
Abstract
Objective
There is limited information about the extent of metabolic syndrome (MetS) among subjects with cardiac diseases in Ethiopia. Therefore, this study aimed to determine the prevalence and associated factors of MetS among adults with cardiac diseases.
Methods
A cross-sectional study was conducted at Hawassa University Comprehensive Specialized Hospital in southern-Ethiopia between May 2021 and August 2021. Data pertaining to the study were collected from 319 participants (153 cardiac and 166 non-cardiac groups) using the WHO stepwise approach. The International Diabetes Federation (IDF) and the revised National Cholesterol Education Program: Adult Treatment Panel III (ATP) were used to define MetS.
Results
The prevalence of MetS was 44.2% and 50.2% in IDF and ATP III, respectively. Among the cardiac group, 54.9% had MetS in IDF criteria, compared to 34.3% in the non-cardiac group (p < .001); whereas, it was 60.1% in the cardiac group and 41% in non-cardiac group (p < .001) by ATP III. Age >60 years, waist–height ratio ≥5, high waist–hip ratio, body mass index 25–29.9 and ≥30 kg/m2 were significantly associated with higher odds of MetS in both IDF and ATP III. Also, smoking history and monthly income were associated with MetS by ATP III, while being female was associated with higher odds of MetS by IDF.
Conclusion
More than half of the subjects with cardiac diseases developed MetS as compared to non-cardiac controls. Periodic screening and focusing on the identified modifiable high-risk factors such as body weight, smoking, and central adiposity is important to effectively mitigate the risk of further comorbidity and complications in this high-risk population.
Introduction
Metabolic syndrome (MetS) is a combination of conditions like obesity, high blood pressure, high blood sugar levels, abnormal cholesterol levels, and insulin resistance. These factors together raise the chances of developing severe health problems such as cardiovascular disease, diabetes, and stroke. 1
MetS is strongly linked to an increased risk of diabetes and cardiovascular diseases (CVDs).1,2 Considering that CVDs are the main reason for illness and death worldwide, and it is crucial to analyze how MetS helps to reduce the burden of this CVDs.1,3 In general, the risk of all-cause death increased by 1.5 times and the risk of CVD mortality, and stroke increased by two times in individuals with MetS. Therefore, those with the MetS were more prone to cardiovascular consequences rather than all-cause mortality. 4
Individuals diagnosed with MetS face approximately two to three times higher risk of developing CVD and die when compared to those who do not have the condition.5,6 Patients suffering from CVD could be vigilant about their susceptibility to acquiring additional illnesses, considering the severe and often fatal complications associated with the disease. Among these potential comorbidities, MetS stands out as particularly impactful, as it can exacerbate the effects of CVD and raise the likelihood of its incidence.5,7
Insulin resistance, persistent inflammation, and activation of neurohormones have been proposed as key factors in the progression of MetS and the subsequent transition to CVDs and type 2 diabetes.1,4 In addition, several factors, including endothelial damage, LDL-cholesterol accumulation, and monocyte activation in smooth muscle cells within the arterial wall, are thought to contribute the development and advancement of atherosclerosis. The components of MetS are also believed to be involved in atherogenesis, either through direct or indirect mechanisms, due to their strong linkage to CVD. 8
A review of data from 29 African nations found a prevalence of MetS in the African population to be 32.4%. 9 In Ethiopia, the prevalence was almost similar, with a rate of 30.0% and a confidence interval (CI) ranging from 24.0% to 36.0%. 10 However, a study conducted abroad revealed that the prevalence of MetS among patients with cardiovascular diseases was 34.2%, with a 95% CI ranging from 26.8% to 42.6%. 5
MetS is indeed a significant health concern globally, particularly in regions like sub-Saharan Africa, including Ethiopia, where there is a growing burden of both infectious and non-communicable diseases (NCDs). MetS acts as a precursor and significant risk factor for various cardiovascular conditions, including coronary artery disease, stroke, and heart failure. 11 In addition, the clustering of metabolic abnormalities within MetS significantly increases the risk of developing CVD and exacerbates its progression. 11 Understanding of prevalence and the association of MetS with CVD is crucial for effective prevention and management strategies. Therefore, the present study aimed to determine the prevalence and associated factors of MetS among adults with cardiac diseases using two definitions.
