
Abstract
In patients treated with macitentan (Opsumit®, Actelion Pharmaceuticals Ltd., Basel, Switzerland) for pulmonary arterial hypertension (PAH), prevention and/or effective management of treatment-related adverse events may improve adherence. However, management of these adverse events can be challenging and the base of evidence and clinical experience for macitentan is limited. In the absence of evidence, consensus recommendations from physicians experienced in using macitentan to treat PAH may benefit patients and physicians who are using macitentan. Consensus recommendations were developed by a panel of physicians experienced with macitentan and PAH using a modified Delphi process. Over three iterations, panelists developed and refined a series of statements on the use of macitentan in PAH and rated their agreement with each statement on a Likert scale. The panel of 18 physicians participated and developed a total of 118 statements on special populations, add-on therapy, drug–drug interactions, warnings and precautions, hospitalization and functional class, and adverse event management. The resulting consensus recommendations are intended to provide practical guidance on real-world issues in using macitentan to treat patients with PAH.
Macitentan (Opsumit®, Actelion Pharmaceuticals Ltd., Basel, Switzerland) is a dual endothelin receptor antagonist (ERA) that was approved in the United States in 2013 for the treatment of pulmonary arterial hypertension (PAH) (World Health Organization [WHO] Group 1) based on data from the pivotal SERAPHIN trial.1,2 Macitentan, like other ERAs, can cause a spectrum of adverse effects ranging from minor nuisance problems to severe adverse drug reactions, some of which may be difficult to differentiate from disease-related complications. When using targeted therapies such as macitentan to manage patients with PAH, prevention and/or effective management of these adverse events may help optimize adherence and set expectations to keep patients on treatment. 3
Nonetheless, optimizing the prevention and management of adverse events can be challenging and the best strategies have not been defined. The challenge may be particularly acute for recently introduced medications, such as macitentan, due to a limited base of evidence and clinical experience on adverse event management. The prescribing information and published pivotal trial data on macitentan provide an essential foundation of knowledge on its efficacy, safety, and use. However, these sources do not incorporate important real-world, experiential learning on the practical use of macitentan, such as detailed data on adverse event management and dose titration reports.
