
Abstract
Objective
Apelin is a novel adipocytokine with a significant role in ischemia/reperfusion injury that is synthesized and secreted in myocardial cells and coronary endothelium. There is debate on its value for the diagnosis and prognosis of myocardial infarction. We aimed to investigate plasma apelin level in patients with acute ST segment elevation (STEMI) and non-ST segment elevation (NSTEMI) myocardial infarction and its relationship with left ventricular function and prognostic parameters.
Methods
Forty-one patients with STEMI, 21 patients with NSTEMI and 10 patients as control group with normal coronary angiograms were included. Plasma apelin level at presentation was investigated regarding its relationship with other diagnostic and prognostic parameters.
Results
Apelin level was significantly higher in acute myocardial infarction (0.31 ± 0.56 ng/mL) compared to control group (0.08 ± 0.05 ng/mL) (p < 0.01). Likewise, it was found to be significantly higher in STEMI group (0.45 ± 0.73 ng/mL) compared to control group (0.08 ± 0.05 ng/mL) (p < 0.01). Although apelin was higher in NSTEMI group (0.13 ± 0.10 ng/mL) compared to control group (0.08 ± 0.05 ng/mL), this difference was not statistically significant (p > 0.05). No correlation was found between apelin and NT-proBNP, hsCRP, troponin, ejection fraction (EF) and Killip score (p > 0.05). A positive correlation was found between apelin and TIMI, GRACE and Gensini scores (p < 0.05). Only GRACE score was found to be correlated with apelin in MI groups.
Conclusion
Apelin level was found to be high in acute myocardial infarction. With its inotropic and vasodilator effects, apelin was thought to have a protective role against severe ischemia.
Introduction and background
At present, cardiovascular diseases are a significant cause of morbidity and mortality. Of these, one of the most serious outcomes of coronary artery disease is acute coronary syndromes. Acute coronary syndromes are classified as ST elevation myocardial infarction (STEMI), non-ST elevation myocardial infarction (NSTEMI) and unstable angina pectoris (USAP).
Apelin is a novel peptide and a member of the adipokinin family, which is an endogenous ligand for the angiotension-like receptor 1 (APJ).1,2 APJ receptor is found in heart, endothelium, lungs, kidneys and adipose tissue.3,4 Apelin is synthesized in cardiomyocytes and resides in heart tissue and circulatory system. Apelin-APJ pathway is an effective regulator of blood pressure, blood flow and many functions of the heart. The most definitive evidence regarding the physiologic functions of apelin is for cardiovascular hemostasis. 5 It has a role in regulation of the vascular tone, cardiac contractile function and fluid balance. 3 Apelin, considered to be a potent vasodilator, also has positive inotropic and diuretic effects. It is found abundantly in vascular endothelial cell. The apelinergic system is believed to play a significant role in endothelial cell proliferation and angiogenesis. 6 It was found to have effect on cardiovascular protection by suppressing oxidative stress. 7 Apelin is thought to play a role in the prognosis of ischemic events. Apelin and APJ expression was reported to increase during myocardial damage. 8 Oxygen-deprived myocardium increases apelin expression in order to support contractile function of the heart. 9 In this study, we aimed to measure apelin level in STEMI and NSTEMI patients and to investigate its relationshipwith left ventricular function and prognostic markers.
Materials and methods
Patient selection
Our study was performed as a prospective study.Eighty-nine patients admitted to University of Health Sciences Dr Siyami Ersek Training and Research Hospital, Department of Cardiology, Turkey between July and December 2011 with chest pain and who were diagnosed with STEMI or NSTEMI were prospectively included in the study. All eligible patients admitted in the given time period were consecutively included. Ten patients with no sign of valvular disease, arrhythmia, rheumatic or systemic inflammatory disease who were admitted with ongoing chest pain and to whom coronary angiography was performed to exclude acute coronary syndrome were included as the control group. The coronary angiograms of the control group revealed normal coronary arteries.