Materials and methods
Study setting, design, and population
This was comparative cross-sectional study in design and conducted between May 2021 and August 2021 at the chronic diseases clinic of Hawassa University Comprehensive Specialized Hospital. Hawassa, the capital city of the Sidama region, is located 275 km away from Addis Ababa to the south direction. The study involved two groups of participants: the first group consisted of subjects with diagnosed cardiac diseases who were included in the cardiac disease group, while the second group included those without cardiac diseases as a control group. All participants were at least 18 years old during the study period. However, pregnant women, patients with known diabetes, patients with renal failures and chronic liver disease, and confirmed HIV patients were excluded from the study.
Sample size, participants’ recruitment, and sampling technique
The sample size estimation was conducted by taking into account the difference between proportions and considering the following parameters: alpha (α) = 5%, beta (β) = 10%, and power = 90%. In relation to MetS, the prevalence of 34.2% was considered for subjects with cardiac diseases,
5
while a prevalence of 16.7% was considered for a group of subjects without cardiac diseases.
12

Data collection and assessments
The structured questionnaire was developed by adapting the World Health Organization (WHO) STEPwise questionnaire 13 to collect data from the study subjects via interviewer administration such as socio-demographic, behavioral, anthropometric, and clinical information. Before actual data collection, the purpose, benefits, and procedure were clarified to each study participant. Next to this, trained nurses who were working in the chronic diseases clinic did the measurements of blood pressure, height, weight, waist circumferences and hip circumferences of the study subjects. In addition, a review of medical records of the patients was done to include the required information. Anthropometric measurements were taken using a Seca weighing scale and stadiometer to measure weight (in kilograms) and height (in centimeters), respectively. Participants were instructed to wear light clothing and be barefoot, with measurements rounded to the nearest 100 g for weight and 0.5 cm for height. Body mass index (BMI) was calculated by dividing weight by height squared (kg/m2), with results categorized as underweight (BMI <18.5), normal weight (BMI 18.5–24.9), overweight (BMI 25–29.9), and obese (BMI ≥30). Waist circumference (WC) was assessed by measuring the distance between the iliac crest and the lower rib to the nearest 0.1 cm. The hip circumference (HC) was measured at the widest point of the buttocks with a precision of 0.1 cm. To determine the waist-to-hip ratio (WHR) and waist-to-height ratio (WHtR), the WC (cm) was divided by the HC (cm); and WC (cm) was divided by the height (cm), respectively. Blood pressure (BP) was measured using a standard adult digital blood pressure device. The measurement was conducted after the patients had rested and stabilized for a minimum of 5 min in the clinic. To ensure accuracy, two readings were taken within a 2-min interval, and the average of these readings was used to determine the BP status of the participants.
Sample collection and laboratory analysis
Each subject provided approximately 4–5 ml of vein blood, which was collected using a gel-based serum separator tube (gel-SST) after an overnight fast of 8–12 hours. Within 30 min of collection, the serum was separated and analyzed for biochemical biomarkers determination or stored at −52 °C in case there was a delay in laboratory analysis. To determine serum triglycerides (TGs) and fasting blood sugar (FBS), an enzymatic colorimetric technique was utilized. In addition, a direct homogeneous method was conducted to measure the HDL-cholesterol (HDL-c) level. These serum biochemical biomarkers were quantified by the COBAS 6000 analyzer from Roche, Germany.
Definition of metabolic syndrome
As per the definition of revised National Cholesterol Education Adult Treatment Panel III (NCEP-ATP) guideline of 2005, MetS is defined as having at least three of the following five risk factors: a WC of ≥102 cm for males and ≥88 cm for females, BP of ≥130/85 mmHg or on medication, FBS of ≥ 100 mg/dl, TG ≥ of 150 mg/dl or on medication, and HDL-c of < 40 mg/dl for men and < 50 mg/dl for women or on medication. 14 according to International Diabetes Federation (IDF) definition, it is defined as the presence of central obesity (adjusted for Africans) ≥80 cm in women and ≥94 cm in men plus any two of the other four criteria which are mainly the same to those stated in the revised NCEP-ATP III criteria above. 15
Data management and quality control
The English version questionnaire was initially prepared and then translated into the local Amharic language for data collection purposes. To ensure its effectiveness, the questionnaire was tested on 18 confirmed subjects with cardiac diseases in another hospital. Any necessary correction was made based on the pre-test feedback. Data collectors received training on how to collect socio-demographic, behavioral, and anthropometric data, as well as on research ethics. The principal investigator diligently checked the clarity of all collected data on a daily basis. Furthermore, all laboratory data collection and test analyses were strictly adhered to standard operational procedures (SOPs).