Physicians who use macitentan in treating patients with PAH need to alleviate or prevent macitentan-related adverse events and manage other specific circumstances appropriately, despite the paucity of relevant evidence and lack of evidence-based recommendations. Both physicians and patients may benefit from expert advice from physicians experienced in the treatment of PAH and the use of macitentan. 4 The Delphi method is a well-known approach for developing and recording consensus advice when evidence is not available.5–10 The study is intended to provide consensus recommendations for the management of PAH with macitentan based on the current practice in the United States using a Delphi process with a panel consisting of US-based physicians familiar with this medication.
Methods
A modified Delphi process was used to develop the consensus. The Delphi process was originally described by Delbecq et al. and has been reviewed previously.11–15 The current study was conceived by one author (FFR), who also served as a study moderator and recruited the Delphi panelists. The target Delphi panel size was 20 members. Initially, the US investigators in the SERAPHIN pivotal trial of macitentan with the largest numbers of patients were invited to participate. Then, members of the Pulmonary Hypertension Association who were located in the United States and listed in the Association’s database as managing at least 200 patients with pulmonary hypertension were then invited in alphabetical order until the target panel size was reached. The 200-patient threshold was selected because it represents the most experienced category listed in the Pulmonary Hypertension Association database and because the moderators felt that it was adequate to demonstrate appropriate expertise in PAH for the purposes of the study. The actual number of patients with PAH under active management was verified by panelist self-report. All panelists who participated actively in the Delphi process (defined as completing and returning at least two out of three questionnaires including the final questionnaire, and reviewing the draft and final manuscripts) met the International Committee of Medical Journal Editors criteria for authorship and are included as co-authors.
For this study, the modified Delphi procedure used three questionnaires, which included statements based on the macitentan prescribing information,
1
the published results of the SERAPHIN trial,
2
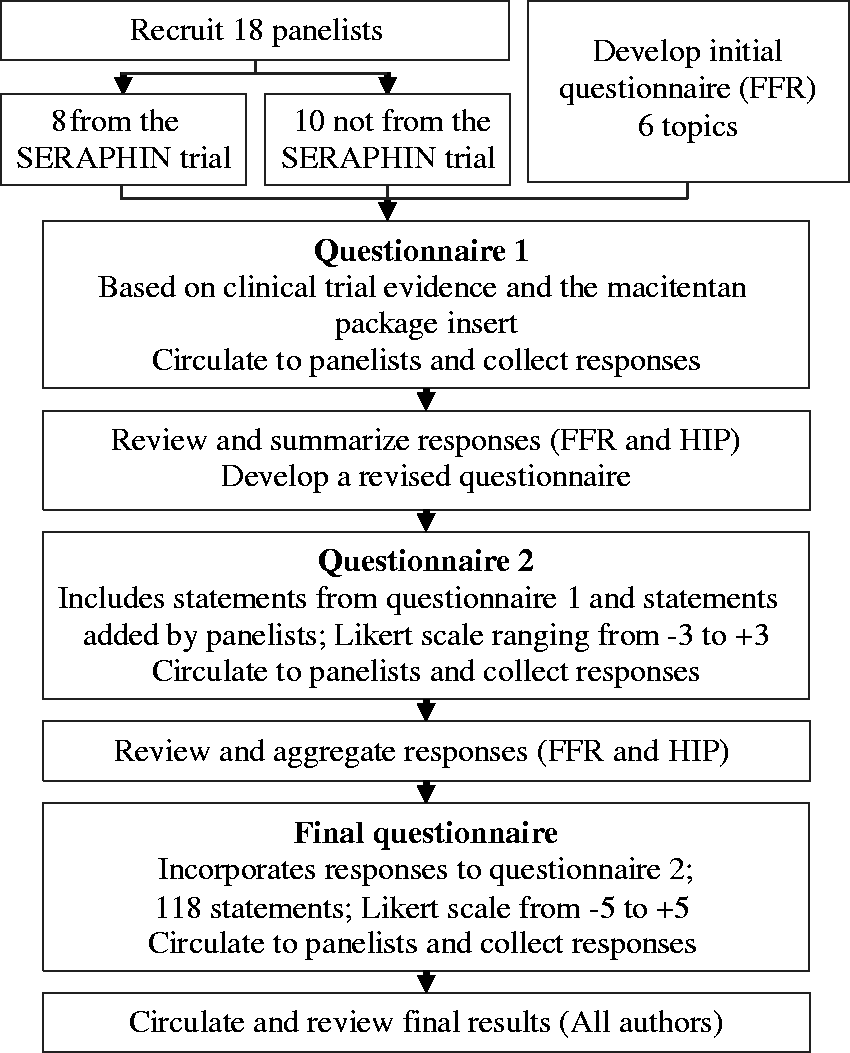
and the panelists’ clinical experience. The procedure was as follows (Fig. 1):
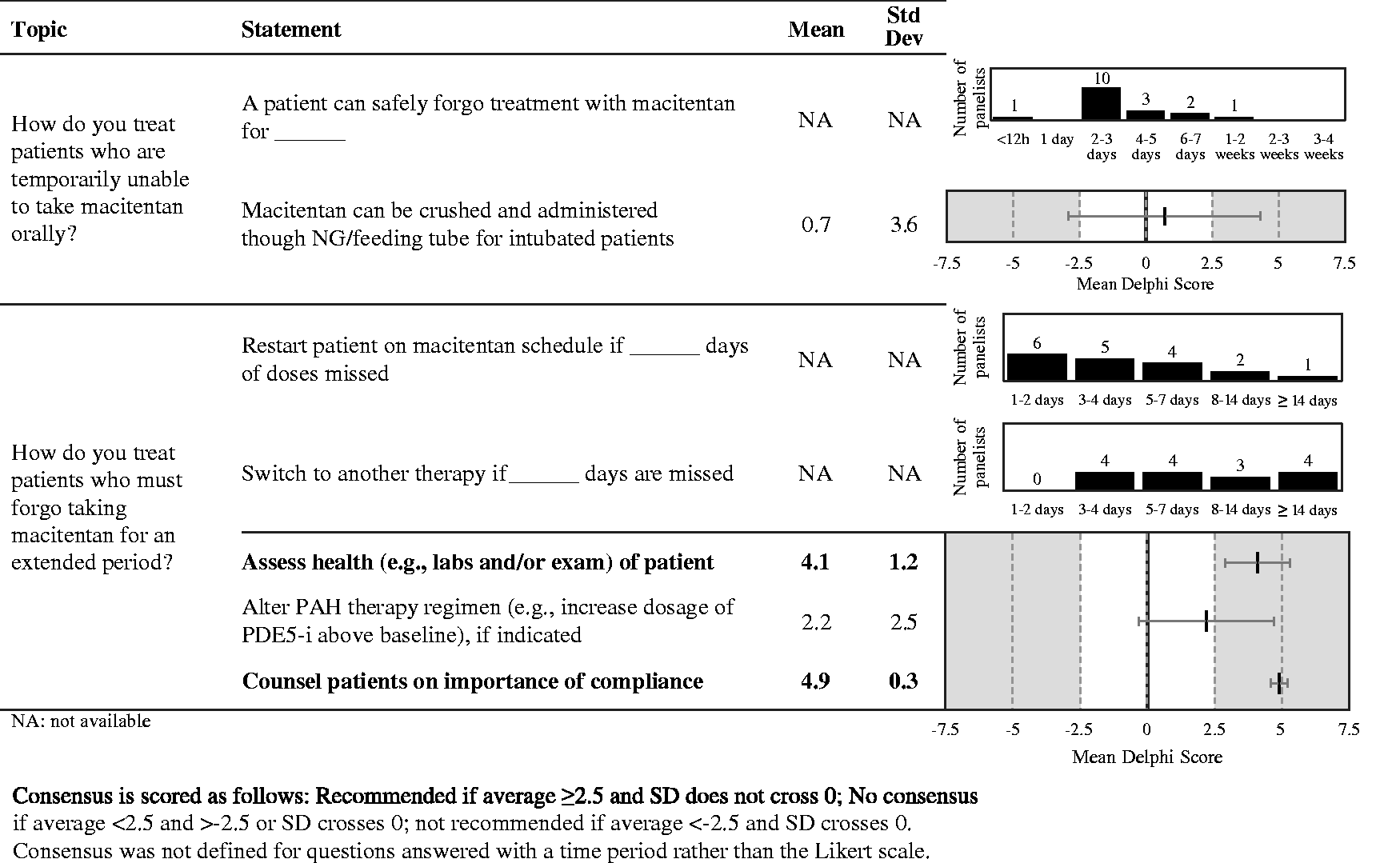
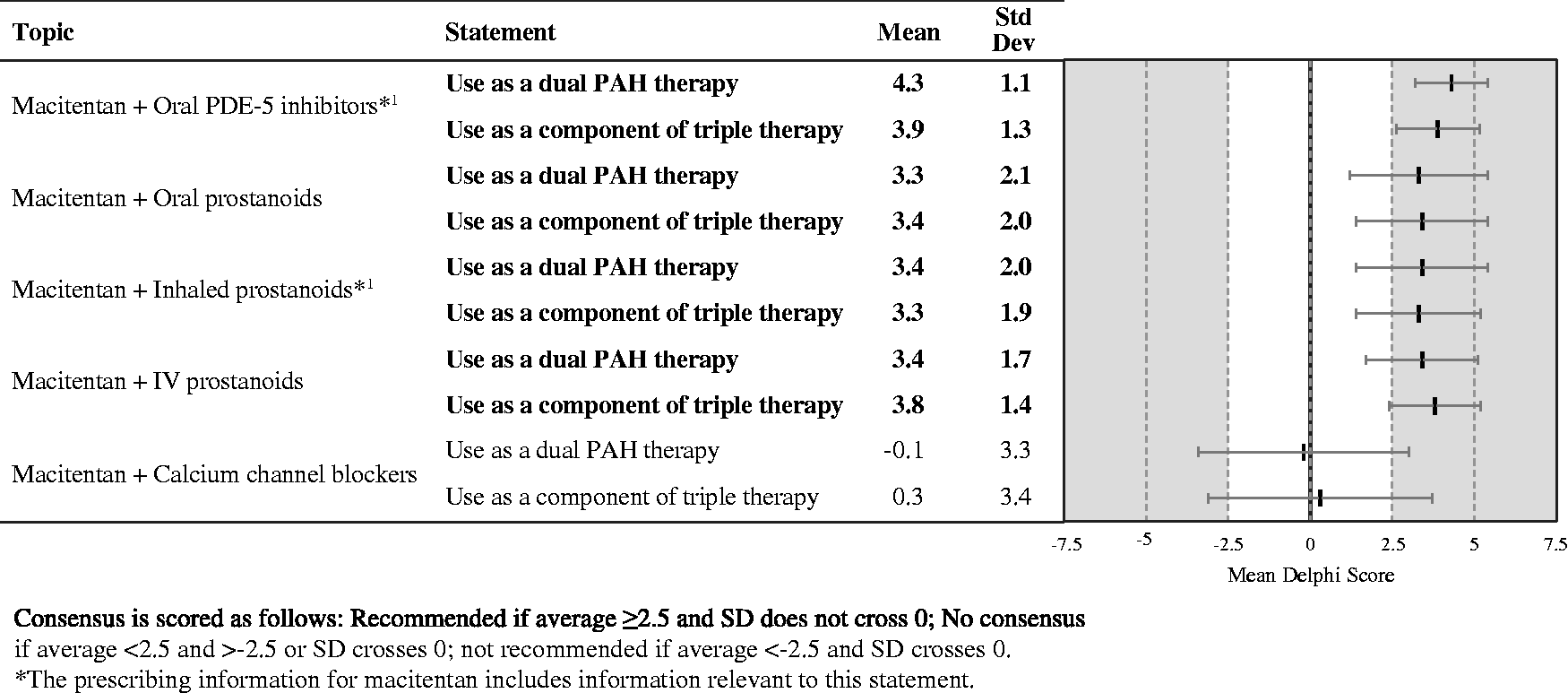
The moderator (FFR) developed an initial questionnaire based on available clinical trial evidence and the macitentan package insert.1,2,16,17 The initial questionnaire was a topically organized spreadsheet with multiple statements relevant to the use of macitentan. Panelists were requested to provide open-ended comments on each statement and to add additional relevant statements at their discretion. The initial questionnaire was circulated to the Delphi panelists by email. Panelists responded independently. At this point two moderators (FFR and HIP) reviewed and summarized responses to the initial questionnaire and used the responses to develop a second questionnaire spreadsheet that incorporated the initial statements and additional statements added by the panelists without changing the