
Abstract
Aim
Cardiovascular diseases are the leading cause of death worldwide and physical activity (PA) practice is recommended as the most efficient preventive measure to curse their burden in sub-Saharan Africa. Our study aimed to compare cardiovascular risk factors (CVRFs) in adolescents in public and private schools in Cameroon and assess the impact of PA practice.
Methods
We conducted a cross-sectional study on students from private and public secondary schools in the city of Douala. Anthropometric parameters, blood glucose, and blood pressure (BP) were collected. PA was assessed using the short form of the International Physical Activity Questionnaire. Multivariate logistic regression was used to assess the influence of PA levels on different CVRFs. The differences were considered significant for p < .05.
Results
We recruited 771 participants, aged 16 ± 1years, 51.4% female, and 48.6% private school students. Prevalence of CVRFs was 38.4%; 11.5%; 5.6%; 5.4%, and 3% for overweight/obesity, abdominal obesity, smoking, glucose homeostasis abnormalities, and high BP (HBP) respectively. Around 41% of participants had low PA level (LPA). Abdominal obesity and LPA were more common among girls (p < .0001 both) and 1.3% of participants had more than four CVRF. In multivariate analysis, LPA was significantly associated with a higher odd of HBP (OR = 7.69; p < .0001).
Conclusion
The prevalence of various CVRF is high among Cameroonian adolescent schoolers. Public policies should focus on prevention programs through physical exercise and the reduction of smoking.
Introduction
Cardiovascular diseases (CVDs) are the leading cause of death in the world with 17.7 million deaths representing 31% of total mortality.1,2 In developed countries, 50% of the population dies from CVD and developing countries experience an increase in cardiovascular morbidity and mortality in line with economic growth. 3 Although symptoms first appear in middle age, CVD is chronic and begins in childhood. 3 Thus, cardiovascular morbidity and mortality appear earlier in developing countries due to late detection and management. 1 For decades, many studies have highlighted the importance of cardiovascular risk factors (CVRF) in the occurrence of cardiovascular events. The removal or reduction of these risk factors would be responsible for a decrease in the incidence of the disease or complications. 2 For instance, quitting smoking for three years reduces the risk of coronary events by 50%; the treatment of hypertension reduces the risk of stroke by 40% and that of myocardial infarction (MI) by 15%; the treatment of hypercholesterolemia reduces cardiovascular mortality by 30% over 20 years. 2
Studies have shown that CVRF found in adolescents is predictive of CVD complications in adults 4 and that reducing cardiovascular morbidity and mortality requires prevention and early management of these risk factors. 4 Therefore, the prevention, identification, and management of CVD in adolescents is advocated as an important precursor to reduce cardiovascular morbidity and mortality in adulthood. The increase in cardiovascular morbidity and mortality among young adults, 1 as well as its high prevalence (35%) in Cameroon, 5 make CVD an urgent public health problem emphasizing the necessity of early detection of CVRF in adolescents. School environment could play a key role in the progression of obesity and other CVRFs in developing countries 6 as students spend much of their day in school. Results on the influence of school type (e.g. private, public) on CVRFs are still controversial. Some studies show that public school students exhibit more obesity, less physical activity (PA) and less fruit consumption 7 while other studies have reported opposite trends. In Cameroon, private and public school settings are mostly different. Private schools are costly and are made for high-income families while public schools are mostly attended by low-income students. These differences can have a great impact on the environmental factors associated with CVRF and PA practice. However, these differences have not yet been evaluated in our context.
In adolescents, regular PA practice is known to prevent the onset of overweight and obesity by improving body composition and musculoskeletal health. 8 An improved cardiorespiratory fitness and body composition in adolescents has been associated with a healthier cardiovascular profile in adulthood and a significant reduction in death. 9 Regular PA in adolescence has also been demonstrated to improve cognitive function and self-esteem and reduce depression and anxiety in adulthood. 10 The World Health Organization guidelines call for children and adolescents to accumulate at least an average of 60 min of moderate-to-vigorous PA per day (mostly aerobic PA including active play, walking or biking, exercising, school-based activities, recreational activities, etc.). However, a recent report shows that more than 80% of adolescents aged 11–17 years did not meet current recommendations for PA; with 79.3% in low-middle-income countries. 11 In Cameroon, there is a lack of data on PA although some sectorial policies on PA and noncommunicable disease prevention spanning from 1974 to 2019. 12 Our study aimed to compare CVRFs on adolescents in public and private schools in Cameroon and assess the impact of PA practice.
