
Abstract
Background
A high prevalence of stress-related disorders is well known among healthcare professionals. We set out to assess the prevalence of cardiovascular risk factors and compliance with national dietary and physical activity recommendations in NHS staff in the UK with comparison between clinical and non-clinical staff, and national surveys.
Design
A multi-centre cross-sectional study.
Methods
A web-based questionnaire was developed to include anonymised data on demographics, job role, cardiovascular risk factors and diseases, dietary habits, physical activity and barriers towards healthy lifestyle. This was distributed to staff in four NHS hospitals via emails.
Results
A total of 1158 staff completed the survey (response rate 13%) with equal distribution between the clinical and non-clinical groups. Most staff were aged 26–60 years and 79% were women. Half of the staff were either overweight or obese (51%) with no difference between the groups (P = 0.176), but there was a lower prevalence of cardiovascular risk factors compared to the general population. The survey revealed a low compliance (17%) with the recommended intake of five-a-day portions of fruit and vegetables, and that of moderate or vigorous physical activity (56%), with no difference between the clinical and non-clinical staff (P = 0.6). However, more clinical staff were exceeding the alcohol recommendations (P = 0.02). Lack of fitness facilities and managerial support, coupled with long working hours, were the main reported barriers to a healthy lifestyle.
Conclusions
In this survey of UK NHS staff, half were found to be overweight or obese with a lower prevalence of cardiovascular risk factors compared to the general population. There was a low compliance with the five-a-day fruit and vegetables recommendation and physical activity guidelines, with no difference between the clinical and non-clinical staff.
Introduction
Doctors and nurses are considered to be the guardians of public health. By nature of their training and profession, they advise people on healthy lifestyles, in addition to offering medical and surgical treatments. However, not much is known about the prevalence of cardiovascular risk factors and lifestyles of the healthcare professionals (HCPs) or other staff working in the health sector. It is recognised that doctors fail to take care of their physical and mental health and have higher levels of depression, anxiety, burnout and substance misuse than in other groups of workers.1–3 HCPs often find it difficult to seek help for their health problems, because they feel they are letting down their patients or colleagues, or for practical reasons such as workload or because they fear stigma and adverse effects on their career. 4
It is recognised that healthy and active HCPs are more likely to counsel their patients on a healthy lifestyle,5,6 be viewed by their patients as a role model, 7 and have an impact on patient care and outcomes.8,9 Moreover, healthy HCPs are vital for employers for performance and financial reasons. A report commissioned by the UK Department of Health (DoH) to assess the health and wellbeing of the staff in the NHS identified that the current levels of sickness absence in the NHS mean that more than 10 million working days are lost every year, equivalent to 4.5% of the entire workforce (equivalent to 45,000 full-time staff), and at a direct cost of £1.7 billion every year. 10 The report also recognised that healthcare in the future will have a stronger preventive emphasis than in the past, and if the NHS is to be seen to practise what it preaches it will be important that its own staff take action to reduce their own risk factors and are seen to champion lifestyle improvement. However, evidence on the current status of cardiovascular health and lifestyles in NHS staff is still lacking. A recent meeting of the International Commission on Occupational Health also recognised the importance of work-related health factors on cardiovascular outcomes. 11
The aims of this study were to assess the status of cardiovascular risk factors in NHS staff, measure their compliance with national dietary and physical activity (PA) guidelines, and perform a comparison between clinical and non-clinical staff with respect to these parameters. We also assessed the personal and organisational factors that the staff perceives to be barriers to a healthy lifestyle.
Methods
This is a multicentre cross-sectional study based on a self-reported questionnaire. Four hospitals based in and around London agreed to participate in the study. All staff directly employed by the trusts were included in the survey. Ethics approval or waiver was obtained from each of the hospital trusts.
