
Abstract
Many therapeutic options are available for patients with pulmonary arterial hypertension (PAH). However, little is known about the effects of sequential combination therapy on exercise capacity. Here we monitored exercise capacity by cardiopulmonary exercise testing (CPX) and observed the benefit of using a peak VO2 cutoff of 15 mL/kg/min to guide combination therapy. Thirty patients newly diagnosed with PAH were treated with goal-oriented sequential combination therapy. Endothelin receptor antagonists (ERA) were the first-line treatment, with phosphodiesterase type 5 inhibitors (PDE-5i) as the preferred combination partner. The patients underwent cardiac catheterization at baseline and after 12 months and CPX at baseline and after three, six, and 12 months. Circulatory power (CP) was defined as the product of peak O2 uptake and peak systolic blood pressure (SBP); ventilatory power (VP) was defined as peak SBP divided by the minute ventilation–CO2 production slope. After 12 months, ERA had been administered to 100% of the study patients and PDE-5i to 82%. Mean CP at baseline and after three, six, and 12 months was 1807, 2063, 2248, and 2245 mmHg·min/mL/kg, respectively, and mean VP was 2.93, 3.53, 4.16, and 3.68 mmHg, respectively. CP was greater after 6 months than at baseline (P = 0.047); VP was greater after three months than at baseline (P = 0.019) and further improved at six months compared with three months (P = 0.040). Therefore, repeated CPX assessment, including measurement of CP and VP, can provide useful information regarding the efficacy of goal-oriented treatment for PAH.
Pulmonary arterial hypertension (PAH) is a life-threatening disease that is associated with poor prognosis. 1 Many potential therapeutic options are now available for patients with PAH, 2 including three recently approved classes of drugs: prostanoids; endothelin receptor antagonists (ERA); and phosphodiesterase type 5 inhibitors (PDE-5i). 3 In particular, the ERA bosentan4,5 and ambrisentan6,7 and the PDE-5i sildenafil8,9 and tadalafil 10 are used widely to treat PAH. Current treatment algorithms11,12 recommend an ERA or PDE-5i as a first-line treatment for PAH of functional class II or III beginning at a relatively early stage of disease. Compared with monotherapy, combination therapy improved exercise capacity and reduced the risk of clinical disease progression in patients with PAH.13,14 However, the optimal strategy regarding the implementation of combination therapy has not yet been determined.
Recognition of the potential value of cardiopulmonary exercise testing (CPX) in patients with PAH is increasing.14–16 However, little is known about how exercise capacity changes over time under “goal-oriented” sequential combination therapy in patients newly diagnosed with PAH. Hoeper et al. 14 proposed goal-oriented treatment for PAH patients in response to results from CPX and six-minute walk distance (6MWD). However, these treatment goals might be suboptimal. For example, the most recent treatment guideline for PAH advocates that a peak oxygen uptake (VO2) cutoff value of ≥15 mL/min/kg is a better indicator of prognosis. 11 In addition, an improvement in 6MWD often does not reflect benefit in clinical outcomes in patients with PAH. 17
In the present study, we observed the therapeutic effect of goal-oriented therapy evaluated by using CPX. In addition, we focused on relatively new indices, namely circulatory power (CP) and ventilatory power (VP), in the CPX of PAH patients. The aim of this study was to use a peak VO2 cutoff of 15 mL/kg/min to guide combination therapy and observe exercise capacity over time by monitoring the results of CPX in patients with PAH.
Materials and methods
Study design and population
The study was conducted prospectively at Nagoya University Hospital, Japan, from October 2012 through March 2015. Eligible patients were aged 16–80 years at study entry and had newly diagnosed PAH of World Health Organization (WHO)-functional class (FC) II to IV according to the Dana point criteria. 18 Patients who had WHO-FC IV disease with hemodynamic instability were immediately treated with intravenous epoprostenol if needed.