Methods
We conducted a cross-sectional study on a population consisting of upper secondary school students from public and private management schools in Douala. Participants aged no more than 18 years, officially enrolled in one of the selected schools, having received parental consent, and at whom the questionnaires and parameters were complete have been recruited. Using a cluster sampling strategy, we randomly selected 35 students from each class in the second cycle of the selected public or private schools from each of the five sub-divisions in the city of Douala. One public and one private school were randomly drawn from each subdivision of the city. Considered “Cameroon in miniature,” Douala is an urban area, economic capital, and most populated city in Cameroon with people coming from all parts of the country.
The study was approved by the ethical committee of the Faculty of Medicine and Biomedical Sciences of the University of Yaoundé I. Authorizations from the regional delegation of secondary education and heads of the chosen institutions have been obtained before the enrollments. A consent form has been signed by each parent or guardian prior to data collection. Anthropometric, clinical, and biological data were obtained using preconceived fact sheets and validated international scales.
Physical activity measurement
Physical activity was assessed using a modified version of the International Physical Activity Questionnaire (IPAQ) short form. The questionnaire was modified according to recent validated studies.13,14 The modified version covered four domains of PA: (1) school-related PA, including activity during physical education classes and breaks, (2) transportation, (3) housework, and (4) leisure time. In each of the four domains, the numbers of days per week and time per day spent walking, moderate activity, and vigorous activity were recorded and used to calculate metabolic equivalent (METs) minutes per week. Participant's PA level was classified as high (vigorous-intensity activity on at least three days achieving a minimum total PA of 1500 MET min/week or seven or more days of any combination of walking, moderate intensity; or vigorous intensity activities achieving at least 3000 MET min/week total PA), moderate (three or more days of vigorous intensity activity and/or walking of at least 30 min per day; or at least five days of moderate intensity activity and/or walking of at least 30 min per day or at least five days of any combination of walking, moderate intensity or vigorous intensity activities achieving a minimum total PA of 600 MET min/week) or low (not meeting any of the criteria for either moderate of high levels of PA).
Anthropometric parameters
The weight was measured using an analog scale of the SECA brand. Participants were standing at the center of the scale, without shoes and with light clothing. The height was measured using a height gauge graduated in centimeters (50 to 200 cm). Participants stood, barefoot and joined, head placed according to the Frankfurt plan, arms hanging along the body and palms facing thighs. The data obtained were projected onto the curves of the International Obesity Task Force (IOTF) available from the age of 2 to 18 years, the thresholds of overweight and obesity were made by the percentile curves reaching respectively the values 25 and 30 kg/m2 to 18 years. According to the IOTF definition, overweight was defined as a body mass index (BMI) which is the ratio of weight in kilograms divided by the square of height in meters between the IOTF-25 percentile and the IOTF-30 percentile, and obesity for a BMI above the IOTF-30 percentile. 15 Waist circumference was determined using a tape and abdominal obesity was considered for a value higher or equal to the 90th percentile for age and sex. 16
Blood pressure (BP) was measured using an OMRON 705 IT electronic BP monitor validated for children and adolescents 17 ; with adapted cuffs according to standard recommendations in a quiet room after at least 10 min of resting in a sitting position. To define high blood pressure (HBP), the BP values obtained were projected onto the 2004 National High Blood Pressure curves as a function of age and gender. 18 HBP was defined as a BP greater than the 95th percentile. 18 Fasting blood glucose (FBG) was obtained after at least eight hours of overnight fasting using a ONE touch Ultra brand glucometer and appropriate test strips. Glucose homeostasis abnormalities (GHAs) were defined according to the American Diabetes Association cut-off value for an FBG ≥ 100mg/dL. 19
Statistical analysis: Data were analyzed using SPSS 20 software. Quantitative data were presented as mean ± standard deviation while qualitative data were presented as counts and frequencies. Frequencies of different CVRFs were determined and compared between groups using the chi-square test. Multivariate logistic regression was used to determine the association of low PA with some CVRFs. The level of PA was taken as the independent variable and classified into two categories: low PA level (LPA) and moderate or high PA level (MHPA). Cardiovascular risk factors were considered dependent variables and categorized as dichotomous variables. Crude odds ratios (ORs) were calculated and adjusted for age (in years), gender, and type of school. Differences were considered significant for p < .05.