The questionnaire was developed on a web-based platform (www.surveymonkey.com) to improve ease of completion and collection of data, and was pre-tested with 20 random staff members. The Checklist for Reporting Results of Internet E-Surveys (CHERRIES) was followed for development and reporting of the survey. 12 An email with explanation of research background, including the link to the survey questionnaire, was circulated four times within a period of 6 weeks during June–July 2015 to all the eligible staff in the four hospitals, and they were encouraged to respond on a voluntary basis. The staff had to give their consent to the questionnaire before they could proceed further, which was duly recorded. The research project was advertised on the intranet website of the trusts to raise the awareness and encourage participation, but no incentives were offered. At the end of this period, the data from the on-line questionnaire were extracted for analysis.
Survey questionnaire design
List of national standards/guidance on body mass index, diet and physical activity as outcome measures.
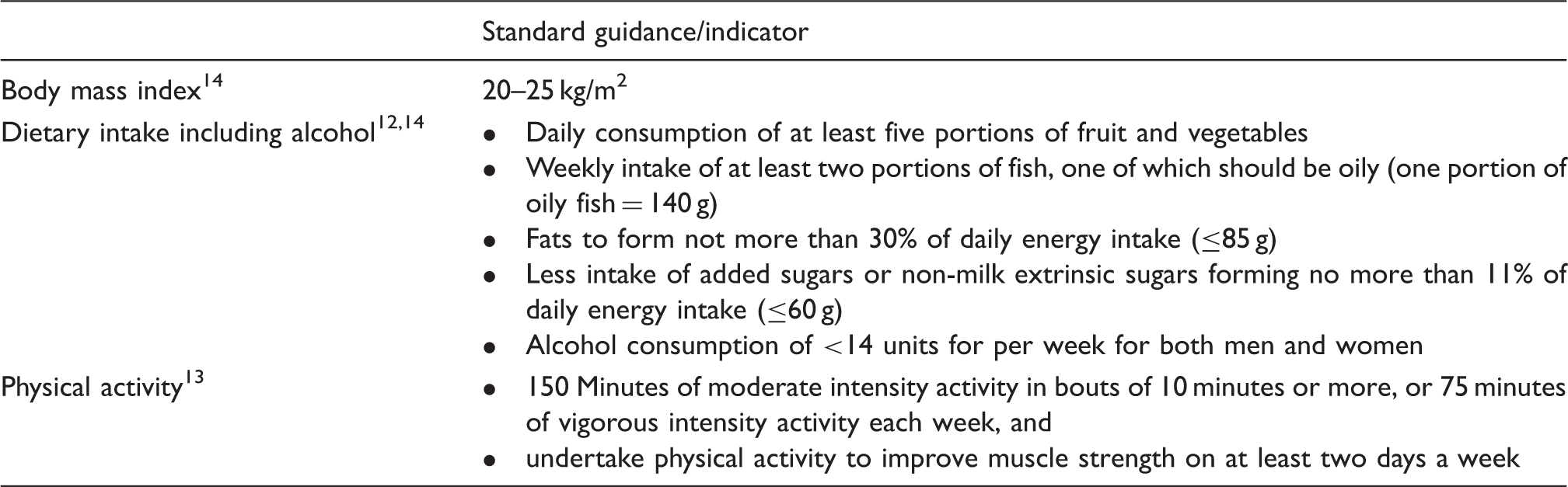
The questions on diet were obtained from the Leeds short form food frequency questionnaire (SFFFQ), 16 which has 20 food frequency questions, the responses to which are used to calculate food group or nutrient-specific daily intake and a diet quality score (DQS) in five domains (consumption of fruit, vegetables, oily fish, fats, and non-milk extrinsic sugars (NMESs)) and a total score (Supplementary file B). A DQS of 12 or more is considered to represent a healthy diet. The PA questions included the standard short international physical activity questionnaire (IPAQ) 17 to assess both leisure as well as work-related PA, and categorise total PA as moderate or more based on standard criteria (Supplementary file C). The last section of the survey consisted of questions related to work and barriers to a healthy lifestyle.