overall organization. The second questionnaire requested panelists to rate each statement on a numeric Likert scale ranging from –3 (strongly disagree) to 3 (strongly agree). The second questionnaire was circulated to the Delphi panelists by email. The moderators reviewed and aggregated responses to the second questionnaire into a summary spreadsheet and used them to refine the questionnaire to create a third and final version, shown in Figs. 3–8. The final questionnaire requested panelists to rate each statement on a numeric Likert scale ranging from –5 (strongly disagree) to 5 (strongly agree) to improve discriminant ability. In addition, several questions asked panelists to select a time period rather than indicate their agreement/disagreement. Details of the time periods are shown in Figs. 1 and 4. The summary and the final questionnaire were circulated to the Delphi panelists by email. The results of the final questionnaire were aggregated into a summary spreadsheet and circulated to the panelists for review and comment. The Delphi process used in the study. The Likert scale used in the final stage of the Delphi process. Delphi consensus results—special patient populations. Recommendations that achieved consensus are in bold. Delphi consensus results—use of add-on therapy, “What is your opinion of co-administering macitentan with other PAH therapies?” Recommendations that achieved consensus are in bold. Delphi consensus results—drug–drug interactions. Recommendations that achieved consensus are in bold. Delphi consensus results—warnings and precautions. Recommendations that achieved consensus are in bold. Delphi consensus results—hospitalization. Recommendations that achieved consensus are in bold. Delphi consensus results—adverse events frequency and management.
Following standard practice for the Delphi methodology, the panelists’ anonymity was maintained throughout the process. Anonymity is deemed essential in Delphi methodology to prevent bias by influential clinicians and to reduce the pressure towards conformity. Panelists were encouraged to comment on the validity, specificity, and content of the items under consideration. All comments were incorporated verbatim and anonymously in the statements and questionnaires distributed to panelists in each round. Panelists were also encouraged to provide questionnaires and provide relevant literature. All literature referenced in the statements was circulated to the entire panel for reference and independent examination.
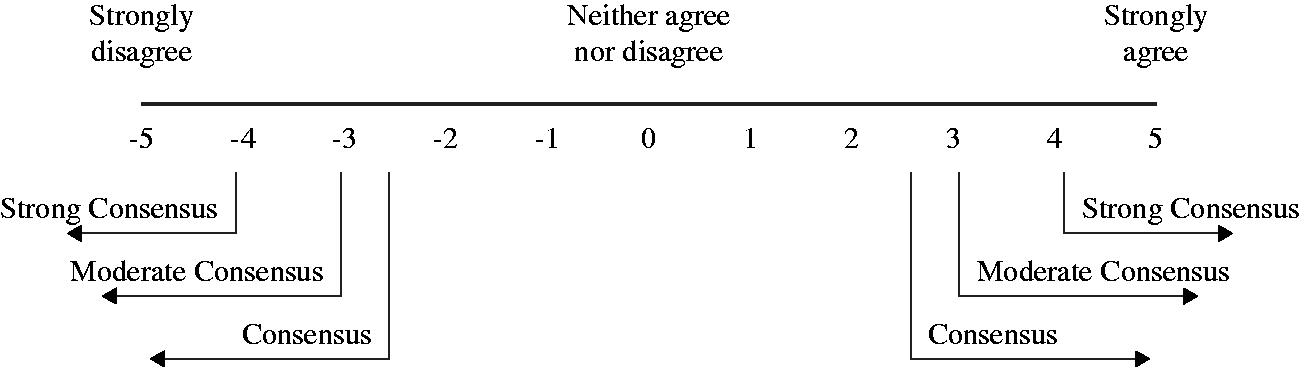
Consensus was defined prospectively as a mean panelist rating ≥2.5 or ≤ –2.5 on the –5 to +5 Likert scale used in the final questionnaire, with a standard deviation that did not cross zero (Fig. 2). Strong, moderate, and weak recommendations were defined retrospectively as a mean panelist rating absolute value ≥4.0 (strong recommendation), ≥3.0 and <4.0 (moderate recommendation), and ≥2.5 and <3.0 (weak recommendation). Consensus was not defined for questions answered with a time period rather than the Likert scale.