Results
We approached 1000 participants and 229 were excluded mainly because of refusing blood collection and incomplete questionnaires. We recruited 771 students with an average age of 16 ± 1years and female predominance (51.4%).
Table 1 shows demographic, anthropometric, and bioclinical characteristics of the participants, compared between male and female gender. Quantitative data are presented as mean ± standard deviation. Values in brackets represent percentages for qualitative data. The mean age of the sample was 16 ± 1years and was similar between males and females. Height and weight were higher in males while BMI was similar between the two groups (p = .256). Systolic BP was higher in males while diastolic BP was similar between the two groups. The frequency of participants in private schools was 48.6% and was higher in females than males (p < .0001). The most frequent CVRF was LPA level with 41.6% followed by overweight/obesity (38.4%) and abdominal obesity represented 11.5%. GHA, HBP, and smoking represented 5.4%, 3%, and 5.6% respectively. Abdominal obesity and sedentary life were more frequent in females (p < .0001 for both) while smoking was more frequent in males (p = .003). Overweight/obesity, GHA, and HBP were similar between the two groups.
Baseline characteristics of participants.

BMI: body mass index; BP: blood pressure; CVD: cardiovascular diseases; GHA: glucose homeostasis abnormalities (FBG ≥ 100mg/dL); BPH: high blood pressure, LPA: low physical activity level.
Table 2 shows the prevalence of different CVRFs between public and private schools in the whole sample as well as in the male and female groups. In the whole sample, overweight/obesity and abdominal obesity were more prevalent in private schools than in public schools while GHA was more prevalent in public schools (p < .05). HBP, LPA, and smoking were similar between the two groups. Among female participants, overweight/obesity and abdominal obesity remained significantly higher in private schools while GHA, HBP, and LPA were significantly higher in public schools (p < .05). In the male group, no significant difference was found between the two groups for all the variables.
Prevalence of cardiovascular risk factors between public and private schools stratified by gender.
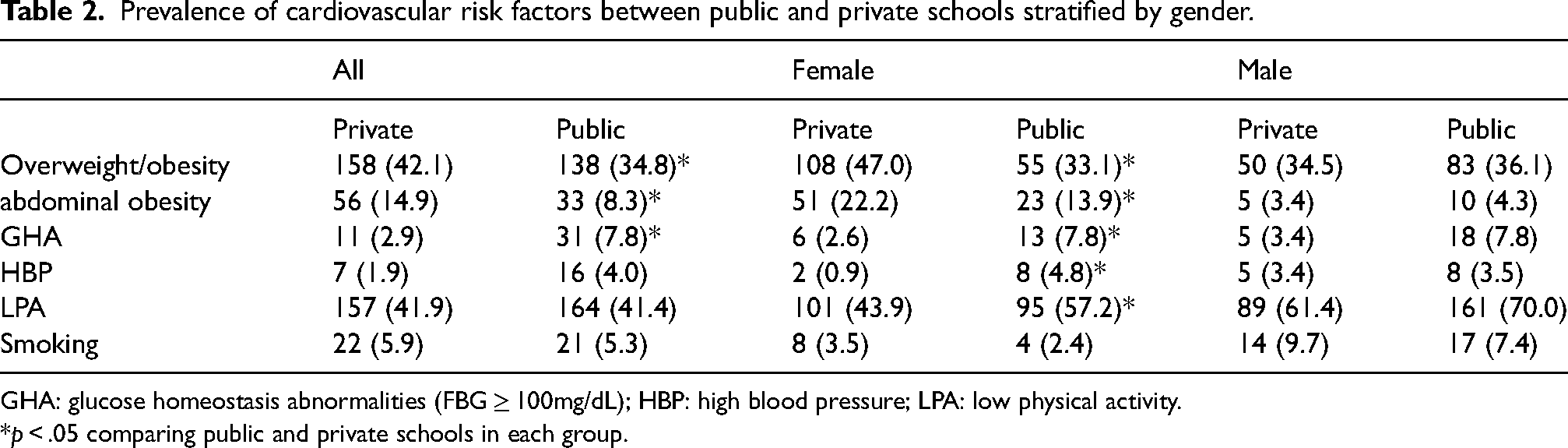
GHA: glucose homeostasis abnormalities (FBG ≥ 100mg/dL); HBP: high blood pressure; LPA: low physical activity.