Statistical analysis
Survey response rates were assessed as view rate, participation rate and completion rate as per the CHERRIES checklist for the whole study cohort. 12 Proportions and percentages are used to describe all categorical data. The chi-square test was used to compare the gender of the clinical and non-clinical staff, while the Mann–Whitney test was used to compare the age category between groups. All questionnaire outcomes were converted to binary outcome measures. Logistic regression was used to compare the outcomes between clinical and non-clinical groups. The analyses were adjusted for age group and sex. All statistical analysis was performed using Stata v. 13.1 (Stata Corp LP, USA).
Results
A total of 1400 staff (out of approximately 9000 to whom the email was sent) gave consent to participate in the survey (view rate 15.6%). Of these, 1289 staff completed at least the first two sections (A and B) of the survey (participation rate 92.1%) while 1158 of them completed all five sections (completion rate 89.8%) (Figure 1). Nine members of staff did not give consent, while no response was obtained from the rest of the staff.
Flow chart demonstrating staff recruitment in the study.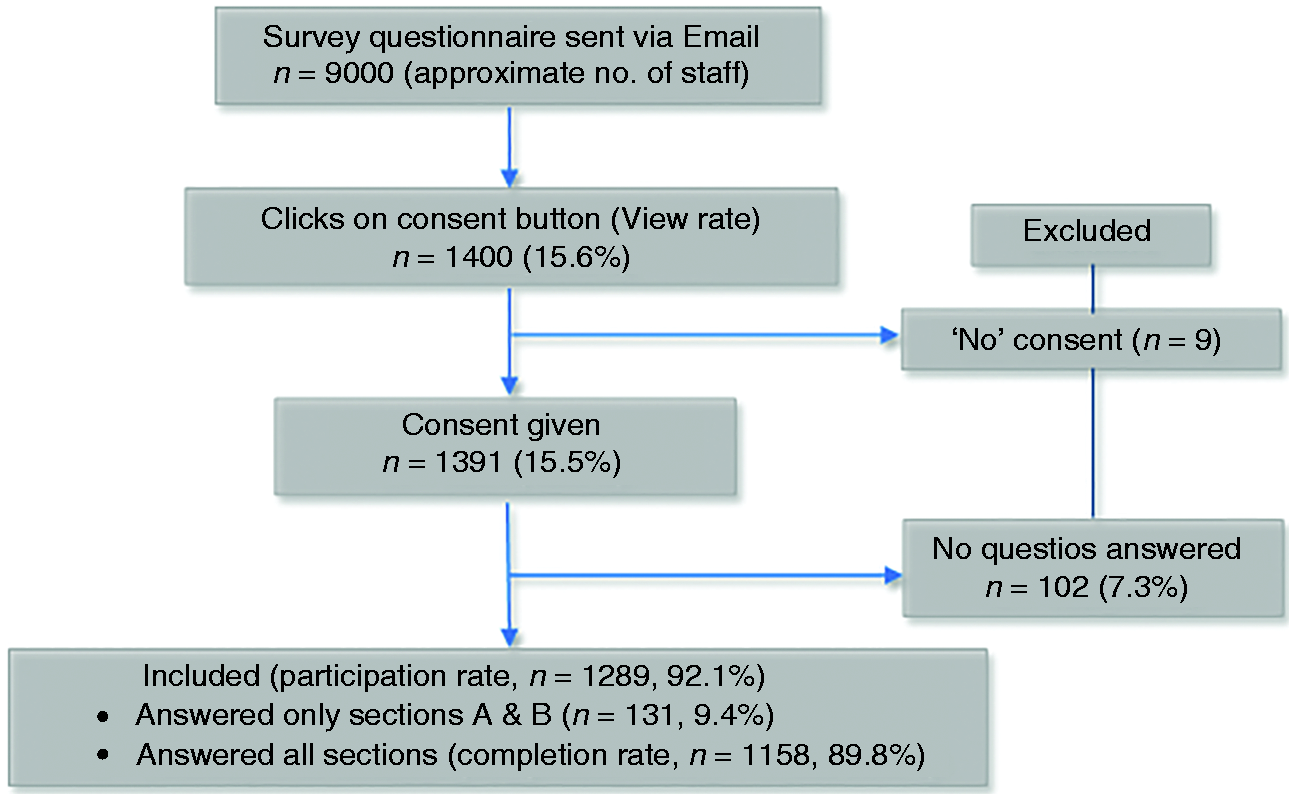
The results for demographics and risk factors along with medical conditions were analysed and reported for all the participants (n = 1289), while the responses pertaining to diet, PA and barriers to a healthy lifestyle were analysed for those who completed the whole questionnaire (n = 1158).