Data analysis
All questionnaires underwent visual inspection, coding, and entry into the Statistical Package for Social Sciences (SPSS) Version 27 for statistical analysis. Descriptive statistics were employed to characterize the study population in relation to relevant variables. The chi-square test was utilized for categorical variables. In addition, the mean and differences of quantitative continuous data in the study groups were assessed using student's t-test. The distribution of categorical variables in the study groups was examined through bivariable and multivariable binary logistic regression. Moreover, a p-value <.25 was employed as a threshold for including a variable in the multivariable analysis. Finally, results were deemed statistically significant when the p-value was <.05 at a 95% CI.
Results
Socio-demographic and socio-economic characteristics of the study participants
A total of 319 participants were enrolled in the study, consisting of 164 males (51.4%) and 155 females (48.6%). The participants were divided into two groups: the first group consisted of 153 subjects with cardiac diseases, with 64 males (41.8%) and 89 females (58.2%), who were following and had been receiving care during the study period. The second group consisted of 166 subjects without cardiac diseases, with 100 males (60.2%) and 66 females (39.8%), who visited the medical outpatient departments for their medical conditions (controls). The median age of the study participants was 42 years (IQR: 27–60), and the subjects with cardiac diseases were older than those without, with a median age of 55 years (IQR: 39.5–65) versus 35 years (IQR: 25–45), respectively (p < .001). In terms of marital status, 78.1% of the participants were married, 29.8% were housewives, and 58.9% were urban inhabitants (Table 1).
Socio-demographic characteristics of the study participants.
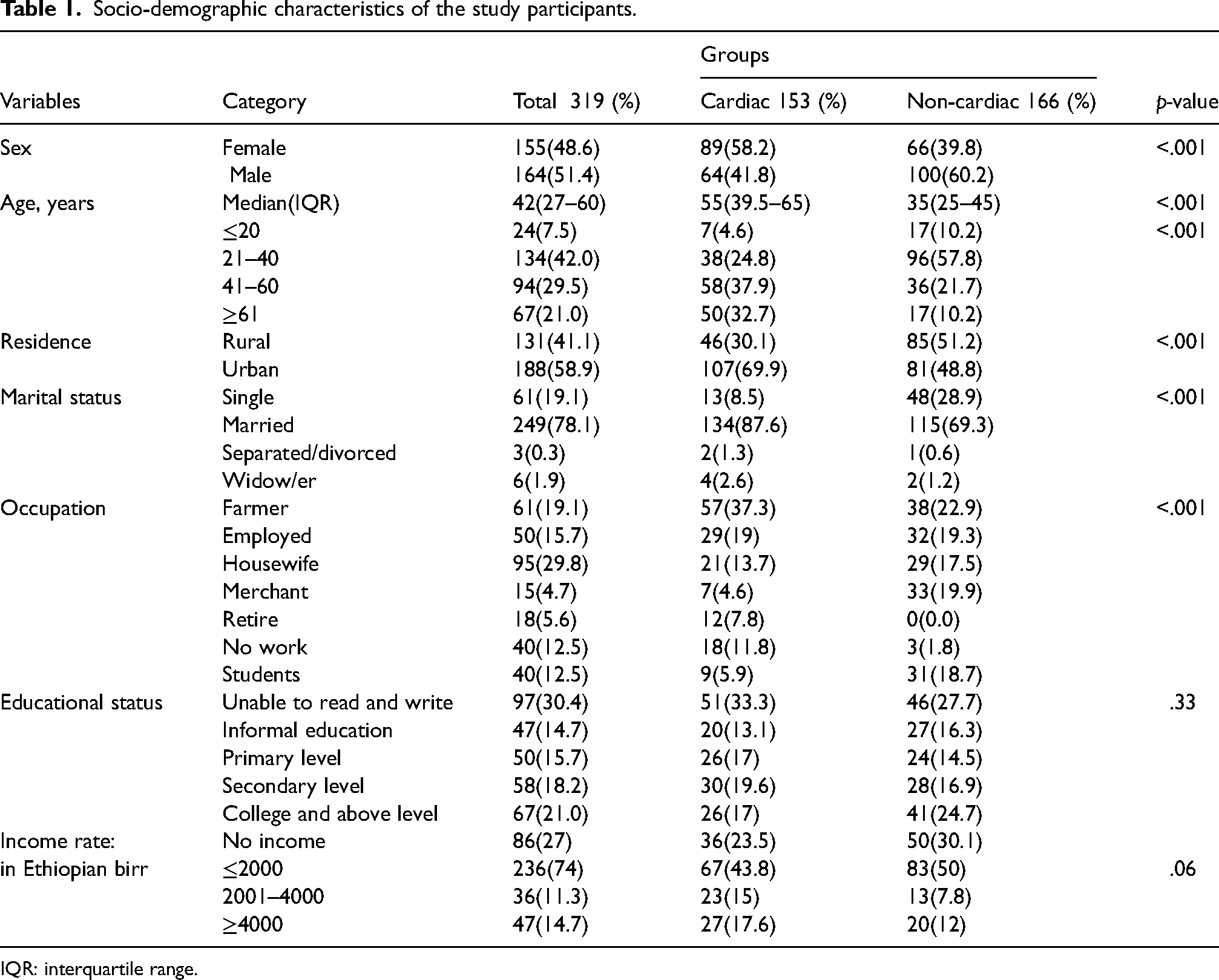
IQR: interquartile range.