Results
A total of 18 physicians joined the Delphi panel, including eight SERAPHIN investigators and ten members of the Pulmonary Hypertension Association who were not SERAPHIN investigators. The number of patients with PAH under active management for individual panelists was in the range of 90–1200. All 18 panelists participated actively in the Delphi process. The final Delphi questionnaire was divided into six topics including 118 statements. All statements and the results of the final questionnaire are shown in Figs. 3–8.
Panelists strongly recommended that patients who have forgone macitentan for an extended period should undergo a health assessment and be counseled on the importance of compliance (Fig. 3). Consensus was not evaluated on the duration for which patients can safely forgo treatment with macitentan, when macitentan should be restarted after missing doses, or when another therapy should be started after missing macitentan doses.
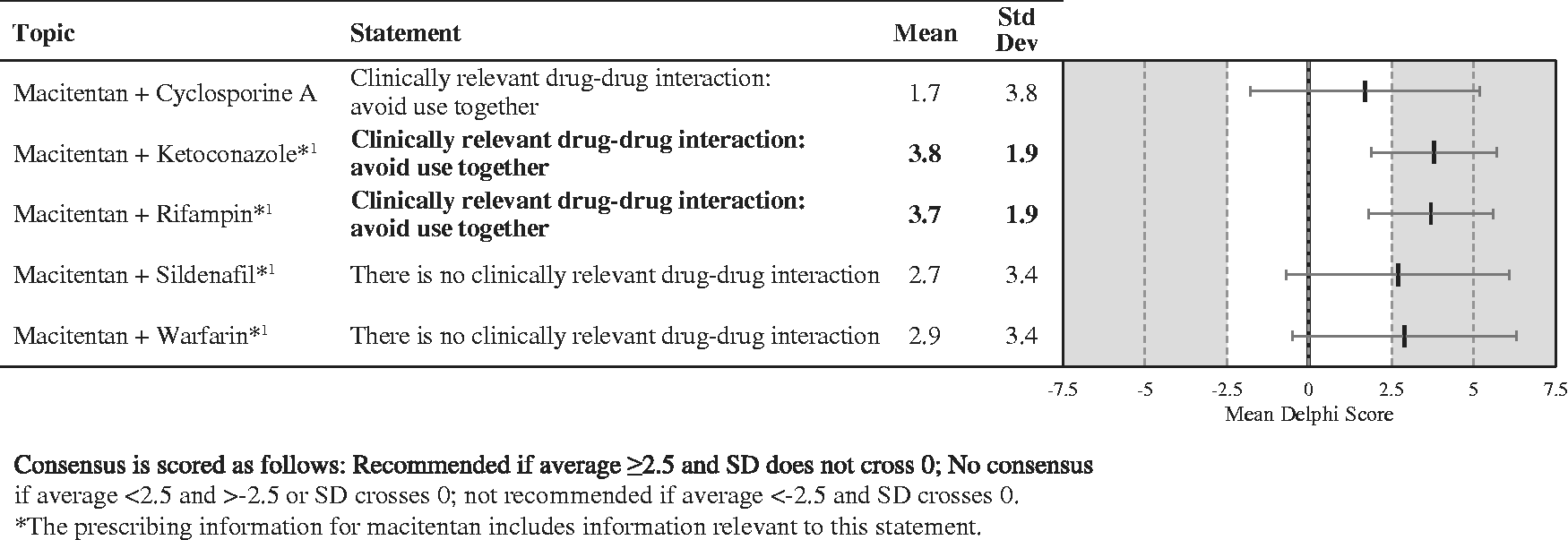
Panelists reached a consensus that macitentan can be used as dual therapy with oral phosphodiesterase type 5 inhibitors (PDE5-i) and oral, inhaled, or intravenous (IV) prostanoids. The strongest recommendation was for use with PDE5-i (Fig. 4). Panelists also reached consensus that macitentan has clinically relevant drug–drug interactions with ketoconazole and rifampin and should not be used concomitantly with these agents (Fig. 5).