For STEMI group, 41 patients to whom percutaneous coronary intervention was performed either due to symptom duration of less than 24 hours, ST segment elevation ≥2 mm in at least two adjacent precordial leads and ≥1 mm in extremity leads lasting for more than 20 minutes or due to persistent pain for 12 hours and/or dynamic electrocardiographic (ECG) changes 10 were included. For NSTEMI group, 21 patients admitted with chest pain or equivalent symptoms, ST segment depression or T wave changes on ECG, elevated troponin I level and to whom an invasive approach was performed 11 were included in the study.
Twenty-seven patients with a history of heart failure (HF), hemodialysis, cerebrovascular accident, organ failure or shock and to whom an invasive intervention was not performed were excluded from the study.
A written informed consent was obtained from all patients included in the study. Approval was obtained from the local Ethical Committee of University of Health Sciences Dr Siyami Ersek Training and Research Hospital, Turkey (15/07/2011–02).
Study protocol
History was taken from study patients along with a detailed physical examination. Killip scores were determined. A twelve-lead ECG was done to patients within the first 10 minutes of admission. Venous blood samples were drawn at admission to measure troponin I, creatine kinase (CK), CK-MB, plasma apelin, lipid panel, NT-pro brain natriuretic peptide (NT-proBNP), high sensitive CRP (hsCRP), complete blood count, BUN, creatinine, HbA1c and INR. TIMI and GRACE scores were determined.
Acetysalicylic acid (300 mg oral loading dose) and clopidogrel (600 mg oral loading dose) were given to STEMI patients before they were taken to the catheterization laboratory. After arterial puncture, unfractionated heparin (1000 units, intravenous) was injected. Gensini scores were determined. High risk patients with intracoronary thrombus received glycoprotein (GP)IIb/IIIA antagonist. Medical treatment after percutaneous coronary intervention included acetylsalicylic acid (100 mg/day, oral), clopidogrel (75 mg/day, oral), enoxaparin (1 mg/kg/day, subcutaneous), beta blocker, statin, angiotensin converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB) and isosorbid mononitrate, if necessary.
Medical treatment was commenced for NSTEMI patients. Acetylsalicylic acid (300 mg, oral), clopidogrel (300 mg, oral), enoxaparin (1 mg/kg/day, subcutaneous), beta blocker, statin, ACE inhibitor or ARB and if needed, isosorbid mononitrate were given. Coronary angiography was urgently performed within 2 hours for refractory angina, HF, life-threatening ventricular arrhythmias or hemodynamic instability. Intervention was performed in a short time periodfor the rest of the patients as warranted by the clinical condition.
Transthoracic echocardiography was performed for all patients within the first 3 days of hospital admission.
Determination of plasma apelin level
Apelin-36 level was measured at admission to the emergency department. Venous blood samples were drawn into an EDTA-containing tube. Blood samples were centrifuged at 3500X g to separate the plasma. Plasma samples were stored at -80°C. Apelin-36 level was measured using EIA kit number 602604 (Phoenix Pharmaceuticals, CA, USA). Pasteur LP 400 was used as Micro Elisa reading device, Nephstar as nephalometry reading device and Biohit as automatic pipette.
Statistical methods
Mean, median, standard deviation, frequency, percentiles (25th-75th) and ratio values were used for the descriptive statistics of data. Data distribution was tested by Kolmogorov–Simirnov and equality of variances were checked. Kruskal-Wallis and Mann-Whitney u test were used for the analysis of parametric data. Spearman correlation analysis was used for correlation analyses. SPSS 19.0 program was used for analysis. Regression analysis, stepwise method, was performed. Age and gender were used as dependent variables if there was an effect on distribution of Apelin, Troponin I, hs-CRP, NT-proBNP, TIMI, body mass index (BMI) and GRACE as independent variables. Statistical significance level used for this study is p ≤ 0.05.
Results
General results
A total of 72 patients, 52 of whom were male (72%) and 20 of whom were female (28%) were included in the study. Of these, 41 (57%) had STEMI, 21 (29%) had NSTEMI and 10 (14%) were control group (Table 1).