Anthropometric, behavioral, and other characteristics of the study participants
More than three-fourths (76.1%) of the study participants had a sedentary to light physical activity performance. About 6.3% had a family history of cardiac problems. Majorities (80.3%) and more than half (51.1%) of the participants had been using fruits and vegetables for a maximum of 2 days/week, respectively. Additionally, a number of participants reported various health issues, such as depression (15.4%), a history of smoking (7.5%), a history of alcoholism (11.9%), and the use of combination drugs for cardiac problems (31%). The average BMI was 23 (±5.2) kg/m2, with cardiac cases having a significantly higher BMI (24.4 ± 5.8 kg/m2) compared to non-cardiac controls (21.6 ± 4.1 kg/m2), p < .001 (Table 2).
Anthropometric, behavioral, and clinical characteristics of the study participants.

BMI: body mass index; kg: kilogram; m: meter; SD: standard deviation; NA: not applicable; * Fisher's exact test.
Patterns of cardiac diseases among participants with cardiac diseases
Out of the 153 patients with cardiac conditions, 25.5% had ischemic heart disease (IHD), 13.7% had hypertensive heart disease (HHD), 3.3% had congestive heart failure (CHF), and 19% had dilated cardiomyopathy (DCM). Additionally, 5.9% had Cor pulmonale, 18.3% had rheumatic heart diseases (RHDs), 2.6% had degenerative vulvar heart disease, and 11.8% had other types of heart disease.
Prevalence of metabolic syndrome and its components among the study participants
In both IDF and NCEP-ATP III definitions, the frequency of abnormal MetS components within a single individual was higher among subjects with cardiac diseases when compared to those without cardiac diseases. The rate of four and five MetS component abnormality was higher among women compared to men in both definitions (Figure 1).

Frequency of abnormal components of metabolic syndrome within a single individual by criteria and cardiac category.