General characteristics
Respondents were almost equally split between clinical (n = 655, 51%) and non-clinical groups (n = 634, 49.2%). The majority (89.5%) of participants were between the ages of 26 and 60 years. There were overall more women (79%) participants, consistent with the NHS workforce. The proportion of men and women did not differ between clinical and non-clinical groups (P = 0.11). The majority of staff (1042, 81%) responded that they belonged to white British or European ethnicity, with no difference between clinical and non-clinical groups (P = 0.53).
Prevalence of cardiovascular risk factors, medical conditions and compliance with recommendations of dietary and alcohol intake, and physical activity among clinical and non-clinical staff.
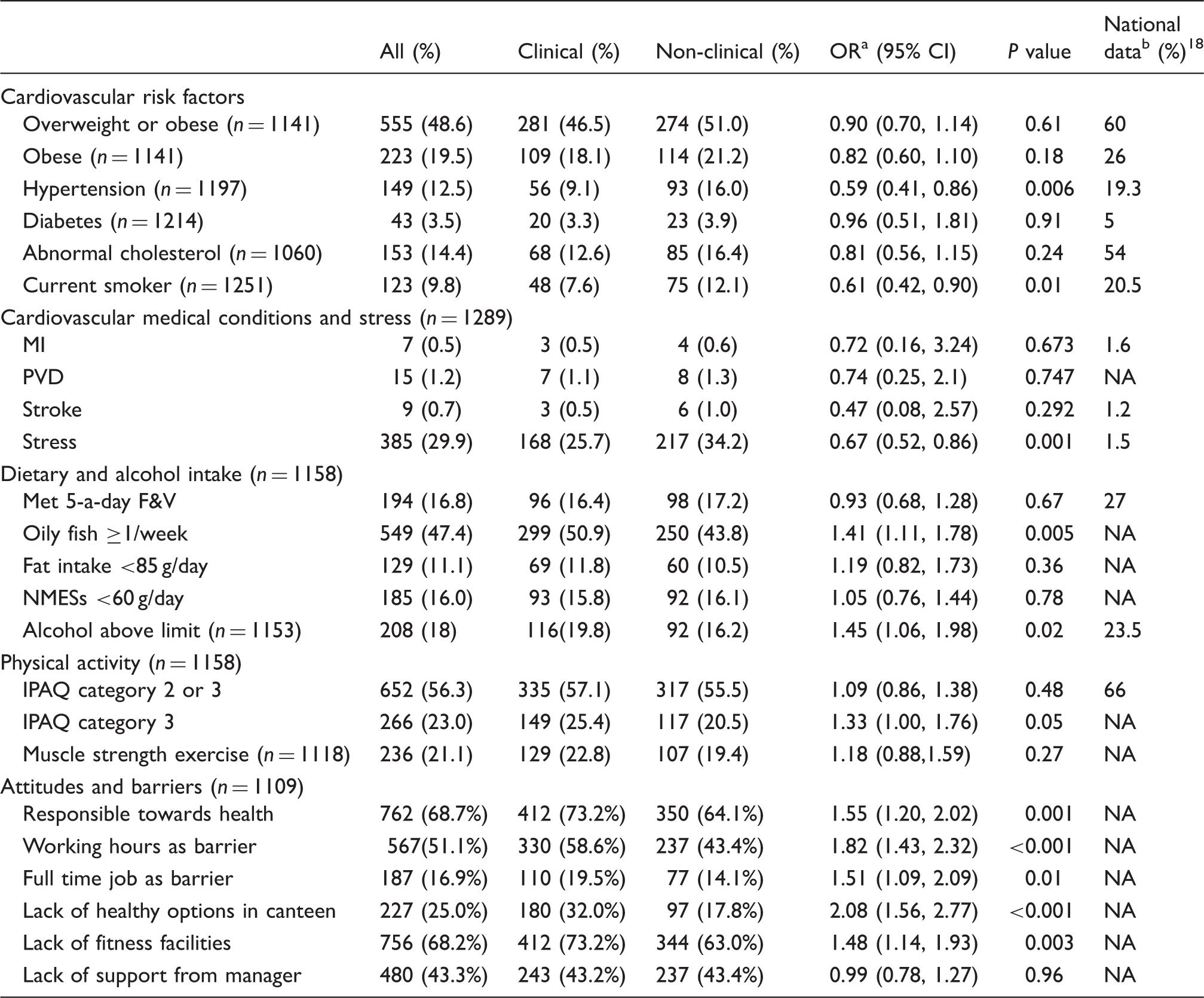
CI: confidence interval; MI: myocardial infarction; PVD: peripheral vascular disease; F&V: fruit and vegetables; NMESs: non-extrinsic milk sugars; IPAQ: International Physical Activity Questionnaire; NA: not available as proportions similar to the study.
Odds ratios are age and sex-adjusted and reported as odds in clinical group relative to odds in non-clinical group.
For ages between 16 and 64 years and averaged for both sexes, except abnormal cholesterol, which includes all ages.
Cardiovascular risk factors
The prevalence of hypertension and the number of staff smoking at the time of the survey was significantly less in clinical compared to non-clinical staff (9.1% vs. 16% for hypertension, P < 0.001, and 7.6% vs. 12.1% for current smoking, P = 0.008) (Table 2). No significant difference was seen in the prevalence of diabetes, abnormal serum cholesterol, or family history of premature coronary heart disease (CHD) between the groups. Table 2 also gives the corresponding figures for prevalence of cardiovascular risk factors in the general population from Health Surveys of England. 18