*p < .05 comparing public and private schools in each group.
Figure 1 shows the frequency of the cumulative number of CVRFs (as presented in Tables 2 and 3) present in each individual. Data were compared between males and females. The frequency of participants with at least one CVRF was 67.4%. In males and females, it was 58.4% and 76% respectively. Only 1.3% of participants had four or more CVRFs. Differences between males and females were significant (p < .0001).

Distribution of the number of cardiovascular risk factors in the sample. ***p < .001; *p < .05.
Characteristics and cardiovascular risk factors according to PA level and stratified by gender.
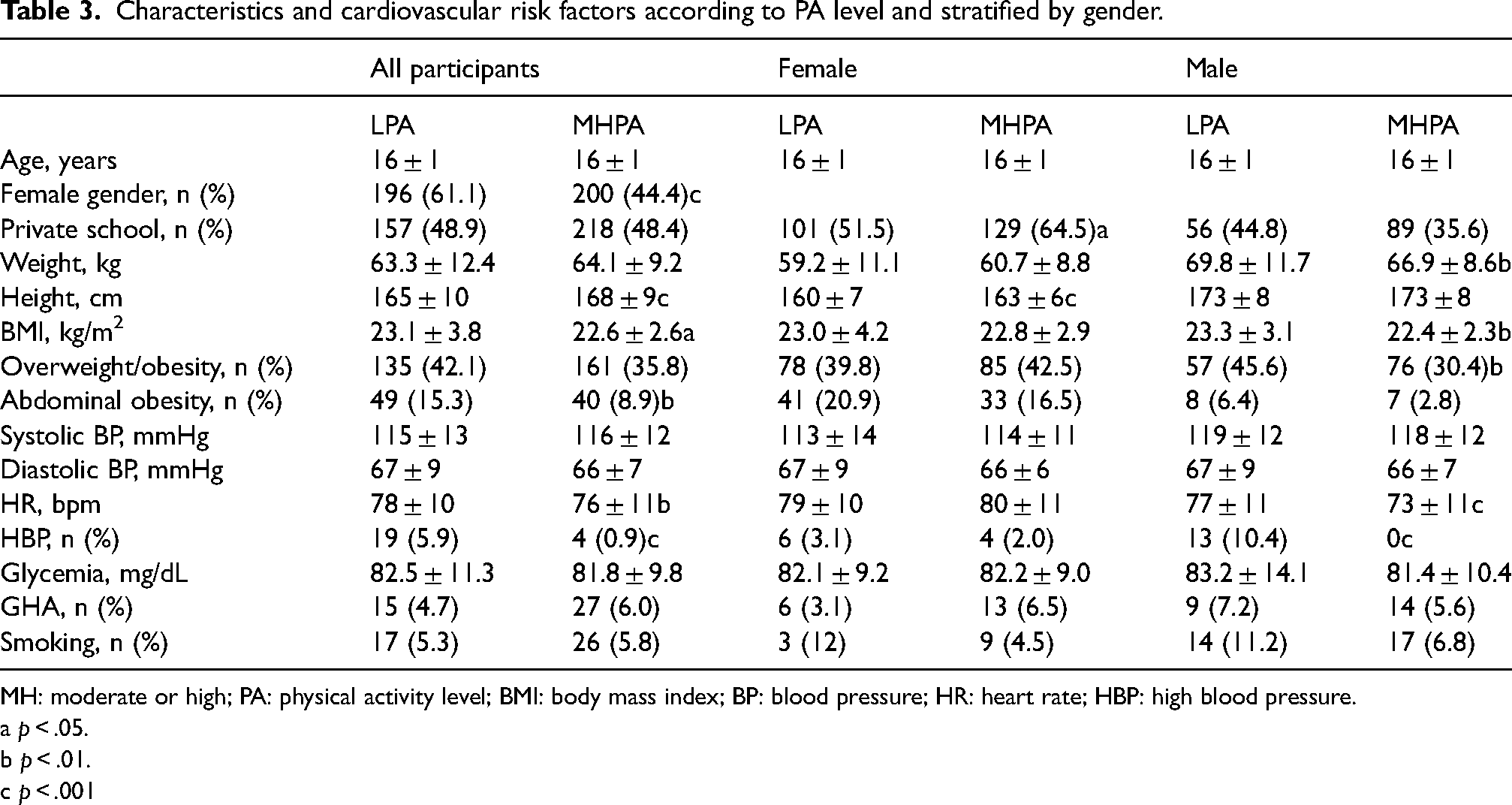
MH: moderate or high; PA: physical activity level; BMI: body mass index; BP: blood pressure; HR: heart rate; HBP: high blood pressure.
a p < .05.
b p < .01.
c p < .001
Table 3 presents participants’ parameters as well as CVRFs compared between low LPA and MHPA level participants and stratified by gender. Participants with LPA were more likely to be of female gender (p < .001). While BMI was significantly higher in participants with LPA (p < .05), overweight and obesity were not significantly different between the two groups. Abdominal obesity and HBP were also significantly higher among participants with LPA (p < .01 and p < .001 respectively). Among female participants, private school students were more likely to have MHPA compared to others (p < .05). All CVRF frequencies were similar between the two groups. Among male participants, overweight/obesity and HBP prevalence were significantly higher among LPA participants compared to the others (p < .01 and p < .001 respectively).