Participants with and without cardiac disease were not significantly different with regard to the mean values of HC (98 ± 13.1 vs. 95.5 ± 12.5 cm, p = .089), FBS (105.3 ± 32.3 vs. 100.9 ± 20.8 mg/dl, p = .14), and WHR (0.95 ± 0.09 vs. 0.95 ± 0.14, 0.89). In addition, WHtR, HDL-c, and TGs also did not show significant variation between the study groups (p > .05). However, the mean WC, SBP, and DBP were significantly higher among subjects with cardiac diseases compared to subjects without cardiac diseases, p < .001, p < .001, and p = .027, respectively. The overall prevalence of MetS was 44.2% (95% CI: 38.6–49.5) using the IDF criteria, while 50.2% (95% CI: 44.5–55.5) using the revised NCEP-ATP III criteria. The cardiac group had a significantly higher rate of MetS when compared to the non-cardiac group in both criteria (54.9% vs. 34.3%, p < .001 by IDF; and 60.1% vs. 41%, p < .001 by NCEP-ATP, respectively). In addition, the rate of MetS was higher in women when compared to men (56.1% vs. 32.9%; p < .001), respectively using IDF while it was higher in women (55.5%) compared to men (45.1%) but the difference was not significant, p = .06. In IDF criteria, the prevalence of abdominal obesity, raised FBS, raised TGs, low HDL-c, and raised BP were 58.9%, 45.1%, 31.3%, 84.6%, and 44.2%, respectively. Moreover, the prevalence of abdominal obesity and raised BP were significantly higher in cardiac group compared to non-cardiac group (68.6% vs. 50%; p < .001 by IDF; and 45.8% vs. 29.5%; p < .001 by NCEP-ATP) and (60.8% vs. 28.9%, p < .001), respectively (Table 3).
Pattern of metabolic syndrome and its components among the study participants.
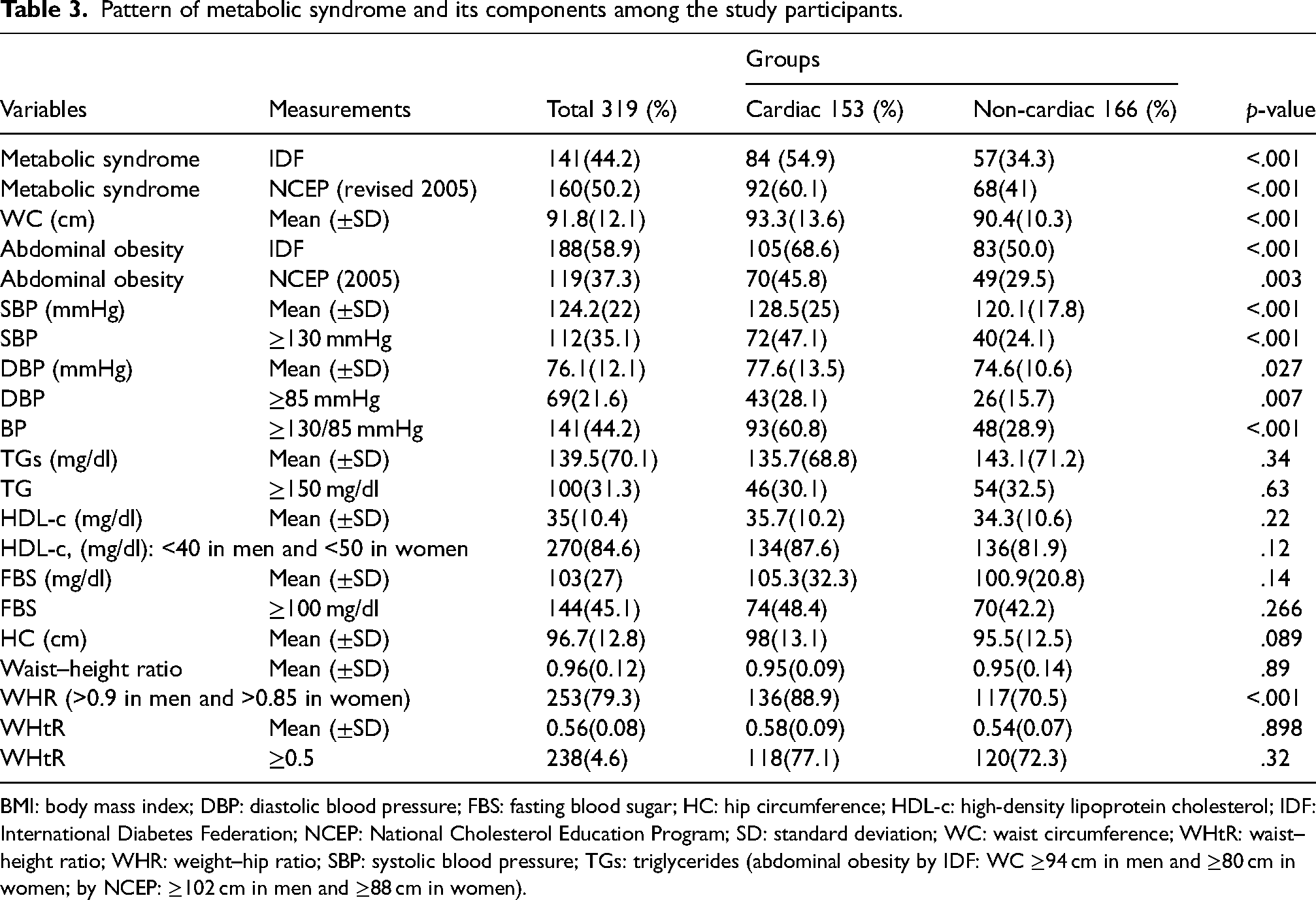
BMI: body mass index; DBP: diastolic blood pressure; FBS: fasting blood sugar; HC: hip circumference; HDL-c: high-density lipoprotein cholesterol; IDF: International Diabetes Federation; NCEP: National Cholesterol Education Program; SD: standard deviation; WC: waist circumference; WHtR: waist–height ratio; WHR: weight–hip ratio; SBP: systolic blood pressure; TGs: triglycerides (abdominal obesity by IDF: WC ≥94 cm in men and ≥80 cm in women; by NCEP: ≥102 cm in men and ≥88 cm in women).
Factors associated with the prevalence of metabolic syndrome