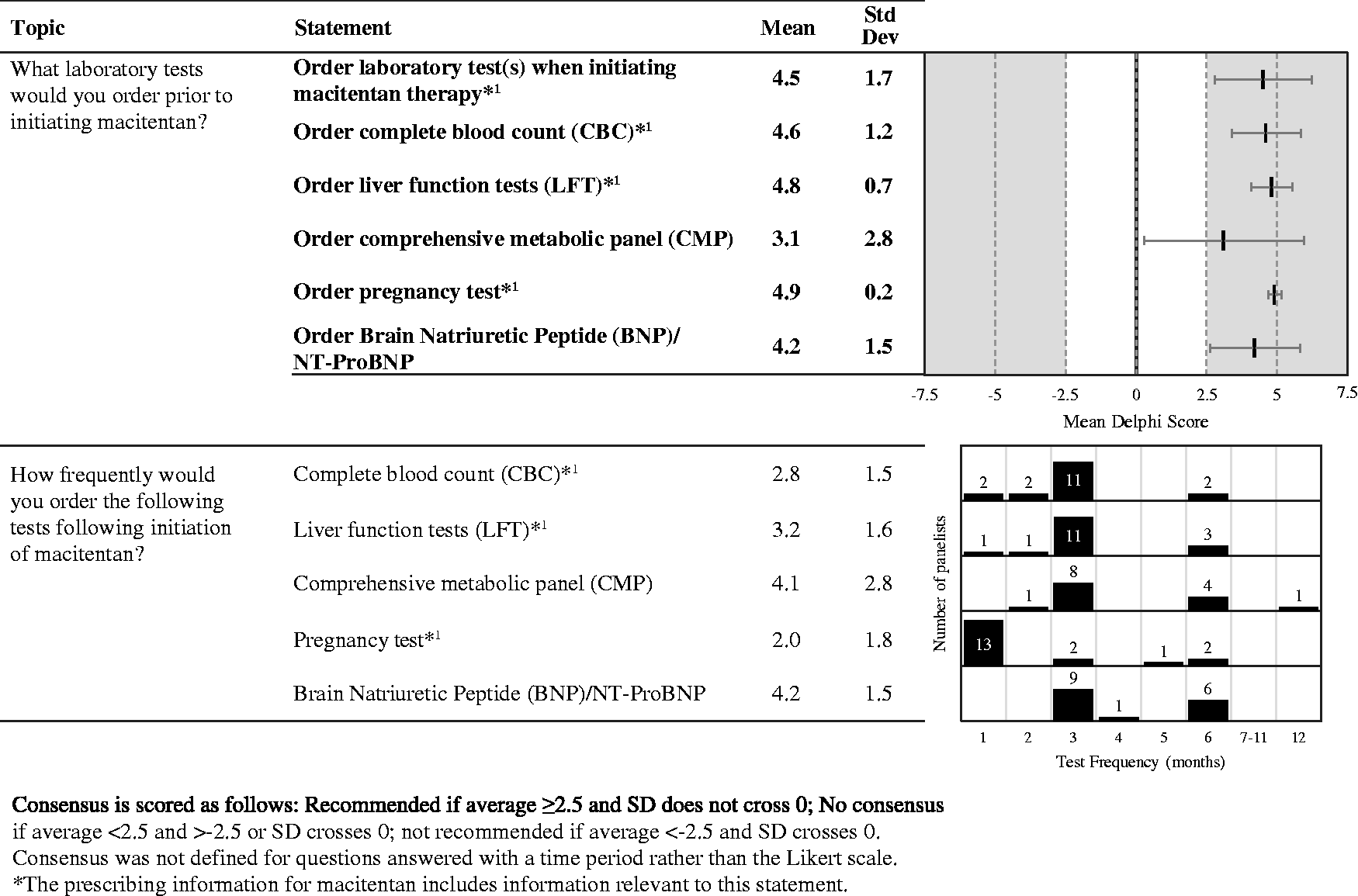
The group recommended laboratory testing when initiating macitentan, with a strong consensus for laboratory testing generally and the following specific tests: complete blood count; liver function tests; pregnancy test (in women of childbearing potential); and brain natriuretic peptide or N-terminal pro b-type natriuretic peptide (NT-proBNP). There was a weak consensus for also ordering a complete metabolic panel. Most panelists recommend monthly pregnancy testing with a complete blood count, liver function testing, a comprehensive metabolic panel, and brain natriuretic peptide assessments every three months (Fig. 6). Note that the prescribing information for macitentan requires monthly pregnancy testing for all women of childbearing potential taking macitentan.
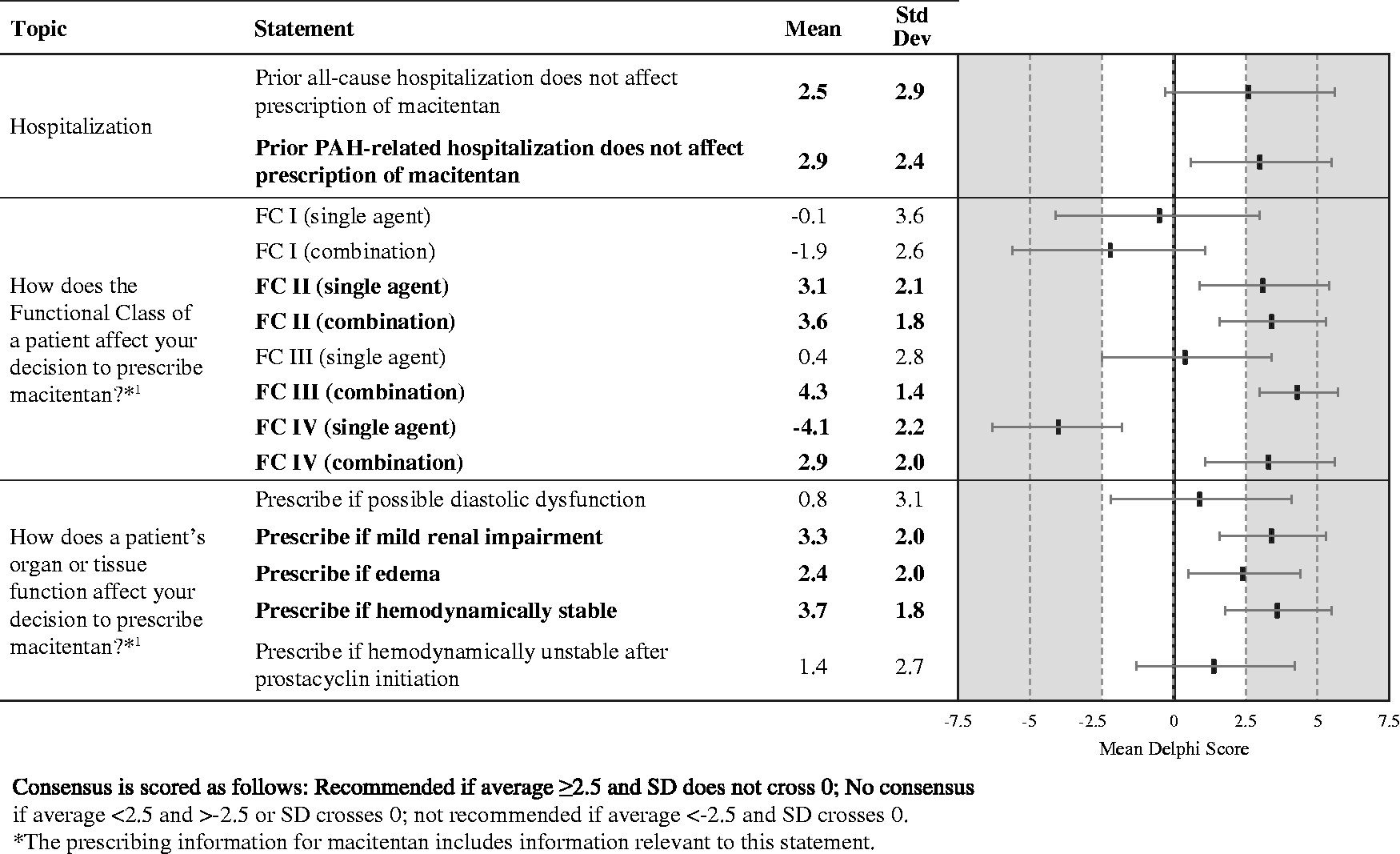
The panelists recommended that prior hospitalization for PAH should not affect use of macitentan. In addition, panelists strongly recommended use of macitentan as part of a combination in treating patients with modified New York Heart Association functional class (FC) II, III, or IV and as single agent therapy for FC II (Fig. 7). Use of macitentan as a single agent is not recommended for patients with FC IV. There was also a consensus for use of macitentan in patients with mild renal impairment or if hemodynamically stable.