Patients with any of the following conditions at enrollment were excluded: (1) pulmonary hypertension corresponding to group 2, 3, 4, or 5 according to the Dana point classification or congenital heart disease; (2) pregnancy; (3) serum creatinine >2.0 mg/dL; (4) history of serious chronic obstructive pulmonary disease or restrictive lung disease (forced expiratory volume in 1 s/ forced vital capacity ratio <70%; vital capacity <80% of predicted); (5) unable to walk without personal assistance; (6) currently receiving PAH-targeted therapy, such as ERA, PDE-5i, or intravenous epoprostenol; or (7) other conditions that, according to the judgement of the physicians in charge, made enrollment inappropriate because of concerns regarding patient safety.
Study procedures and medication protocol
The study protocol included cardiac catheterization at baseline and after 12 months of therapy and CPX at baseline and after three, six, and 12 months (Fig. 1). The treatment goal was a peak VO2 > 15.0 mL/min/kg, which is defined as a “better prognosis” according to 2009 European Society of Cardiology and the European Respiratory Society guideline.
11
An ERA, either bosentan or ambrisentan, was used as a first-line treatment. The second step was a PDE-5i, sildenafil or tadalafil, followed by the addition of intravenous epoprostenol if needed. Other drugs including beraprost, diuretics, digitalis, and anticoagulation were excluded from this combination treatment protocol. Physicians expert in treating PAH determined the optimal pharmacological therapy for each patient.
Study protocol. ERA, endothelin receptor antagonists; PDE-5i, phosphodiesterase-5 inhibitors; CPX, cardiopulmonary exercise testing; Cath, cardiac catheterization.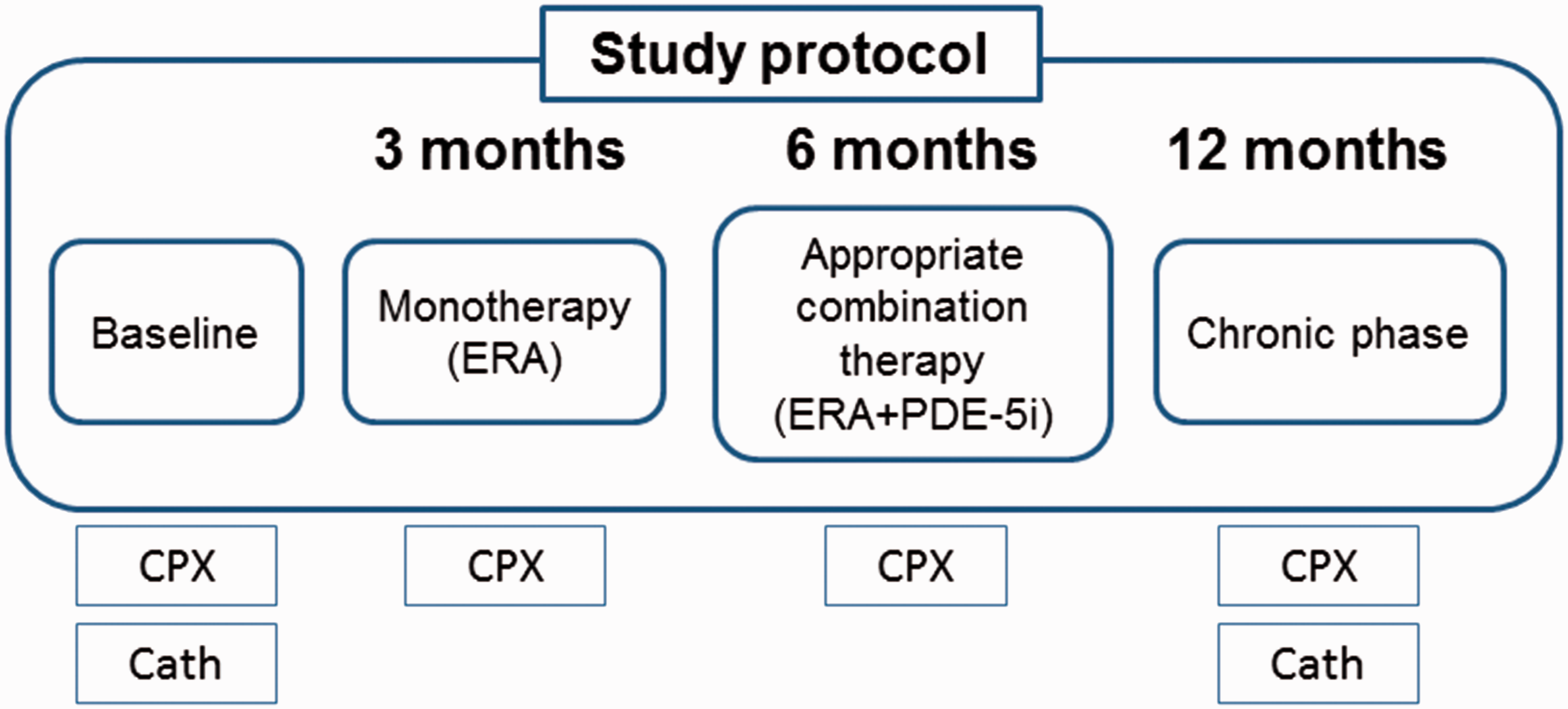
Dosing regimens
Bosentan was given at an initial dose of 62.5 mg twice daily for four weeks, which was titrated to 125 mg twice daily thereafter. Ambrisentan was started at 5 mg once daily for four weeks and increased gradually to 10 mg once daily thereafter in the absence of side effects and with adequate tolerability. Sildenafil was titrated to a maximum of 20 mg three times daily. Tadalafil was started and maintained at 40 mg once daily. Given the individual variability in responses, the choice of the drug and dose to be used in individual cases was left to the discretion of the physician. All drug regimens were adjusted as necessary to limit side effects. Patients were always informed about all available treatment options; whenever combination treatment was proposed, patients were informed regarding potential risks and side effects.