The study conducted crude and adjusted estimates to identify the independent factors associated with the prevalence of MetS among the study subjects. The crude odds ratio (COR) and adjusted odds ratio (AOR) at 95% CI were used for this purpose. In the multivariate analysis, several factors including age, monthly income, WHtR, WHR, and BMI were found to be significant risk factors for MetS according to the revised NCEP-ATP III criteria. Participants with a monthly income of ≤2000 Ethiopian birr had a 44% lower chance of developing MetS [AOR (95% CI): 0.44 (0.23–0.0.85)]. Age over 60 years, being overweight (≥25–29.9 kg/m2), and obesity (≥30 kg/m2) were identified as predictors for MetS [AOR (95% CI): 4.6(1.1–19.3)], [AOR (95% CI):2.9 (1.4–6.0)], and [AOR (95% CI):4.1 (1.5–11.6)], respectively. Additionally, WHtR of ≥5, WHR, and a history of smoking were also significant risk factors for MetS [AOR (95% CI): 3.3(1.7–6.5)], [AOR (95% CI): 2.2(1.1–4.7)], and [AOR (95% CI): 2.9(1.1–8.8)], respectively. However, there was no significant association found between sex and MetS based on the NCEP-ATP III criteria (Table 4).
Factors associated with metabolic syndrome in the study subjects by NCEP-ATP III.

AOR: adjusted odds ratio; BMI: body mass index; COR: crude odds ratio; FHCD: family history of cardiac disease; MetS: metabolic; WHtR: waist–height ratio; WHR: weight–hip ratio (high WHR: >0.9 in men and >0.85 in women).
On the other hand, when conducting a multivariate analysis, it was revealed that female sex, age, WHtR, WHR, and BMI were all significant risk factors for MetS according to the IDF criteria. Specifically, being female, being over 60 years old, having a BMI between 25–29.9 kg/m2, and having a BMI of ≥30 kg/m2 were identified as individual predictors for MetS. The AORs and their corresponding 95% CI were as follows: 2.2 (1.1–4.3) for being female, 10.7 (1.8–64.2) for age >60 years, 4.1 (1.7–10) for overweight and 12.2 (4.2–35.8) for obesity. Additionally, a WHtR ≥ 5 and abnormal WHR were determined to be significant risk factors for MetS [AOR (95% CI): 16.1(5.7–44.9)] and [AOR (95% CI):12.2(4.2–35.8)], respectively. With regard to monthly income level, there was no statistically significant association with MetS based on IDF criteria (Table 5).
Factors associated with metabolic syndrome among the study subjects by IDF.

AOR: adjusted odds ratio; BMI: body mass index; COR: crude odds ratio; FHCD: family history of cardiac disease; WHtR: waist–height ratio; WHR: weight–hip ratio (high WHR: >0.9 in men and >0.8 in women).