Clinical and demographic characteristics and laboratory parameters according to groups.

CABG: Coronary artery by-pass grafting.
Apelin levels
Plasma apelin level measured at admission was found to be significantly higher in STEMI group (0.45 ± 0.73 ng/mL) when compared to the NSTEMI group (0.13 ± 0.10 ng/mL) and control group (0.08 ± 0.05 ng/mL) (p = 0,008; Mann Whitney U Statistic Test). Although plasma apelin level was higher in NSTEMI group than the control group, this difference did not reach statistical significance (p = 0,186; Mann Whitney U Statistic Test). Patients with acute myocardial infarction had significantly higher apelin level (0.31 ± 0.56 ng/mL) than the control group (0.08 ± 0.05 ng/mL) (p = 0,03; Mann Whitney U Statistic Test) (Table 2).
Apelin levels according to groups.
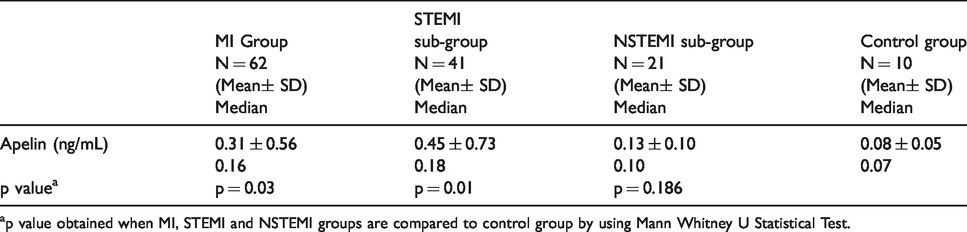
p value obtained when MI, STEMI and NSTEMI groups are compared to control group by using Mann Whitney U Statistical Test.
According to multivariate regression analysis (stepwise method), neither age nor gender distribution through AMI and control groups, showed any significant effect on apelin levels. When gender was selected as dependent variable and Apelin, Troponin I, hs-CRP, NT-proBNP, TIMI score, BMI and GRACE score as independent variables, gender showed no significant effect on apelin concentrations (p = 0.181) (Table 3). When age was selected as dependent variable and Apelin, Troponin I, hs-CRP, NT-proBNP, TIMI score, BMI and GRACE score as independent variables, age distribution showed no significant effect on apelin concentrations (p = 0.134) (Table 4).
Multivariate regression analysis (stepwise method) on apelin Levels (gender is used as dependent variable).
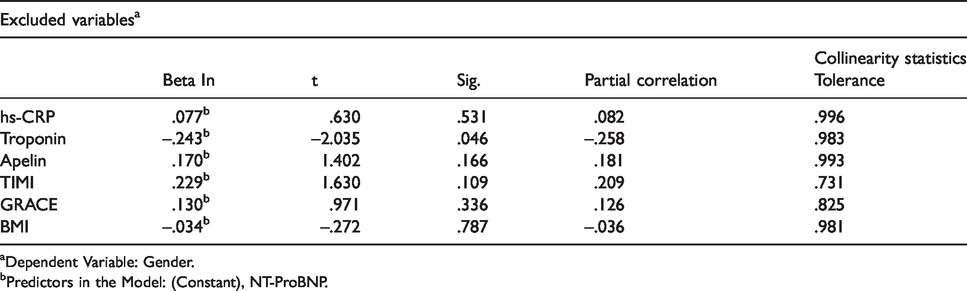
Dependent Variable: Gender.
Predictors in the Model: (Constant), NT-ProBNP.
Multivariate regression analysis (stepwise method) on apelin levels (age is used as dependent variable).
