 years; p < 0.001). Patients treated with PCI had the shortest time to catheterization from ACS diagnosis (median of 2 days), compared to patients who underwent redo-CABG (median of 21 days). Patients treated with medical management alone had more comorbidities, illustrated by a higher weighted CHCI (Table 1).
Characteristics of the study population who underwent cardiac catheterization, stratified based on treatment group.
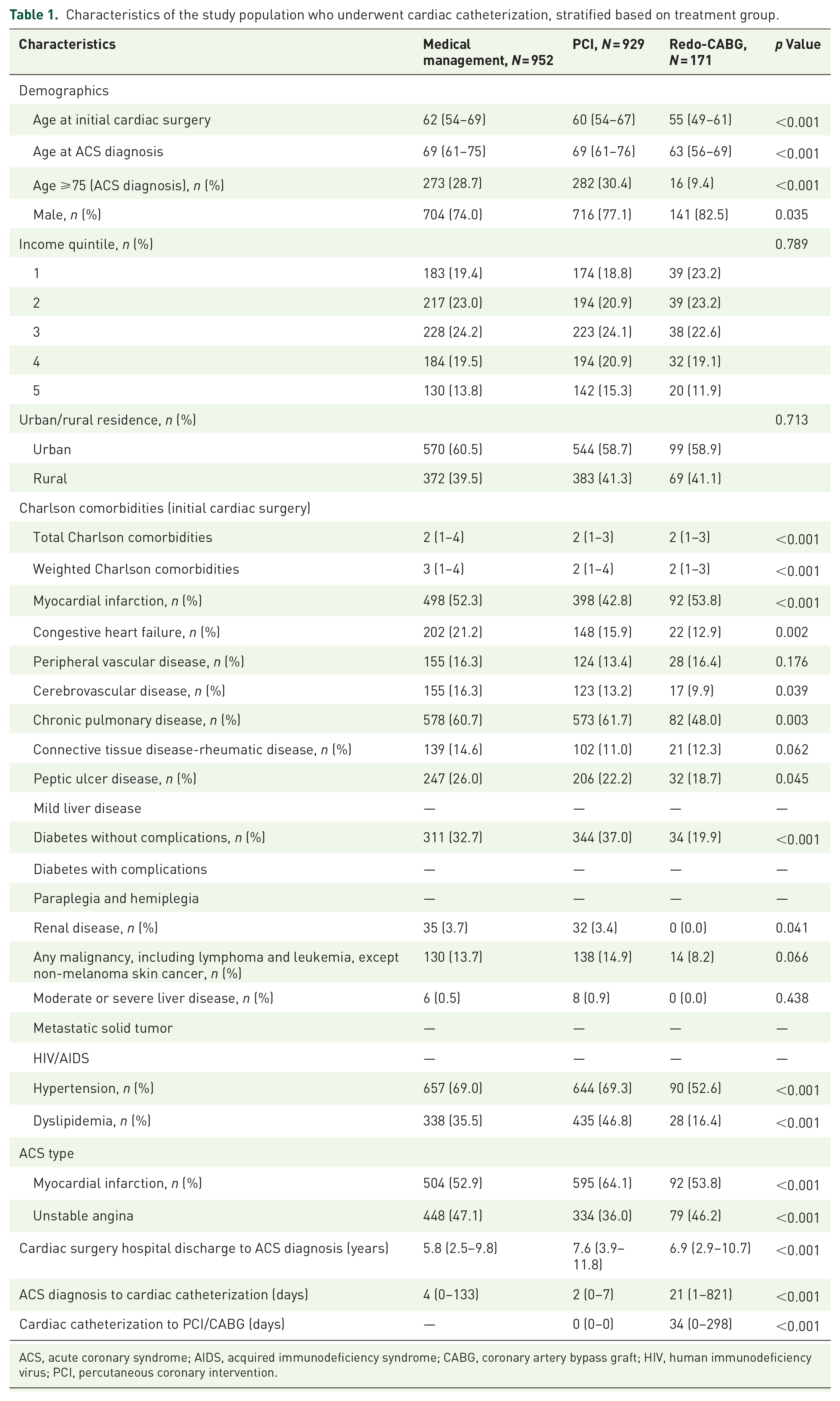
ACS, acute coronary syndrome; AIDS, acquired immunodeficiency syndrome; CABG, coronary artery bypass graft; HIV, human immunodeficiency virus; PCI, percutaneous coronary intervention.