Discussion
MetS comprises a cluster of severe cardiovascular risk factors such as diabetes, dyslipidemia, abdominal obesity, and elevated blood pressure. Therefore, the objective of the present study was to assess the occurrence of MetS and its associated risk factors among patients with cardiac problems in a resource-constrained East African environment.
The prevalence of MetS using the IDF was 44.2% (95% CI: 38.6–49.5), while it was 50.2% (95% CI: 44.5–55.5) when using the revised NCEP-ATP criteria. These results are higher than the prevalence reported among apparently healthy working adults of Addis Ababa (12.5% using ATP criteria and 17.9% using IDF criteria), 16 a community-based study in Gondar, northwest Ethiopia (11.2% using ATP III and 11.9% using IDF), 17 working adults in Eastern Ethiopia (20.1% by IDF), 18 and the pooled prevalence report of MetS in a systematic review and meta-analysis of the Ethiopian population (34.89% by ATP and 27.92% by IDF). 19 The observed difference may be due to the higher proportion of older participants (>40 years = 50.5%), the inclusion of subjects with cardiac diseases, and care seeker controls in the present study.
In this study, the prevalence of MetS in subjects with cardiac diseases was 60.1% (95% CI: 52.3–67.3) according to the revised NCEP-ATP criteria. Interestingly, a similar prevalence rate of 54% was found in a study conducted in Ghana using the same criteria. 20 However, other international studies reported lower rates of MetS: 49.5% in Iran among patients with coronary artery disease, 21 42.5% in the Netherlands in heart failure cases, 22 40.8% in Spain among patients with coronary heart disease, 23 33.4% in China in patients with ischemic diseases, 24 and 37.1% in India in patients with acute coronary syndrome. 25 It is important to note that most of these studies focused on patients with a single type of cardiac problem, whereas our study included patients with different cardiac diseases. This difference in patient selection may contribute to the variation in prevalence rates observed across the studies. In addition, we found that the prevalence of MetS in subjects with cardiac diseases according to IDF criteria was 54.9% (95% CI: 47.1–62.7). This finding is almost consistent with the result of a study conducted in China among patients with coronary heart disease, which reported a prevalence of 47.2%. 24 However, our finding was lower than the rate of 68.3% reported in a study conducted in Vietnam among patients with acute myocardial infarction (AMI). 26 On the other hand, our finding was higher than the result of a systematic review and meta-analysis of 27 studies conducted in Iran, which reported a prevalence of 34.2% in patients with various cardiovascular diseases. 5 These differences may be attributed to variations in the criteria used to define MetS, consideration of the specific type of cardiac problem group as study participants, the sample sizes included in the studies, and genetic disparities between populations.
In relation to the occurrence of MetS components, abdominal obesity was found to be 58.9% according to IDF, which is somewhat similar to the study conducted in Ghana, 54% 20 but lower than the reported rates from India 24 and Iran, 21 which were 87.4% and 75.8% by ATP, respectively.
Additionally, our study revealed that the most frequently observed component of MetS, HDL-c, accounted for 84.6% of the cases. This finding is consistent with a study conducted in Iran, which reported a similar prevalence of 84.8%. 21 However, our study found a higher prevalence compared to the study conducted in Indonesia, where the prevalence was 69.1% among patients with coronary heart disease. 27 Moreover, we found the rate of raised FBS, raised TGs, and raised BP were 45.1%, 31.3%, and 44.2%, respectively. These findings were relatively lower than those reported in studies conducted in India 25 and Ghana. 20 The variations in these rates could be attributed to genetic disparities, differences in dietary habits among individuals, the progression of the cardiac disease in patients, and the lifestyle of the individuals.
In this study, the prevalence of MetS was found to be significantly higher in women (27.3%) compared to men (16.9%) using IDF criteria. This finding is consistent with a study conducted in Shandong, China. 24 The increased risk of MetS among women may be attributed to factors such as higher levels of adipose tissue, the influence of oral contraceptive use, and the onset of menopause. 28 Also, our study revealed that individuals over the age of 60 years had a significantly higher risk of developing MetS according to both criteria. Similar findings have been reported in other studies, highlighting the association between older age and MetS.20,29,30 This association could be attributed to the impact of aging on oxidative stress, insulin resistance, adiposity, and hormonal changes, all of which contribute to the development of metabolic syndrome.31,32 However, the findings are inconsistent with those reported from India 25 and America, 26 which indicated that younger individuals are at a higher risk of developing MetS due to factors such as smoking and alcohol consumption at a younger age.