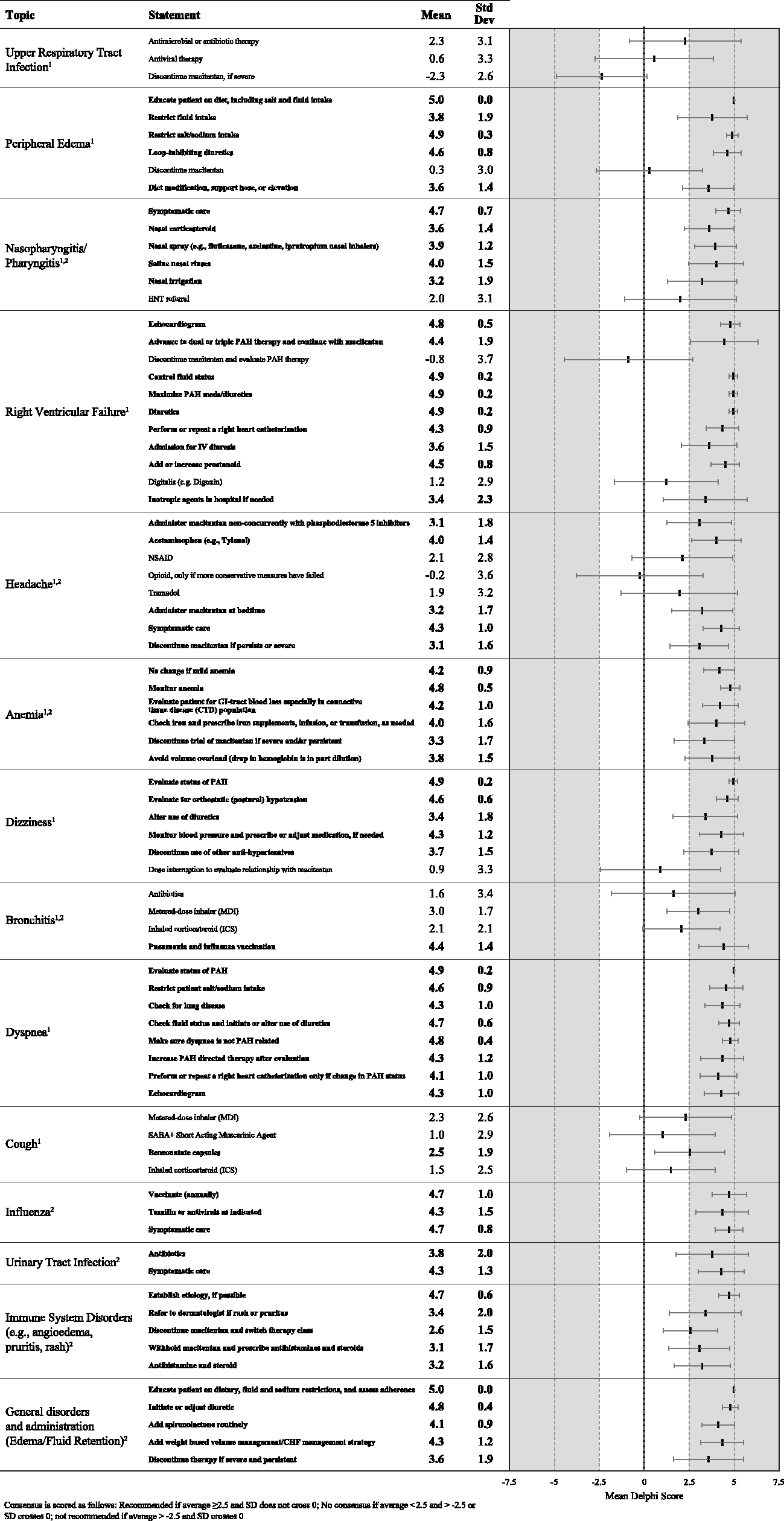
The panelists provided several consensus recommendations for management of common adverse events. See Fig. 8 for the strength of these recommendations.
Upper respiratory tract infections
No consensus recommendations.
Peripheral edema
A patient who develops edema should be educated on diet and advised to restrict fluid and sodium intake. Loop-inhibiting diuretics, spironolactone, compression stockings, and/or elevation are also recommended. Macitentan should be discontinued if severe, persistent edema continues despite these measures.