A mortality difference was observed post-cardiac catheterization, which was dependent upon treatment modality (Figure 3). Patients treated with PCI demonstrated improved survival compared to those who underwent catheterization but were treated medically (hazard ratio (HR) 0.87, 95% confidence interval (CI) 0.77–0.97, p = 0.02; Figure 4)). The group treated with redo-CABG demonstrated 13% mortality in the first year; however, for those who survived this initial postoperative period, there was no significant difference in mortality as compared to the medical management group (HR 0.91, 95% CI 0.74–1.11, p = 0.335; Figure 3).

Survival among patients with ACS post-CABG, stratified by treatment post-cardiac catheterization.

Impact of coronary revascularization on survival among the contemporary cohort of patients with ACS post-CABG.
Predictors of mortality for CABG patients following ACS diagnosis included increased age, lower income, congestive heart failure, peripheral vascular disease, diabetes without complications, renal disease, hypertension, dyslipidemia, time from CABG to ACS presentation, and presentation with MI versus UA (Table 2).
Predictors of mortality following ACS in the entire cohort of patients with previous CABG surgery.
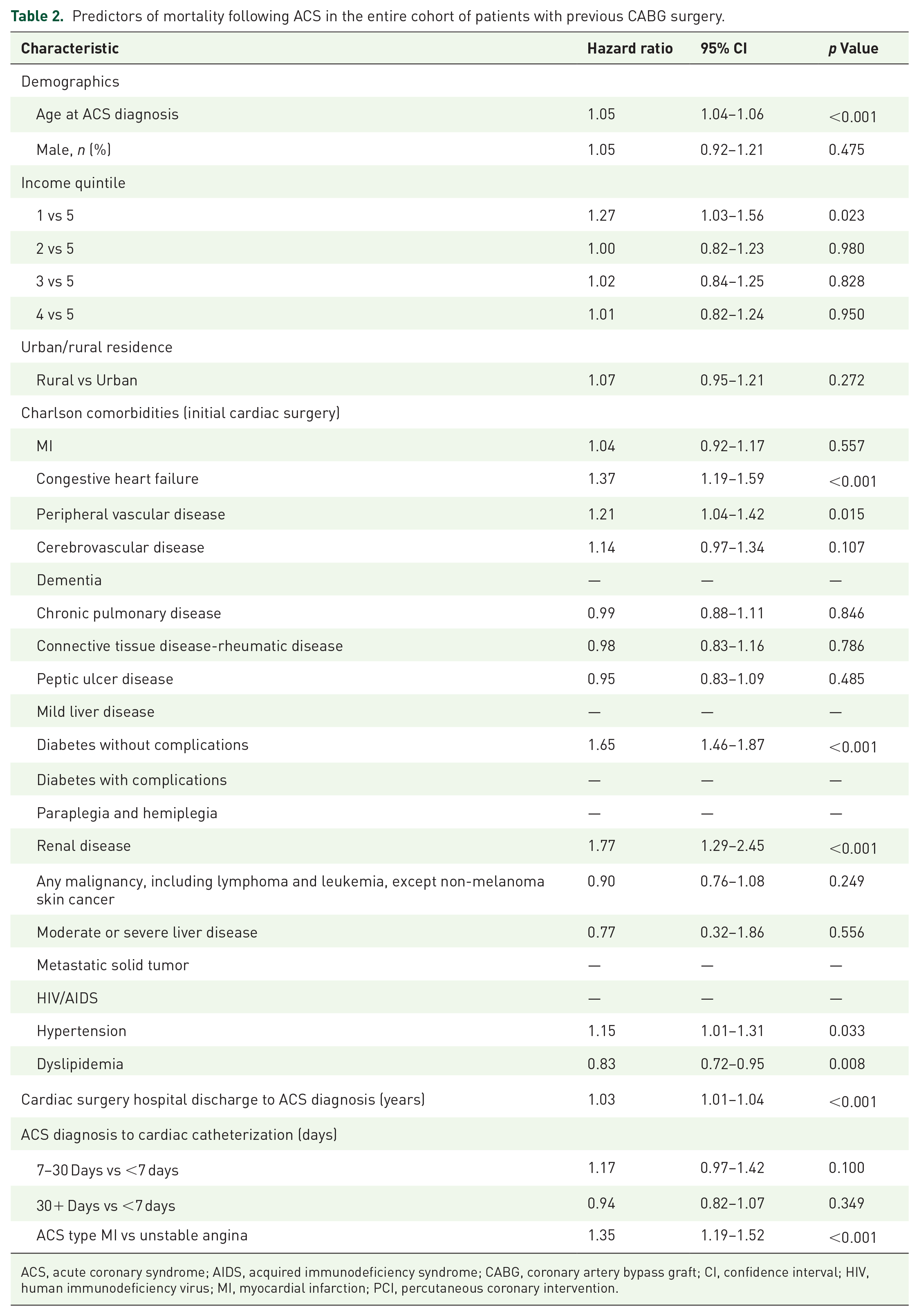
ACS, acute coronary syndrome; AIDS, acquired immunodeficiency syndrome; CABG, coronary artery bypass graft; CI, confidence interval; HIV, human immunodeficiency virus; MI, myocardial infarction; PCI, percutaneous coronary intervention.