Informed consent
The study protocol was approved by the Ethics Review Board of Nagoya University School of Medicine (no. 1157). All participants provided their written informed consent after a physician-in-charge explained the study objectives, study protocol, possible adverse effects of the study drugs, measures for privacy protection, and procedures for study withdrawal.
Exercise capacity
Each patient underwent CPX at a progressively increasing work rate to maximal tolerance on a cycle ergometer. Oxygen and CO2 sensors were calibrated before each test by using gases with known O2, N2, and CO2 concentrations. In addition, the flow sensor was calibrated before each test. All patients started at 10 W for a 3-min warm-up, followed by a 10 -W/min ramp increment protocol. The 12-lead electrocardiogram was monitored continuously, and the arm blood pressure was automatically measured every minute during exercise and throughout the recovery period. After achieving the peak workload, all patients pedaled at a load of 0 W for a cool-down period of at least 2 min, to prevent excess venous pooling. The test termination criterion was either patient request, volitional fatigue, ventricular tachycardia, ≥2 mm of horizontal or down-sloping ST segment depression, or a drop in systolic blood pressure (SBP) of ≥20 mmHg during exercise. A qualified exercise physiologist conducted each test, under supervision by a certified cardiologist. Respiratory gas-exchange variables, including VO2, CO2 output (VCO2), and minute ventilation (VE), were acquired continuously throughout CPX testing by using an Ergospirometry Oxycon Pro (Carefusion Germany, Höchberg, Germany), and the gas-exchange data were obtained breath by breath. The peak VO2 and peak respiratory exchange ratio were defined as the highest 30-s average values obtained during the last stage of CPX. The VE/VCO2 slope was determined by using linear-regression analysis of the VE and VCO2 values obtained up to the respiratory compensation point during exercise. CP was defined as the product of peak VO2 and peak SBP. VP was defined as peak SBP divided by the VE/VCO2 slope.