A low prevalence of cardiovascular conditions (≤1.2%) was reported among the staff, with no difference between the groups. However, a high proportion of staff reported suffering from stress-related conditions (30%), particularly in the non-clinical group (P = 0.001) (Table 2).
Dietary characteristics
Based on the SFFFQ, the recommendation for five portions of fruit or vegetables a day was met by 16.8% of the staff, with no difference in intake between the clinical and non-clinical staff (P = 0.67) (Table 2). Just under half the respondents (47.4%) consumed one or more servings of oily fish per week, being higher in the clinical group (P = 0.005, Table 2). The proportion of staff meeting the recommended intake for fat (≤85 g/day) and NMESs (≤60 g/day) was 11% and 16%, respectively, with no difference between the two groups. A total SFFFQ diet quality score of 12 or more was achieved by 8.5% and 10.9% of clinical and non-clinical staff, respectively (P = 0.18). Almost 39% of staff reported not drinking any alcohol. However, 18% drank above the recommended limit of over 14 units per week, with a greater proportion of clinical staff exceeding the limit compared to non-clinical staff (P = 0.02).
Physical activity
Sitting, as the main pattern of work, was described by 64% of the staff, with a much higher proportion in the non-clinical group (83% vs. 44.9% in clinical; P < 0.05). Almost half of the staff in each group described performing some form of PA besides work. The main reasons described for not performing PA were: not enough time (23%), lack of motivation (11.1%), physical disability (11.4%), lack of facility at work (6.1%) or near home (3.5%), and other reasons (2.6%) including tiredness, child care issues, expense, etc. If facilities were to be provided at work, 52% of staff expressed their interest in performing PA.