Finally, the survival of CABG patients who presented with ACS and were subsequently treated with PCI was compared to a control cohort of CABG patients who never presented with ACS. Baseline characteristics of these two populations are shown in Supplemental Table 6. As depicted in Figure 5, the survival of CABG patients treated with PCI was comparable to those who never presented with ACS after CABG surgery (p = 0.225).
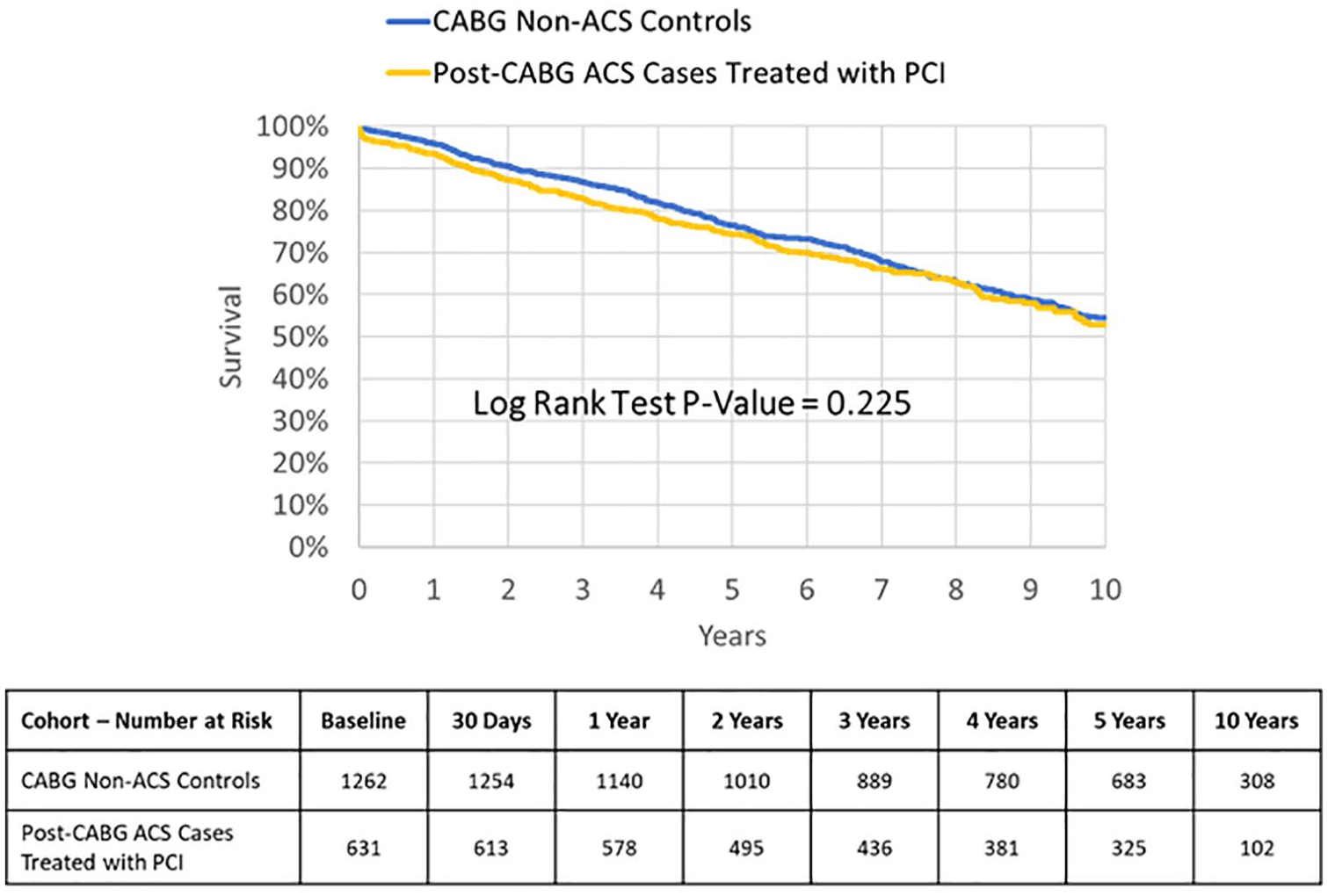
Comparison of survival among patients treated with PCI after their presentation with ACS post-CABG, to the cohort who never experienced ACS post-CABG.