Statistical analysis
All data are expressed as mean ± 1 SD. To evaluate the effect of sequential combination therapy for PAH, hemodynamic parameters at baseline and those after 12 months were compared by using paired t-tests for all patients except the two who died during the study. Repeated-measures analysis of variance was used to assess the change in parameters over time in all patients except the two who died during the study. All statistical analyses were performed by using the SPSS 17.0 software package (SPSS, Chicago, IL, USA). A P value < 0.05 was considered statistically significant.
Results
Patient characteristics at baseline.
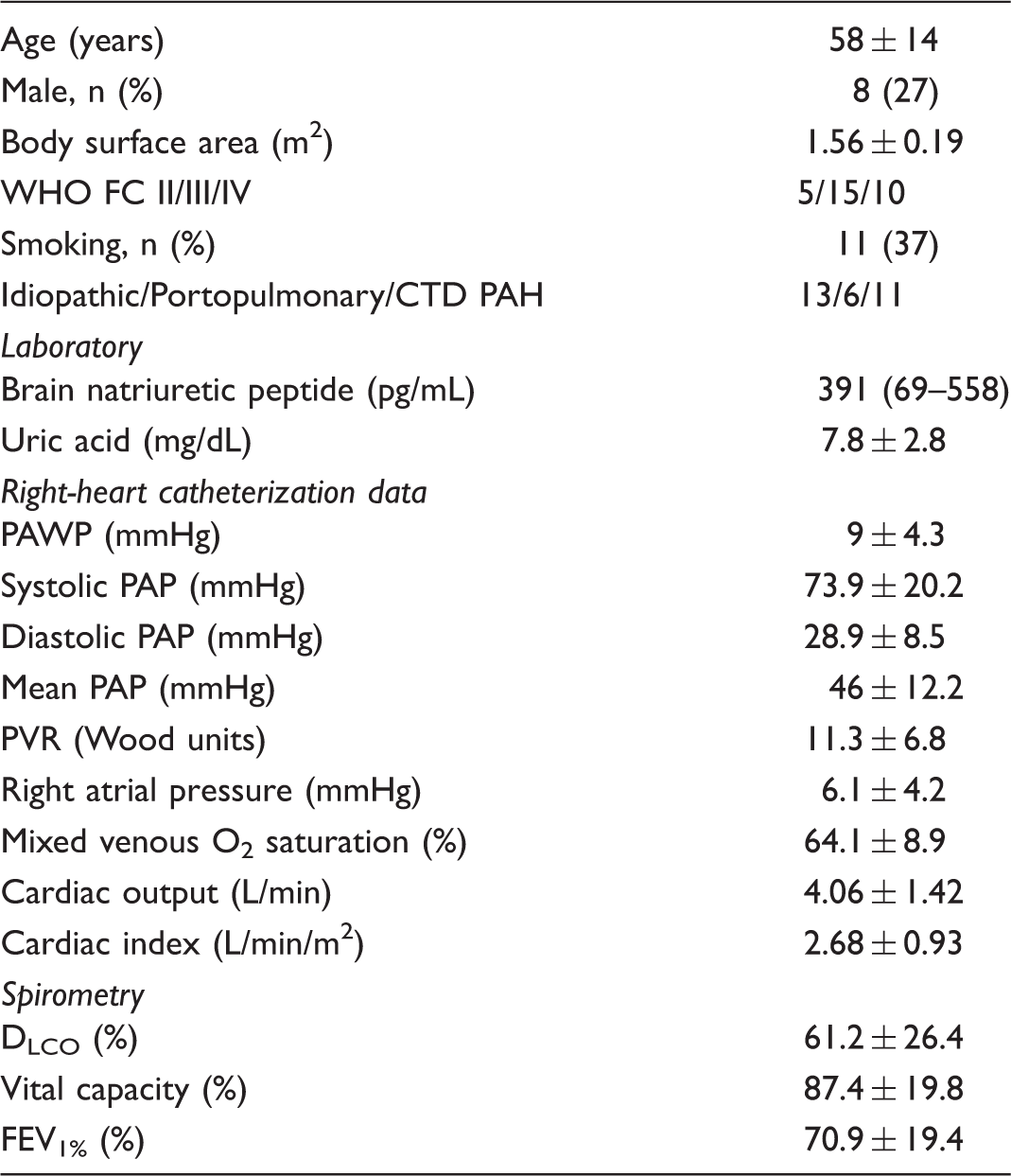
CTD, connective tissue disease; DLCO, diffusing capacity for carbon monoxide; FEV1%, forced expiratory volume in 1 s relative to vital capacity; PAH, pulmonary arterial hypertension; PAP, pulmonary arterial pressure; WHO, World Health Organization; PAWP, pulmonary arterial wedge pressure; PVR, pulmonary vascular resistance. Data are presented as mean ± 1 SD or median (interquartile range).