The short IPAQ questionnaire revealed that approximately 56% of staff undertake moderate or vigorous PA including walking (IPAQ categories 2 and 3) (Table 2). However, there was no difference between clinical and non-clinical groups (odds ratio (OR) 1.09, 95% CI 0.86–1.38, P = 0.48), even after age and sex adjustment.
Muscle strengthening exercises and yoga were being performed by 21% and 18%, respectively, of the staff, with no difference between the clinical groups.
Personal and workplace attitudes and barriers
Two-thirds of the staff (69%) felt responsible for their own health, particularly among the clinical group (Table 2). Most staff did not feel a full-time job was a barrier to a healthy lifestyle (83%) but half did express that their working hours prevented them from staying fit (51%). Lack of fitness facilities (68%), managerial support (43%), and healthy food options in the canteen (25%) were also perceived as barriers to a healthy lifestyle. While lack of managerial support was felt equally in both groups, other barriers were perceived more significantly by the clinical staff (P ≤ 0.01). Only one third (34%) of the managers were aware of the NHS health and wellbeing policy.
Discussion
Principal findings
This large cross-sectional study in four English NHS hospitals revealed the current status of cardiovascular risk factor prevalence and lifestyle factors in the form of dietary intake and PA among clinical and non-clinical staff. We found that half of the staff was overweight or obese with a low compliance with recommended dietary and PA guidelines, and there was no significant difference between the clinical and non-clinical staff. The prevalence of hypertension and smoking was less in the clinical staff, with no difference in other risk factors. The majority of staff felt that they enjoy and have a responsible attitude towards good health, but a large number find lack of fitness facilities, working hours and lack of support from their manager as barriers to a healthy lifestyle.
Comparison with national surveys and other studies
Our survey reveals that although the prevalence of diabetes and excess body weight in clinical staff is similar to that of non-clinical staff, it is lower than the UK adult general population. 18 Excess body weight and diabetes are a growing national as well as international public health issue of grave concern. 19 Only a few surveys on cardiovascular health and lifestyle from other countries have been reported, mostly performed by primary care physicians and two among cardiologists, which reveal a similar or slightly better pattern of risk factor and lifestyle patterns compared to their general population.20–25 The worst cardiovascular health profile has been shown in the survey of physicians in Bahrain, with a high prevalence of diabetes (11%) and overweight or obesity (72%). 25 The rates of BMI ≥ 25 kg/m2 reported in studies from other countries are in the range of 40–50%, which is similar to our survey. The prevalence of smoking was lowest among cardiologists in the USA at 1.3%, 20 while it was highest in Cataluna, Spain, at 19.5%, 24 compared to 7.6% in the clinical staff in this study, and 20.5% in the UK general population. 18 The lower prevalence of smoking in hospital staff could be explained by the no smoking policy within hospital buildings in the UK as well as increased awareness of the harmful effects of smoking over the past few years. 26 The proportion of physicians drinking alcohol above recommended limits has been reported to vary from 3% to 30%,20,22 being 14% in our cohort. It is to be noted that different methods have been used to measure alcohol intake in these studies. Consistent with previous studies and surveys,27,28 our study revealed a high prevalence of stress and depression, which has been related to an increased prevalence of CHD and type 2 diabetes. 29
The compliance with an intake of five portions of fruit and vegetables in our survey (17%) in both staff groups is much lower than that reported in the national survey (27%) for a similar age group. 30 Similar to national data, our survey reveals a low compliance with the intake of total fat to less than 85 g/day and of NMESs to less than 60 g/day, with no significant difference between the clinical and non-clinical staff. Long working hours and lack of suitable fruit and vegetable options in the hospitals 31 could be a contributory factor to the poor intake apart from personal dietary habits. The compliance with PA recommendations in our study is similar to that reported in the general population (67% for men and 53% for women), 32 with clinical staff not fairing any better that non-clinical staff. Other studies in HCPs have demonstrated a higher level of PA among physicians in North Ireland at 57% 21 and worse among those in Bahrain, at 10%. 25 Both work and leisure time PA has been shown to have demonstrated cardiovascular benefits in a recent large study. 33 The recommendation of performing muscle strengthening exercises was low in our study and has not been assessed in other studies.