Post-CABG ACS patients not undergoing cardiac catheterization
The group of patients with previous CABG who did not undergo cardiac catheterization on presentation with ACS (N = 1293) were older (median age 75 years, 51.6% age ⩾75 years at ACS diagnosis) than patients investigated with catheterization (median age 68 years, 27.8% age ⩾75 years at ACS diagnosis) (Supplemental Table 7). These patients had a higher likelihood of four or more grafts (p = 0.031) and were more co-comorbid, as suggested by a higher CHCI (Supplemental Table 7). Patients investigated with catheterization and treated with PCI demonstrated improved survival as compared to the patients not investigated with cardiac catheterization, after adjusting for differences in baseline characteristics (HR 0.62, 95% CI 0.56–0.68; p < 0.01); however, after adjustment using a time-dependent definition, statistical significance was not present (HR 0.99, 95% CI 0.90–1.09; p = 0.8) (Supplemental Figure 1).
Discussion
Important findings from our study include the following: (1) nearly one in five patients post-CABG experience an ACS during follow-up, (2) revascularization is associated with improved outcomes in this patient cohort, and (3) in post-CABG patients with ACS treated with PCI, subsequent survival is similar to post-CABG patients who do not re-present with ACS.
Current ACS guidelines recommend investigating patients with previous CABG by cardiac catheterization, followed by revascularization if indicated10,11; however, this is largely based on trials that excluded patients with prior CABG or only included a small number of CABG patients.12–14 Data to guide the specific management of patients with previous CABG who present with ACS are sparse. As this is a unique patient population with increased comorbidities, nonspecific presentations, and complex coronary anatomy, extrapolation of outcome data from the non-CABG population may not be appropriate. 21 Furthermore, reliable culprit lesion identification remains challenging in patients with prior CABG as a result of their typically complex coronary anatomy. 21 The published literature describes a very low rate of revascularization among ACS patients with previous CABG; however, this may increase over time with advancing techniques in complex and chronic total occlusion PCI. 22
Prior studies have reported conflicting outcomes for patients with previous CABG who present with NSTEMI or UA (Table 3). A subgroup analysis, of the Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression Using Integrilin Therapy (PURSUIT) Trial, randomized patients with ACS to eptifibatide or placebo compared patients with prior CABG (N = 1134) to those without (N = 8321). 6 Patients with prior CABG were older, more comorbid, more likely to have a reduced left ventricular ejection fraction, multi-vessel disease, lower thrombolysis in myocardial infarction (TIMI) flow, and more severe culprit stenoses. 6 Adjusted mortality at 30 and 180 days was higher for patients with previous CABG as compared to those without, with HRs of 1.45 and 1.32, respectively. 6 In contrast to these findings, Shoaib et al. compared outcomes between those with and without prior CABG using a registry of 287,658 NSTEMI patients. 22 Patients with prior CABG (N = 25,296) were similarly older and more comorbid. 22 However, all-cause mortality, major bleeding, reinfarction and Major adverse cardiovascular events (MACE) were similar between the two groups after adjustment. 22 In addition, Mathew et al. analyzed 15,936 patients with prior CABG who presented with an acute MI. 8 Patients with prior CABG were less likely to present with ST elevation/left bundle branch block (LBBB) than those without prior CABG. 8 After adjusting for baseline differences, a history of previous CABG was associated with higher in-hospital mortality in those with ST elevation/LBBB (odds ratio (OR), 1.11, 95% CI 1.00–1.23) but not in those with NSTEMI when compared to patients without prior CABG. 8 This discrepancy has been attributed to clinical factors such as increased age and the greater prevalence of comorbidities in the CABG population, as excess mortality is often attenuated with statistical adjustment for such factors. 21
Studies comparing outcomes in patients presenting with ACS, comparing those with previous CABG to those without previous CABG.