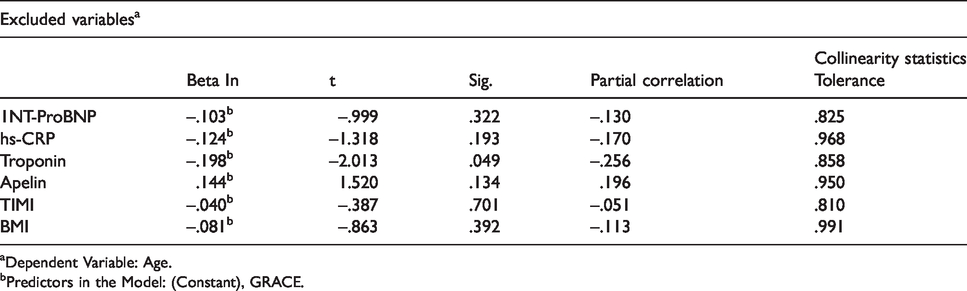
Dependent Variable: Age.
Predictors in the Model: (Constant), GRACE.
When Spearman Correlation Analysis was performed, apelin levels were found in positive correlation with GRACE, TIMI and Gensini scores (correlation coefficient, 0.444, 0.233 and 0.304, respectively and p < 0.01, p < 0.05 and p < 0.01, respectively). When only MI groups (n = 62) were selected for Spearman Correlation, apelin was found to be correlated only with GRACE score (correlation coefficient = 318 and p = 0.012).
No significant correlation was found between apelin levels and NT-ProBNP, hsCRP, troponin levels, EF and Killip score (p > 0.05).
Discussion
In our study, plasma apelin level of patients admitted with acute myocardial infarction (AMI) was found to be higher than the control group. It was demonstrated by several in-vivo and in-vitro studies that APJ gene expression is increased as a response to ischemia. 12 Apelin provides a positive effect on AMI patients by reducing the vascular tone and enhancing cardiac contractile function. Therefore, apelin was found to be increased as a response to severe necrosis and ischemia caused by STEMI. 12 Ronkainen et al. found out in an in-vivo study on rats that acute myocardial infarction leads to a temporary increase in ventricular apelin mRNA levels. It was shown that apelin might be a potential marker for acute cardiac hypoxia and might have a compensatory role in oxygen-deprived myocardial tissue. 8
Myocardial gene expression and apelin secretion are activated by hypoxia-inducible factor-1 (HIF-1). It was demonstrated in rat models that over-expression of HIF-1α reduces infarct size and decelerates the development of heart failure due to infarction. 13 In a study done on isolated rat heart by Kleinz et al., 14 it was found that apelin mRNA increases in ischemic myocardium and decreases back to its normal level after reperfusion. Sheikh et al. also demonstrated that apelin and APJ levels are rise during endothelium-limited myocardial injury. 15
Simpkin et al. 16 proposed for the first time that apelin might have a protective role against reperfusion injury. Apelin-13 was shown to reduce infarct size and post-ischemic myocardial contracture. 17 It was revealed in a recent study that the apelin-APJ system may protect the myocardium from ischemia/reperfusion injury by acting on the reperfusion injury salvage kinase pathway. 18 Zeng et al. 19 demonstrated in their study that apelin attenuates cardiac dysfunction due to ischemia/reperfusion injury by suppressing myocardial apoptosis and providing resistance against oxidative stress.
Although apelin level was found to be elevated in patients with acute myocardial infarction in our study, no significant correlation could be obtained between apelin level and prognostic markers such as NT-proBNP, hsCRP, troponin, EF and Killip score. High apelin level detected in our study, like existing literature, is thought to have a compensatory role for myocardial protection against acute ischemia. In vivo studies showing increased apelin expression during the first 24 hours of acute myocardial infarction support our study results. Oxygen-deprived myocardium accentuates apelin expression, thereby enhancing cardiac contractile function. 9 In a study by Weir et al. done in patients with an acute myocardial infarction in the last 1–14 days and whose EF < 40%, apelin-12 level measured at approximately 46th hour of admission was found to be lower than the control group. Apelin level at the 24th week was higher than the basal value, however,it was still lower than the control group. 20 We measured apelin levels at admission, before patients received any pharmacological or interventional treatment. In the study by Weir et al, blood samples were drawn 24 hours after admission; thus, patients received pharmacological or interventional treatment. The effect of treatment on apelin level was minimized in our study.