Nasopharyngitis and pharyngitis
Nasopharyngitis and pharyngitis can be treated symptomatically, including nasal corticosteroids or other nasal sprays, saline rinses, and nasal irrigation.
Right ventricular failure
Management for right ventricular failure should include right heart catheterization (RHC), inotropic agents if needed, and maximization of PAH medications, advancing to dual or triple PAH therapy if possible. In addition, diuretics should be maximized (including IV diuretics) and fluid status controlled. There was no consensus on whether macitentan should be stopped in patients with right ventricular failure.
Headache
Headache can be minimized by administering macitentan at bedtime and not concurrently with PDE5-i. Acetaminophen and symptomatic care are acceptable to manage patient discomfort.
Anemia
Patients with anemia should be monitored, should receive iron replacement as needed, and should avoid volume overload. No change in macitentan therapy is needed for mild anemia, but severe and/or persistent anemia without identifiable cause may require discontinuation of macitentan.
Dizziness
Patients who develop dizziness should be evaluated for the status of their PAH and for postural hypotension, and may need adjustment or discontinuation of diuretics (fluid management) and/or antihypertensive medications.
Bronchitis
Use of a metered-dose inhaler and pneumonia and influenza vaccinations are recommended for patients who develop bronchitis.
Dyspnea
Patients who develop dyspnea should receive an echocardiogram and should be evaluated for fluid status and lung disease, including an assessment of whether the dyspnea is related to PAH. These patients should restrict their sodium intake and may need to alter the use of diuretics and/or their PAH-directed therapy. RHC is warranted if a patient’s PAH status has changed.
Cough
Benzonatate capsules are suggested for managing cough, though other antitussives can be considered.
Infectious disease (influenza and urinary tract infection)
Common infections may be managed with symptomatic care and appropriate anti-infective agents, e.g. oseltamivir or other antivirals for influenza and antibiotics for urinary tract infections. Patients should receive influenza vaccinations annually. For patients who develop influenza, symptomatic care with Tamiflu and/or antivirals are recommended.
Immune/Allergic disorders
If immune system disorders develop (e.g. allergic reaction or angioedema, pruritus, or rash), it is important to establish the etiology. Patients with rash or pruritus should be referred to a dermatologist. If appropriate, macitentan should be discontinued and/or therapy with antihistamines and steroids initiated.
General disorders and administration (edema/fluid retention)
It is critical to educate the patient on dietary, fluid, and sodium restrictions and to assess adherence to these recommendations. In addition, a diuretic should be initiated or, if the patient is already on a diuretic, the diuretic regimen should be adjusted as needed. Spironolactone should be added routinely and volume should be managed using a weight-based strategy like that used with congestive heart failure (CHF). If edema or fluid retention is severe and persistent, consider discontinuing macitentan.
Discussion
This report is intended to assist physicians who use macitentan in managing patients with PAH by providing expert guidance for aspects of care relating to treatment-related adverse events and interruptions in therapy for which little or no real-world evidence-based data are available. The consensus recommendations presented here were developed by a panel of physicians experienced with macitentan and PAH using a modified Delphi methodology. The Delphi process developed a total of 118 statements and the panel reached consensus on 89 of those statements.
The panelists reached a strong consensus on several recommendations. Macitentan is appropriate as a part of dual or combination therapy with PDE5-i or prostanoids for patients in FC II–IV. Short interruptions in macitentan therapy can usually be tolerated, but longer interruptions should be managed by restarting macitentan or some other PAH therapy.
Panelists made several strong consensus recommendations related to adverse event management. Notably, panelists unanimously and strongly agreed on the importance of educating and counseling patients on diet, fluid, and sodium restrictions and the importance of adherence. Appropriate, effective education and counseling can often help control fluid status and thereby prevent or alleviate common events such as edema and dyspnea. Optimization of the patient’s diuretic regimen to control fluid status is also critical for managing these adverse events. In patients who develop right ventricular failure, medications directed at PAH should be maximized, possibly by adding or increasing a prostanoid, in addition to other measures aimed at controlling fluid status (optimization of diuretics). These patients should also be evaluated by echocardiogram.
Other strong recommendations focused on anemia and infectious disease. Patients should be monitored for anemia and treated as appropriate to help keep them on therapy. However, macitentan should be discontinued if anemia is severe and/or persistent and without identifiable, treatable etiology. All patients should receive pneumonia and influenza vaccinations.
The Delphi method is a broadly accepted strategy for developing consensus recommendations based on expert opinion. A key strength of the Delphi method is its use of a systematic, anonymous process that promotes free sharing of opinions and ideas, weights all panelists’ opinions equally, and makes it difficult for any individual panelist to dominate the process.
For this study, the Delphi method was implemented using electronic communications to collect and disseminate information. A clear advantage of this approach is that use of electronic communications minimizes any need for travel or fixed time commitments; therefore, it facilitates panelists’ participation in the process at low cost while respecting their other important time commitments. Use of electronic communications also helps maintain the anonymous nature of the Delphi process.
Limitations
The Delphi process has several limitations. There is currently no generally accepted criterion defining consensus in Delphi studies, and given the wide variety of topics investigated using the Delphi approach, it may not be possible to define generally applicable criteria.6,7,18 As expected for a process intended to provide guidance when no strong evidence is available, the process is not scientifically or statistically rigorous, and even if consensus is reached, there is no guarantee that the consensus answer is correct.7,9,18
Panel selection and the development of the initial questionnaire may have inadvertently introduced bias into the process.6,13 In this study, the selection of expert panelists was limited to ≤20 US-based participants to help ensure that the Delphi process was manageable. Although the panel as a whole has broad and deep experience with PAH and with macitentan, panelists outside of the US were not included. As a result, the Delphi consensus may not represent perspectives from outside the US. In addition, it may have missed important perspectives from a larger population of US-based physicians due to the small sample size. Other potential stakeholders, such as patients, pharmacists, and payers, were also not included.