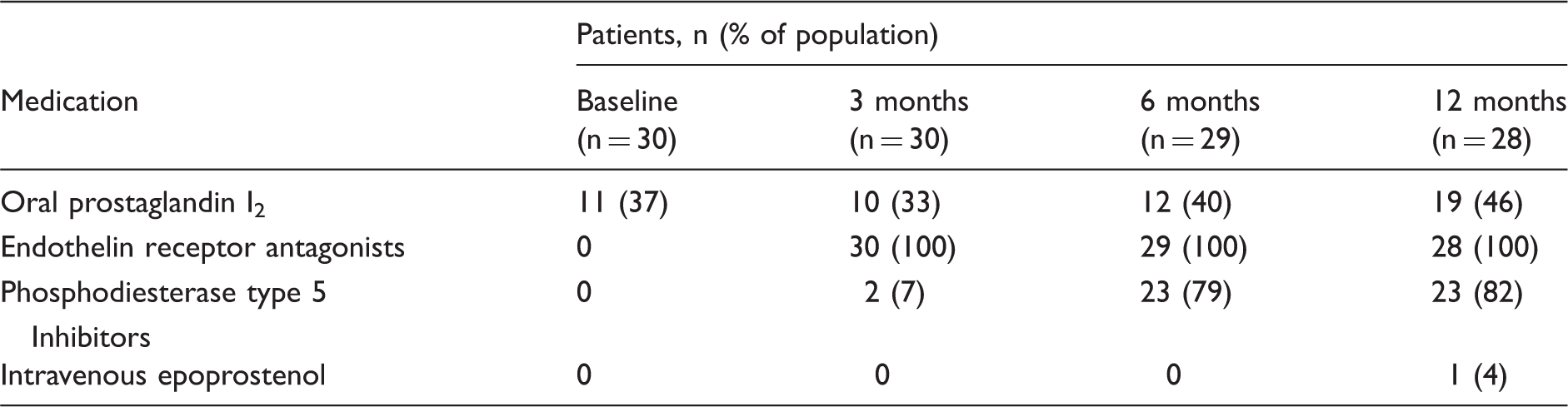
Drugs used to treat pulmonary arterial hypertension.