The number of barriers to a healthy lifestyle among HCPs has been recognised. Lack of time or being too busy has been identified as the main barrier previously. 27 Poor lifestyle and organisational behaviour may cause stress among employees,10,34 and at the same time improved lifestyle, including PA, could result in less stress and better cardiovascular health outcomes besides increased productivity and patient outcomes.
In UK, the NHS is the largest employer whose employees serve the rest of the population, but their own health goes unnoticed. 34 The survey reveals that despite a number of UK DoH policies in recent years, with several recommendations for improving the health of NHS staff,10,34,35 their implementation is suboptimal. While most hospitals have occupational health services catering for vaccinations and work-related injuries, there may be a lack of a proactive approach to prevention and health promotion. This could be due to a lack of acceptance of staff health as an important issue at the senior management level. A nurse-led service can be introduced in hospitals to identify potential risk factors and provide advice on diet, weight loss, smoking cessation and stress management. Healthy lifestyle choices can be promoted by the availability of appropriate food choices in the hospital canteens, and on-site PA facilities supplemented with education and increased awareness at all staff levels.
Limitations of this study
A cross-sectional survey with self-reported data would have several limitations and sources of bias. 36 Because of the anonymous nature of this survey, comparison of respondents with non-respondents was not possible. A low response rate as is commonly found in postal or web-based surveys can introduce sampling error. Attempts were made to maximise the response rate by sending out four batches of emails with the link of the survey to all the staff over a period of 6 weeks and advertising the study on the trust intranet. We can be reasonably assured that the sample represents the distribution of staff in the trusts in clinical and non-clinical groups as it corresponds to the proportion provided by the human resources departments at the three sites. However, there may be a selection bias caused by lack of participation on the part of those staff who are less healthy or follow unhealthy lifestyles. This would be difficult to prevent as participation was completely voluntary and no attempt was made to approach the staff personally. Besides, as the survey data are self-reported, errors can arise from lack of accurate knowledge of personal body size and risk factors, and both under and over-reporting of questions related to diet and PA. To minimise such bias, validated questionnaires such as the SFFFQ for diet and short IPAQ for PA were used. Although the SFFFQ has been validated against the longer food frequency questionnaire, it still contains a fewer number of food items and hence is less robust for measuring the intake of NMESs and fat. 16
Conclusion
In this survey of NHS staff, about half of the staff was found to be overweight or obese, with a lower prevalence of cardiovascular risk factors compared to the general population. There is a low compliance with the recommended intake of five-a-day portions of fruit and vegetables and other dietary components, with no difference between the clinical and non-clinical groups except a higher proportion of clinical staff exceeding the alcohol consumption limits. Similarly, just over half of the staff is meeting the PA guidelines. The majority of staff felt that they enjoy and have a responsible attitude towards good health, but a large number identified lack of fitness facilities, working hours, and lack of support from their manager as the main barrier to a healthy lifestyle.
Footnotes
Author contribution
TKM conceived the research question with additional input from SB, TG, DAW and KK. The survey questionnaire was developed by TKM with input from CLC, JEC, SB, TG, DAW and KK. TKM and PB performed the statistical analysis. All authors provided additional intellectual content, contributed to critical revisions of the manuscript, and read and approved the final submitted version.
Acknowledgements
The authors would like to thank all the staff of the hospitals for their participation and to senior managers in the hospitals for supporting and facilitating the survey. Also thanks to Deevya Chudasama of Accent-MR, UK for her help in developing the questionnaire.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.