Although anonymity is an important aspect of the Delphi process, it means that panelists are not accountable for their responses, possibly leading to responses based on insufficient or minimal consideration. 18 The panelists had a wide range of experience within 200 + PAH patient criterion. Panelists less experienced in the disease area in question may have a voice disproportionate to their knowledge of the disease, so that less experienced panelists can vote against and effectively discount tried-and-tested strategies proposed by more experienced panelists. This issue is unlikely to have been significant in this study because the panelists were selected for their experience with macitentan and PAH, and inclusion of panelists with differing levels of expertise related to the study will have helped ensure the manuscript captures the full range of opinions. 13
In conclusion, we used the Delphi process to develop expert consensus recommendations on the use of macitentan in managing patients with PAH. The recommendations are intended to provide practical guidance on clinical questions related to but not fully covered in the package insert and pivotal trial reports for macitentan.
Footnotes
Acknowledgements
Editorial assistance was provided by AXON Communications and funded by an independent grant provided by Actelion Pharmaceuticals US, Inc.
Conflict of interest
All authors had access to the Delphi questionnaire analysis and data and participated in the review, revision, and approval of the content of the manuscript for submission. Eight authors were SERAPHIN investigators and their institutions received funds for patient enrollment in the trial. FFR received support for the design and conduct of this study through an independent grant from Actelion Pharmaceuticals US, Inc. and is a consultant, speaker, and has received research funding from Actelion Pharmaceuticals US, Inc., Gilead Sciences, Inc., Lung Biotechnology, United Therapeutics Corporation, Bayer Corporation, and research funding from Bellerophon Therapeutics, Ikaria, Inc., and Eiger BioPharmaceuticals. HMA receives research funding from Actelion Pharmaceuticals US, Inc. and United Therapeutics Corporation and has served as an Advisory Board Member for Actelion Pharmaceuticals US, Inc., Gilead Sciences, Inc., and United Therapeutics Corporation. RLAA receives research funding from Actelion Pharmaceuticals US, Inc., Bayer Corporation, and United Therapeutics Corporation and has served as an Advisory Board member for Bayer Corporation. VPB receives research funding from United Therapeutics Corporation and serves as an Advisory Board member for Bayer Corporation, Gilead Sciences, Inc., United Therapeutics Corporation, and Actelion Pharmaceuticals US, Inc. RCB has received research support and served as a consultant for Actelion Pharmaceuticals US, Inc., Gilead Sciences, Inc., United Therapeutics Corporation, Bellerophon Therapeutics, Medtronic, and St. Jude’s and has served on Speaker Bureaus for Gilead Sciences, Inc., and St. Jude’s. CDB has received research grant support from Actelion Pharmaceuticals US, Inc., Gilead Sciences, Inc., and United Therapeutics Corporation for multi-center pharmacological studies. In addition, CDB has served as a consultant or Advisory Board member for Actelion Pharmaceuticals US, Inc. and Gilead Sciences, Inc. JB has served on Speaker Bureaus and Advisory Boards for Actelion Pharmaceuticals US, Inc. and Bayer Corporation. CGC has served as an Advisory Board member for Actelion Pharmaceuticals US, Inc., United Therapeutics Corporation, and Gilead Sciences, Inc. MMC has received research support from Actelion Pharmaceuticals US, Inc., Gilead Sciences, Inc., Medtronic, Reata Pharmaceuticals, Inc., Eiger BioPharmaceuticals, Inc, GeNO LLC, and GlaxoSmithKline plc, consulting fees from Actelion Pharmaceuticals US, Inc., Gilead Sciences, Inc., United Therapeutics Corporation, WebMD LLC (Medscape), SteadyMed Therapeutics, Inc., and Express Scripts Holding Company, and honoraria for speaking for Gilead Sciences, Inc. and Bayer Corporation. BPD was the principal site investigator at LSU Health Sciences Center for the SERAPHIN Trial that resulted in FDA registration of macitentan. LSU has received research support from Actelion Pharmaceuticals US, Inc., Gilead Sciences, Inc., and Bayer Corporation. MSE has received research support from United Therapeutics Corporation and Actelion Pharmaceuticals US, Inc., and participates in Speakers Bureaus for United Therapeutics Corporation, Gilead Sciences, Inc., and Actelion Pharmaceuticals US, Inc. PE has received research support from United Therapeutics Corporation and Actelion Pharmaceuticals US, Inc., and has served on Speakers Bureaus and Advisory Boards sponsored by Actelion Pharmaceuticals US, Inc. JF has served as a consultant and on Advisory Boards for Actelion Pharmaceuticals US, Inc., and as a consultant and on Speaker Bureaus and Advisory Boards for Gilead Sciences, Inc., United Therapeutics Corporation, and Bayer Corporation. JWM has received research support from Actelion Pharmaceuticals US, Inc., and has served as a consultant and Speaker Bureau member for Actelion Pharmaceuticals, Inc. and Bayer Corporation, and as a consultant for Reata Pharmaceuticals, Inc. and United Therapeutics Corporation. MP has served as a consultant and Advisory Board member for Actelion Pharmaceuticals US, Inc., Bayer Corporation, Gilead Sciences, Inc., and United Therapeutics Corporation. JSS has received research support from Actelion Pharmaceuticals US, Inc.and has served as a consultant and on Advisory Boards and Speaker Bureaus for Actelion Pharmaceuticals US, Inc. NS has received honoraria from Bayer Corporation, Gilead Sciences, Inc., and United Therapeutics Corporation for consulting and has received research support from Actelion Pharmaceuticals US, Inc, Bayer Corporation, Gilead Sciences, Inc., Bellerophon BioPharmaceuticals, Arena Pharmaceuticals, Inc., and United Therapeutics Corporation. HIP has served on scientific advisory boards for Actelion Pharmaceuticals US, Inc, Bayer Corporation, GlaxoSmithKline plc, Janssen Pharmaceuticals, Inc., and United Therapeutics Corporation, and currently serves on a Data and Safety Monitoring Board for Eiger BioPharmaceuticals, Inc.
Funding
Please see the declaration of conflicting interests for funding details.