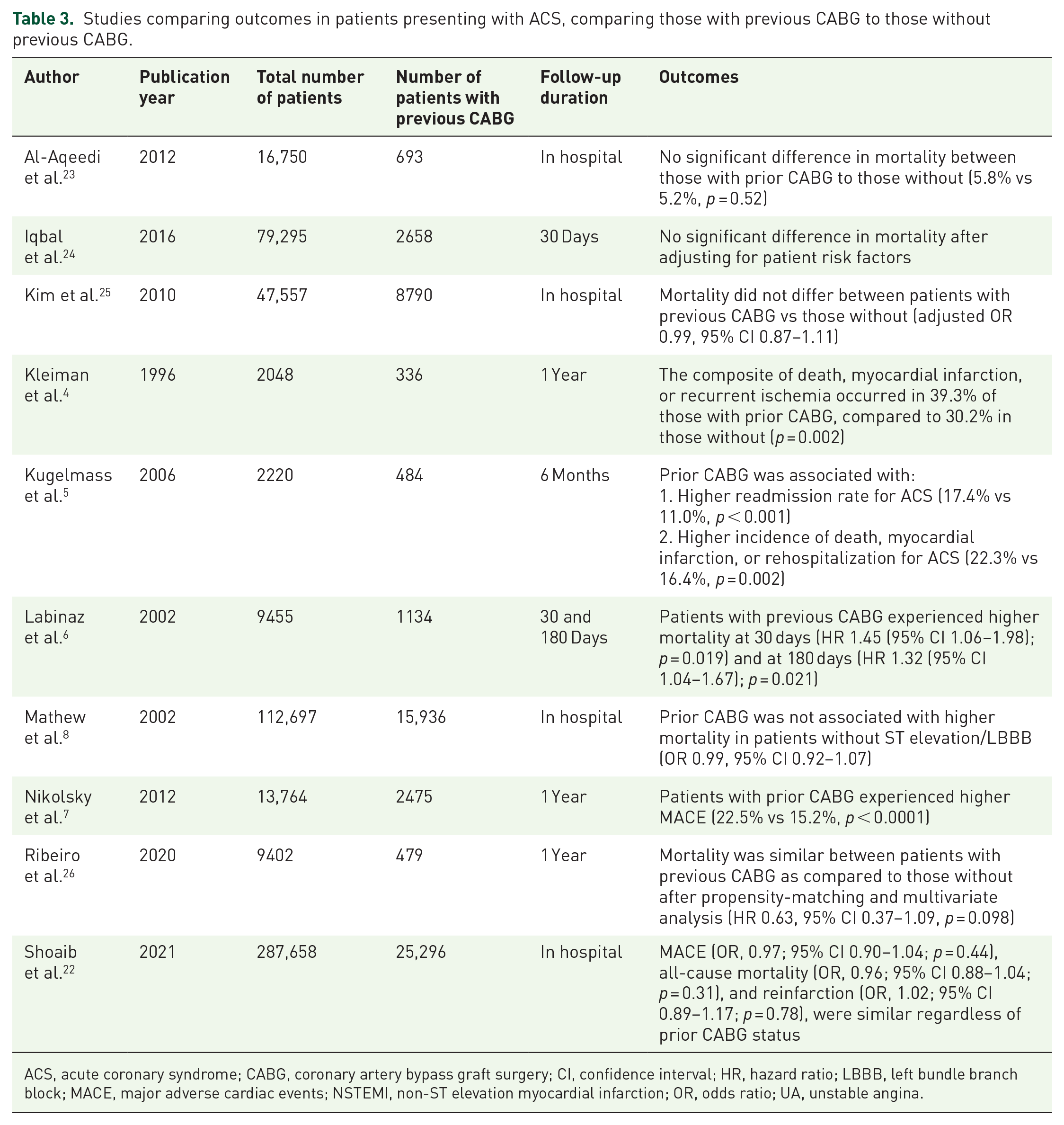
ACS, acute coronary syndrome; CABG, coronary artery bypass graft surgery; CI, confidence interval; HR, hazard ratio; LBBB, left bundle branch block; MACE, major adverse cardiac events; NSTEMI, non-ST elevation myocardial infarction; OR, odds ratio; UA, unstable angina.