Table 4 shows univariate and multivariate analysis of some CVRFs (taken as the dependent variable) with PA level (taken as the independent variable). In univariate analysis (Model 1), LPA was associated with higher odds of abdominal obesity (OR = 1.85; p = .007) and HBP (OR = 7.14; p < .0001). After adjusting for age, gender, and type of school (Model 2), abdominal obesity was no more significant while LPA remained associated with higher odds of HBP (OR = 7.69; p < .0001). Differences were not significant for other parameters.
Multivariate association of physical activity level with some cardiovascular risk factors.

GHA: glucose homeostasis abnormalities; BP: blood pressure; OR: unadjusted odd ratio; ORa: adjusted odd ratio; CI: confidence interval; LPA: low physical activity; MHPA: moderate or high physical activity; Model 1: unadjusted; Model 2: adjusted for age, gender and type of school.
Discussion
In this cross-sectional study on Cameroonian students from public and private secondary schools, some important findings can be highlighted: in our young population, 67.4% had at least one CVRF, with a female predominance and up to 1.3% of students were found with at least four cardiovascular factors. Low LPA and overweight/obesity were the most frequent CVRFs with 41.6% and 38.4% respectively. Abdominal obesity and LPA were more common in females while smoking was more frequent in males. Overweight/obesity was most common among private school students while LPA was common among public school students. After adjusting for some cofounders, LPA was significantly and strongly associated with HBP.