In this study, participants who exhibited high WHtR, WHR, and BMI ≥25 kg/m2 were found to have a significant association with the development of MetS according to both ATP and IDF criteria. This finding is corroborated by a study conducted in Ghana, 20 Iran, 21 and Vietnam USA, 26 which highlights central obesity as a crucial factor in the onset of MetS. The association between increased BMI, central obesity, visceral fat accumulation, inflammation, insulin resistance, and the risk of MetS and CVDs is well established in the literature. 26 Moreover, in this study, 41.8% of participants with cardiac problems had a BMI ≥25 kg/m2, 68.6% had high WC according to IDF criteria, and 45% based on NCEP-ATP guidelines. This suggests a potential increase in excess body fat, even without metabolic problems, highlighting a population at risk. 33 Obesity continues to be a significant public health issue, with a strong link to an increased risk of developing new-onset heart failure. 34 Furthermore, obesity and cardiac disorders can have a bidirectional relationship. Subjects with cardiac disease may have poor exercise tolerance and may resort to a rather sedentary lifestyle hence the propensity for developing obesity and MetS.
Our study revealed a significant association between being female with a higher risk of having MetS, which is consistent with previous studies.35,36 On the other hand, a study from India reported a non-significant association between gender and MetS. 25 Additionally, our finding indicated an association between monthly income level and MetS, this in line with the conducted in Ethiopia 29 and China, 37 although the impact may vary between developing and developed countries. Furthermore, having a history of smoking was associated with MetS in our study, it is consistent with reports from studies conducted in China 38 and Korea. 39 This could be attributed to smoking triggering the release of hyperglycemic hormones, increasing lipolysis, and exacerbating insulin resistance, all of which contribute to the development of MetS.38,39
Limitations
Our study did not utilize the general population as the control group; instead, non-cardiac patients seeking medical treatment at the hospital were included during the study period. However, we tried to compare the rate of MetS in this study with previous studies conducted on the general adult population in Ethiopia.16–19 In addition, as our study was cross-sectional, it is important to note that it cannot establish a direct causal relationship between MetS and its risk factors Last, we only employed two classification criteria to assess the prevalence of MetS; different results may have been obtained if other criteria such as the WHO and NCEP-ATP III, 2002 were used. Despite these limitations, this study provides valuable insights into MetS among adults with cardiac diseases in the limited data setting of sub-Saharan Africa, particularly in Ethiopia.
Conclusion
More than half of the subjects with cardiac diseases developed MetS, in comparison to those patients without cardiac problems. Among adults with cardiac problems, BMI, central obesity, and smoking were identified as modifiable risks associated with MetS. Hence, it is crucial to highlight the significance of addressing these modifiable risk factors early on, to minimize or prevent comorbidity and additional complications in this high-risk population.
Footnotes
Acknowledgments
We want to acknowledge nurses who were working in the chronic diseases clinic for their infinite provision throughout all pertinent data collection. In addition, our gratitude also goes to the study participants for their keen involvement in the study.
Authors’ contribution
Study concept, design, and analysis: Alemayehu Abera and Agete Tadewos Hirigo. Acquisition of data: Abera Alemayehu. Drafting and critical revision of the manuscript: Alemayehu Abera, Mekdes Shifeta, Sisay Tesfaye, Bedasa Addisu, Agete Tadewos Hirigo.
Availability of data and materials
The whole data supporting this study are included within the manuscript.
Consent for publication
Not applicable.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval was obtained from the Research and Ethics Review Committee of the School of Biomedical and Laboratory Sciences of the University of Gondar (approval no: SBMLS2789/2021). Permission was obtained from Hawassa University Comprehensive Specialized Hospital Clinical and Academic Director Office. Written informed consent was obtained from all participants before conducting data for the study, and the study was done in accordance with the code of Helsinki Declaration of ethical principles for medical research involving human beings.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.