In a study by Kadoglou et al., 21 apelin-12 level was found to be lower in patients with AMI and unstable angina when compared to the control group and to patients with asymptomatic coronary artery disease. They found a correlation between low apelin level and Gensini score in patients with asymptomatic coronary artery disease. In our study, there was a positive correlation between apelin level and Gensini score. In the same study by Kadoglou et al, low apelin level was found to be correlated with hsCRP in patients with coronary artery disease. We did not find such a correlation in our study.
Severe ischemia in STEMI can lead to a high apelin level in the early period. In a study by Kuklinska et al., apelin level was found to be significantly reduced at the 5th day when compared to admission in STEMI patients; however, no relation was found between apelin level and EF. 22 The same study revealed an early increase in apelin level as a response to ischemia and a late reduction in plasma level as a result of expenditure. The lack of control group is a limitation of this study. Apelin level was found to be higher in STEMI patients when compared to the control group with normal angiography results in our study. No significant correlation was found between apelin level and prognostic markers such as NT-ProBNP, hsCRP, troponin, EF and Killip score.
We found a positive correlation between apelin level and TIMI, GRACE risk scores and Gensini score which shows the angiographic severity of coronary artery disease. When only MI groups were taken into consideration, apelin was found to be correlated only with GRACE score. It is yet unknown whether apelin may be used as a marker of prognosis and injury in AMI. To the best of our knowledge, this is the first study to demonstrate a positive correlation between apelin and TIMI, GRACE and Gensini scores. Cosansu et al. found no significant correlation between apelin and TIMI, GRACE and Gensini scores in patients with non-ST segment elevation acute coronary syndromes (NSTE-ACS) and STEMI. 23 In a study by Li et al., plasma apelin level was found to be decreased in patients with stable angina and apelin correlated negatively with Gensini score. 24
Increased apelin level in AMI as a possible protective response against ischemia may explain the positive correlation between apelin and the angiographic severity of coronary artery disease as indicated by Gensini score. Higher Gensini score showing a significant atherosclerotic burden may result in more severe ischemia, thus leading to elevated apelin level. Similarly, apelin and TIMI and GRACE risk scores may be positively correlated because higher ischemic burden results in increased mortality and event risk as reflected by higher risk scores and at the same time it leads to an increase in apelin level. The positive correlation seen between apelin level and GRACE score in MI groups but not in control group may also be explained by ischemia-mortality relation. Further studies are needed to investigate the relationship between risk scores and apelin.
Limitations of our study are low patient number, apelin measurement limited to admission and lack of evaluation of pharmacological and interventional treatment effects on apelin level. In addition, potentially confounding factors such as diabetes are not available in our study. Further studies need to be performed to investigate the effect of such confounding factors. Larger studies are also needed to investigate if apelin has a protective role against ischemia.
In conclusion, plasma apelin level was found to be significantly higher in patients admitted with acute myocardial infarction. Apelin level in STEMI group was significantly higher than NSTEMI and control groups. Apelin level in NSTEMI patients was found to be higher than the control group in our study, however no statistically significant difference was observed. There was a positive correlation between apelin level and TIMI, GRACE risk scores and Gensini score. Further large studies are needed for this purpose.
Supplemental Material
sj-pdf-1-cvd-10.1177_2048004020963970 - Supplemental material for Plasma apelin level in acute myocardial infarction and its relation with prognosis: A prospective study
Supplemental material, sj-pdf-1-cvd-10.1177_2048004020963970 for Plasma apelin level in acute myocardial infarction and its relation with prognosis: A prospective study by Ozge Guzelburc, Refik Demirtunc, Servet Altay, Tugba Kemaloglu Oz and Gulsah Tayyareci in JRSM Cardiovascular Disease
Footnotes
Contributorship
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
None.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.