Overweight and obesity were present in 38.4% of participants, with a significantly higher prevalence in private facilities. This prevalence is higher than the 23% found by Epacka et al. among adolescents in Cameroon. 5 In the United States, 36% of children and adolescents are overweight or obese 20 ; in Tunisia, overweight and obesity affect 25.4% of schoolchildren aged 6 to 12 years. 21 The prevalence of overweight/obesity varies greatly from study to study, year to year, and country to country. These variations can be explained by the difference in the assessment scales used: 8.7% according to the IOTF and 14.7% according to the French reference curves in the same study conducted in Tunisia. 21 Overweight/obesity was more common in girls than in boys and in private school participants compared to public ones, particularly in the female group. These findings are contrary to that of a previous study on adolescents in Argentina where they found 15% and 14.2% for overweight/obesity in public and private schools respectively. 22 These differences can be explained by differences in school facilities between the two countries. In Cameroon, private schools are mostly expensive and are reserved for high-incomes families. Children from those families are mostly obese because of their high-caloric diet. However, this explanation is not conclusive because we could not assess the socioeconomic status of our participants’ families. Further studies are necessary to bring more details.
GHA which includes prediabetes and diabetes was found in 5.4% of the population although only one participant presented an FBG ≥ 126mg/dL. This prevalence was significantly higher among female pupils in public schools. Prediabetes in adolescents is known as a precursor of type 2 diabetes in adulthood. 23 Our results were similar to those of Epacka et al. in a cohort of Cameroonian adults 24 and lower than 12.3% and 8.4% among adolescent boys and girls in India, respectively 25 as well as 15% found in 2016 in a population aged 18 to 23 years in Pakistan. 26
The 3% prevalence of HBP found in our population was close to the 2.2% prevalence found in a population of high school students by Silverberg et al. 27 and the 4.4% recently found in a population of adolescents in Nigeria. 28 The relatively young age of our population is thought to be responsible for a low prevalence of HBP as it is well known that hypertension prevalence increases with age. The significantly low prevalence of HBP in private compared to public schools is coupled with LPA which was significantly common in private compared to public schools. Furthermore, LPA was strongly associated with HBP after adjustment for age, gender, and school facility. The negative association of PA has already been demonstrated.29,30 The BP lowering effects of PA can be mediated by neurohormonal, vascular, and structural adaptations, such as the higher release of nitric oxide, a reduction in peripheral sympathetic nervous activity, a reduction in the release of catecholamine, and a decrease in arterial stiffness.31 Differences in PA levels found between public and private schools can be explained by the socio-economic status of private schools with an environment that incites PA practice. Public policies should focus on socio-economic disparities in school education systems that can hinder PA practice among school adolescents.
Some limitations can be highlighted in this study: lipid profile has not been included in the evaluation of CVRFs in our study. This is mainly due to the reticence of students and their parents who did not want us to collect and carry their blood to the lab. We could only obtain the collection of a drop of blood and its analysis per se for FBG. The evaluation of PA level has been made using a psychometric tool but not using direct measures like a cyclo-ergometer. Although we used a validated questionnaire, the results could not reflect the real PA level. The conclusion of our study should be taken with caution because of the observational design although longitudinal studies have drawn almost the same conclusion about the protective impact of PA on BP.31 Finally, although the sample size of the study was sufficient, splitting it into different groups could have reduced the statistical power. Further studies involving more participants in public and private will increase the statistical significance of the study and strengthen the conclusions drawn.
Conclusion
The prevalence of the various CVRFs is high among Cameroonian adolescents and accounts for more than half of the population. Effective implementation of school curricula, sports clubs, television programs, anti-smoking laws, and the strengthening of screening programs for the sole purpose of educating, preventing, detecting, and managing these various risk factors is imperative work for Cameroon.
Footnotes
Acknowledgments
We thank all participants who accepted to be enrolled, all teachers, and monitors who facilitated the communication with participants and all administrative authorities who helped with the procedures.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Study approved by the ethical committee of the Faculty of Medicine and Biomedical Sciences of the University of Yaoundé I (N°238/UY1/FMSB/VDRC/CSE).
Authors’ contributions
F.K., A.M., and A.D. designed the study protocol and provided support for the materials. M.A.P.O.M, J.F.K., and O.M., contributed to logistic and data collection; E.C.B.L. and J.M.N. led the statistical analyses and contributed to the manuscript draft. F.C. and E.C.B.L. wrote the first manuscript draft. S.M., L.V., H.N., C.N., S.D., and M.S.N.E. critically contributed to analysis, discussion, and interpretation of the data, and to the writing of the manuscript. All authors reviewed and approved the final manuscript draft.