An important and often challenging component of revascularization in patients with NSTEMI and previous CABG is to determine the culprit lesion. This may explain, in part, why patients with previous CABG are less likely to undergo revascularization. Shoaib et al. demonstrated that even after adjustment for differences in baseline characteristics, patients with a history of CABG who presented with ACS were less likely to undergo revascularization (40%) as compared to those without previous CABG (53%). 22 Our study corroborates this finding, as only 61% of the post-CABG population were referred for cardiac catheterization. Moreover, when patients with previous CABG are investigated by cardiac catheterization, complex anatomy may preclude revascularization in a proportion of patients. In fact, Lee et al. reported that a culprit vessel was identified in only half of invasively managed CABG patients presenting with NSTEMI. 27 Data from the National Cardiovascular Data Registry (NCDR) cathPCI Registry were used to characterize and determine outcomes in patients with previous CABG, comparing native versus bypass graft PCI. 28 In this large registry of over 1 million interventions, PCI in patients with prior CABG comprised only 17.5% of the total procedural volume. 28 A native coronary artery was believed to be a culprit in the majority of cases (62.5%), whereas a bypass graft culprit comprised only 37.5% of cases (34.9% SVGs, 2.5% arterial grafts, and 0.2% both SVG and arterial grafts). 28 Furthermore, patients with bypass graft PCI had higher contrast volumes and longer fluoroscopy times, lower rates of final TIMI 3 flow, were more likely to require intra-aortic balloon pump support, and experienced higher post-procedural complications and in-hospital mortality, as compared to those with native vessel PCI. 28 Additionally, no reflow, peri-procedural MI, and in-stent restenosis were more common when an SVG was treated, as compared to native vessel PCI. 28
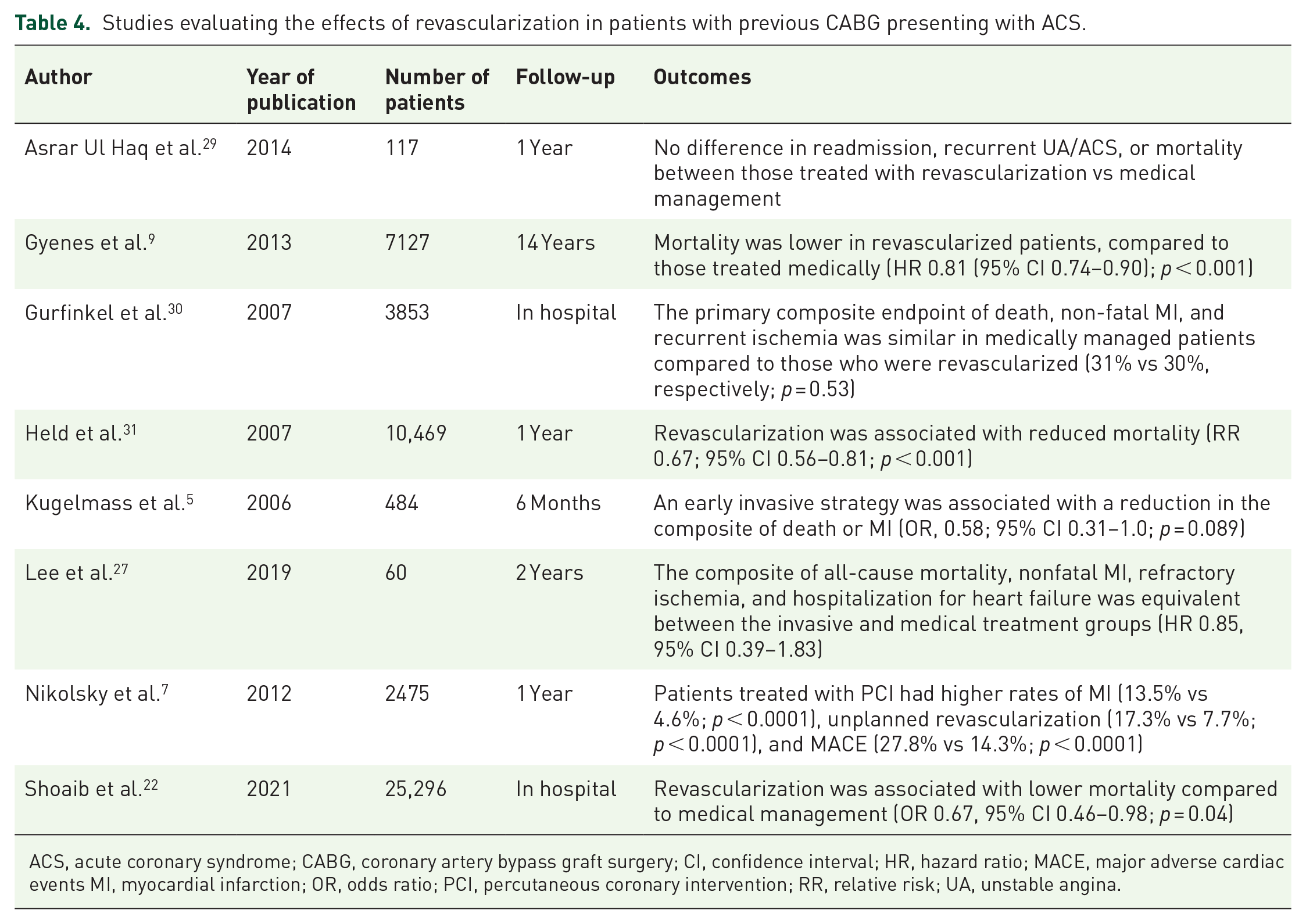
A number of studies have attempted to determine the prognostic benefit of invasive management for NSTEMI in patients with CABG (Table 4). For example, Shoaib et al. conducted a sensitivity analysis on 25,296 patients with previous CABG who presented with NSTEMI, comparing outcomes between those who underwent PCI versus medical management. 22 Those treated medically were older and more likely to have left ventricular dysfunction or chronic kidney disease, similar to our observation. 22 PCI was associated with lower inpatient mortality compared to medical management (OR 0.67, 95% CI 0.46–0.98; p = 0.04); however, the odds of in-hospital reinfarction, major bleeding, and MACE did not differ between the two groups. 22 This result was supported by a subgroup analysis of 484 patients with previous CABG in the TACTICS-TIMI 18 trial, which randomized patients with NSTEMI to an early invasive versus conservative (selectively invasive) strategy. 5 Those with prior CABG demonstrated a higher composite of death, MI, or rehospitalization for ACS compared to those without prior CABG (22.3% vs 16.4%, p = 0.002). 5 In addition, an early invasive strategy in the CABG group trended toward a reduction in death or MI (OR 0.58, 95% CI 0.31–1.0, p = 0.089). 5 Similarly, Gyenes et al. evaluated outcomes in 7127 patients with previous CABG who underwent coronary angiography for ACS or UA. 9 Patients treated with revascularization benefited from improved mortality compared to the medically managed group after adjusting for baseline differences (HR 0.81 (95% CI 0.74–0.90); p < 0.001). 9 These findings contrast a study by Lee et al. which randomized 60 patients with UA or NSTEMI and prior CABG to invasive management or medical care (excluding refractory ischemia or cardiogenic shock). 27 The efficacy outcome including all-cause mortality, nonfatal MI, refractory ischemia, and hospitalization for heart failure was equivalent between the two groups (42% invasive group, 45% medical group; HR 0.85, 95% CI 0.39–1.83). 27 Furthermore, there was no difference in the composite safety outcome of major bleeding, stroke, procedure-related MI, or worsening renal function, which occurred in 26% of the invasive group and 31% of the medical group (HR 0.87, 95% CI 0.34–2.25). 27 Of note, 15/29 (52%) patients assigned to the medical management group underwent catheterization during the follow-up period, of which 7/29 (24%) received PCI, potentially contributing to the negative findings. 27 Our results suggest there may be mortality benefit to revascularization in patients with appropriate anatomy, as compared to those treated medically. In addition, our findings demonstrated survival at par for CABG patients treated with PCI to those with CABG who never re-present with ACS, further suggesting the benefit of revascularization in this setting.
Studies evaluating the effects of revascularization in patients with previous CABG presenting with ACS.
ACS, acute coronary syndrome; CABG, coronary artery bypass graft surgery; CI, confidence interval; HR, hazard ratio; MACE, major adverse cardiac events MI, myocardial infarction; OR, odds ratio; PCI, percutaneous coronary intervention; RR, relative risk; UA, unstable angina.
The exact mechanism driving the apparent survival advantage from revascularization in the post-CABG population remains unknown, and it remains possible that any differences in outcome are reflective of baseline differences in the patient populations. However, the answer may reside in a recent study by Seraphim et al. that evaluated the prognostic implications of global stress myocardial blood flow and perfusion reserve using cardiac magnetic resonance imaging in 341 patients with prior CABG. 32 After adjusting for prognostic factors (age, comorbidities, regional ischemia, extent of previous infarction), both myocardial blood flow and perfusion reserve independently predicted all-cause mortality and MACE. 32 Similar conclusions may be drawn from The Outcomes of Percutaneous RevascularizaTIon for Management of SUrgically Ineligible Patients with Multivessel or Left Main Coronary Artery Disease (OPTIMUM) registry. 33 This study described PCI outcomes in 726 patients with complex coronary artery disease, who were ineligible for CABG. 33 16.4% of patients had a history of prior CABG, and 27.1% presented with an ACS. 33 In this registry, both complete and incomplete revascularization improved symptom and quality of life scores at 6 months, suggesting that any improvement in myocardial blood supply improves patient outcomes. 33 Taken together, these studies imply that the benefit of PCI in cases of ACS following CABG surgery may stem from improved overall myocardial perfusion placing less importance on identifying a specific culprit lesion.
Limitations
The major limitation of our study is the retrospective design, including the lack of individualized patient-level data. Importantly, we were unable to determine why some ACS patients with prior CABG were not referred for cardiac catheterization, a decision made by the treating physician at the time of the ACS presentation. It is possible that this patient cohort may have significant non-cardiac comorbidities, suspected type II MI, known complex coronary anatomy, or other prohibitive risk factors precluding not only invasive assessment but also potentially explaining the higher mortality in this patient group. Given this limitation, this patient cohort was not included in the primary analysis. In addition, those who were referred for catheterization but were ultimately medically managed may have had anatomy that was not suitable for revascularization. What remains unclear is whether the apparent survival benefit in revascularized patients was realized by treating the culprit lesion, by improving overall myocardial perfusion, or was secondary to their fewer medical comorbidities. Finally, despite statistical adjustment for differences within patient groups, unknown confounders may have influenced the observed findings and mortality differences.
Conclusion
Our analysis suggests a prognostic benefit from revascularization in patients with previous CABG presenting with ACS. Although our findings could have been influenced by inherent differences in baseline characteristics, including coronary anatomy and comorbidities, such findings should be validated in a prospective, multicenter study.
Perspectives
Data to guide the management of ACS in patients with a previous CABG are lacking.
We demonstrate a survival advantage for PCI compared to catheterization plus medical management in patients with prior CABG presenting with ACS.
These findings should be validated in future prospective studies.
Supplemental Material
sj-docx-1-tak-10.1177_17539447241308047 – Supplemental material for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization
Supplemental material, sj-docx-1-tak-10.1177_17539447241308047 for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization by Hilary J. Bews, Brett Hiebert, Shuangbo Liu, John Ducas, Amir Ravandi, Kunal Minhas, Malek Kass, Michael P. Love, Harindra C. Wijeysundera and Ashish H. Shah in Therapeutic Advances in Cardiovascular Disease
Supplemental Material
sj-docx-2-tak-10.1177_17539447241308047 – Supplemental material for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization
Supplemental material, sj-docx-2-tak-10.1177_17539447241308047 for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization by Hilary J. Bews, Brett Hiebert, Shuangbo Liu, John Ducas, Amir Ravandi, Kunal Minhas, Malek Kass, Michael P. Love, Harindra C. Wijeysundera and Ashish H. Shah in Therapeutic Advances in Cardiovascular Disease
Supplemental Material
sj-docx-3-tak-10.1177_17539447241308047 – Supplemental material for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization
Supplemental material, sj-docx-3-tak-10.1177_17539447241308047 for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization by Hilary J. Bews, Brett Hiebert, Shuangbo Liu, John Ducas, Amir Ravandi, Kunal Minhas, Malek Kass, Michael P. Love, Harindra C. Wijeysundera and Ashish H. Shah in Therapeutic Advances in Cardiovascular Disease
Supplemental Material
sj-docx-4-tak-10.1177_17539447241308047 – Supplemental material for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization
Supplemental material, sj-docx-4-tak-10.1177_17539447241308047 for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization by Hilary J. Bews, Brett Hiebert, Shuangbo Liu, John Ducas, Amir Ravandi, Kunal Minhas, Malek Kass, Michael P. Love, Harindra C. Wijeysundera and Ashish H. Shah in Therapeutic Advances in Cardiovascular Disease
Supplemental Material
sj-docx-5-tak-10.1177_17539447241308047 – Supplemental material for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization
Supplemental material, sj-docx-5-tak-10.1177_17539447241308047 for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization by Hilary J. Bews, Brett Hiebert, Shuangbo Liu, John Ducas, Amir Ravandi, Kunal Minhas, Malek Kass, Michael P. Love, Harindra C. Wijeysundera and Ashish H. Shah in Therapeutic Advances in Cardiovascular Disease
Supplemental Material
sj-docx-6-tak-10.1177_17539447241308047 – Supplemental material for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization
Supplemental material, sj-docx-6-tak-10.1177_17539447241308047 for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization by Hilary J. Bews, Brett Hiebert, Shuangbo Liu, John Ducas, Amir Ravandi, Kunal Minhas, Malek Kass, Michael P. Love, Harindra C. Wijeysundera and Ashish H. Shah in Therapeutic Advances in Cardiovascular Disease
Supplemental Material
sj-docx-7-tak-10.1177_17539447241308047 – Supplemental material for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization
Supplemental material, sj-docx-7-tak-10.1177_17539447241308047 for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization by Hilary J. Bews, Brett Hiebert, Shuangbo Liu, John Ducas, Amir Ravandi, Kunal Minhas, Malek Kass, Michael P. Love, Harindra C. Wijeysundera and Ashish H. Shah in Therapeutic Advances in Cardiovascular Disease
Supplemental Material
sj-jpg-8-tak-10.1177_17539447241308047 – Supplemental material for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization
Supplemental material, sj-jpg-8-tak-10.1177_17539447241308047 for Outcomes among patients with coronary artery bypass grafts presenting with acute coronary syndrome: impact of revascularization by Hilary J. Bews, Brett Hiebert, Shuangbo Liu, John Ducas, Amir Ravandi, Kunal Minhas, Malek Kass, Michael P. Love, Harindra C. Wijeysundera and Ashish H. Shah in Therapeutic Advances in Cardiovascular Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.