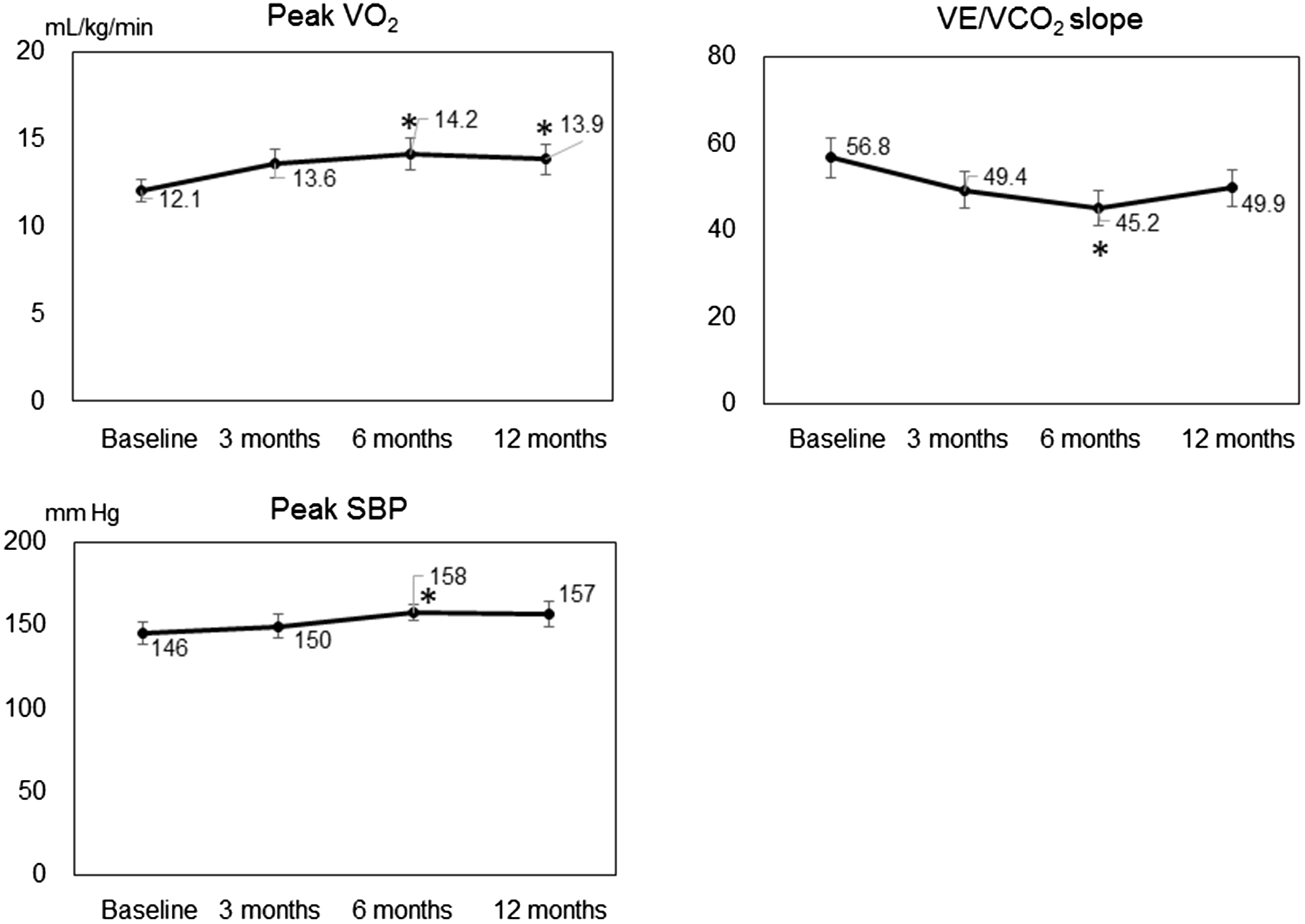
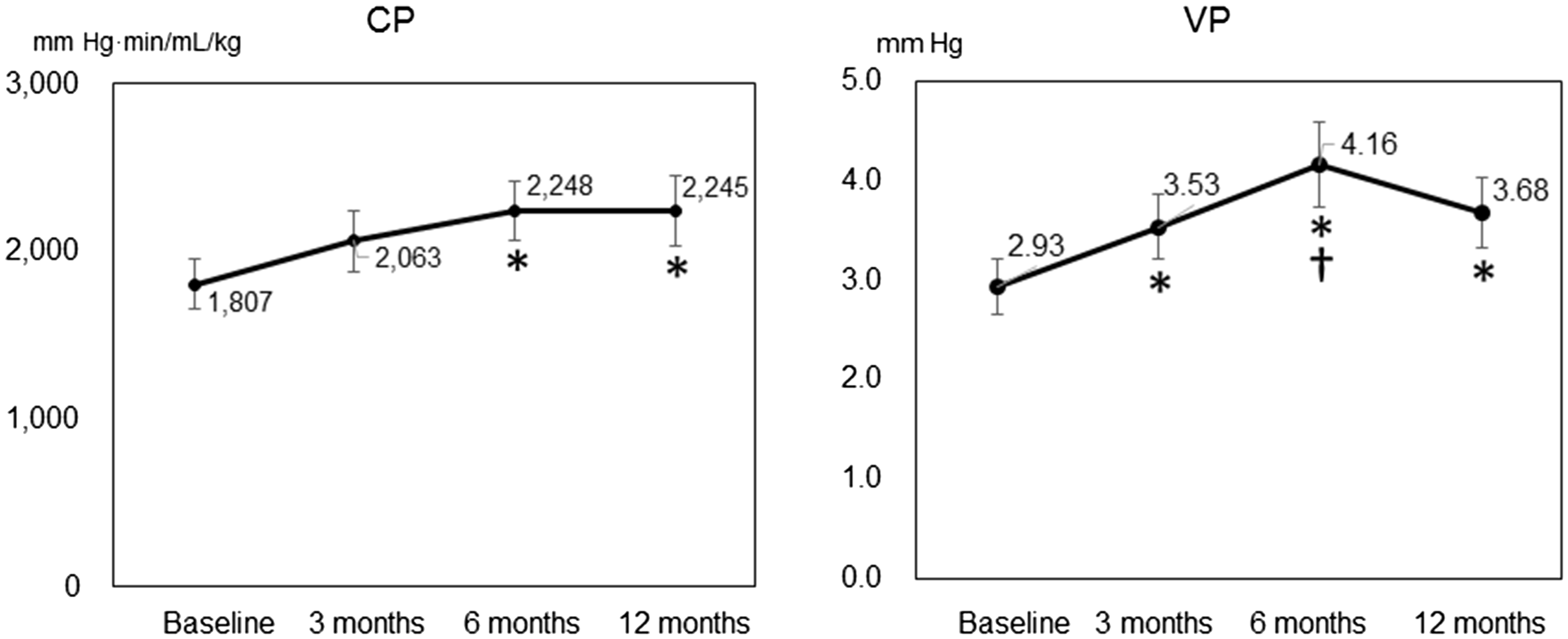
Both mean pulmonary arterial pressure (mPAP) and pulmonary vascular resistance (PVR) were decreased after 12 months compared with baseline values; the two patients who died during the study were excluded from this analysis (Fig. 2). Compared with baseline values, peak VO2 and peak SBP were higher and VE/VCO2 slope was lower after six months, but the three-, six-, and 12-month data for these parameters did not differ from each other (Fig. 3). At baseline and at three, six, and 12 months after initiation of PAH-specific treatment, mean CP was 1807, 2063, 2248, and 2245 mmHg·min/mL/kg, respectively, and mean VP was 2.93, 3.53, 4.16, and 3.68 mmHg, respectively (Fig. 4). CP was greater after six months of combined PAH-targeted therapy than at baseline (P = 0.047). In addition, VP was greater after three months of treatment than at baseline (P = 0.019) and greater still at six months compared with three months (P = 0.040).
Hemodynamic parameters at rest in patients with pulmonary arterial hypertension. mPAP, mean pulmonary arterial pressure; PVR, pulmonary vascular resistance. Changes in exercise capacity over time in patients receiving sequential combination therapy for pulmonary arterial hypertension. VE/VCO2, minute ventilation/peak CO2 output; Peak VO2, peak O2 uptake; SBP, systolic blood pressure. *P < 0.05 vs. baseline. Changes in circulatory power (CP) and ventilatory power (VP) over time in patients receiving sequential combination therapy for pulmonary arterial hypertension. *P < 0.05 vs. baseline, †P < 0.05 vs. three months.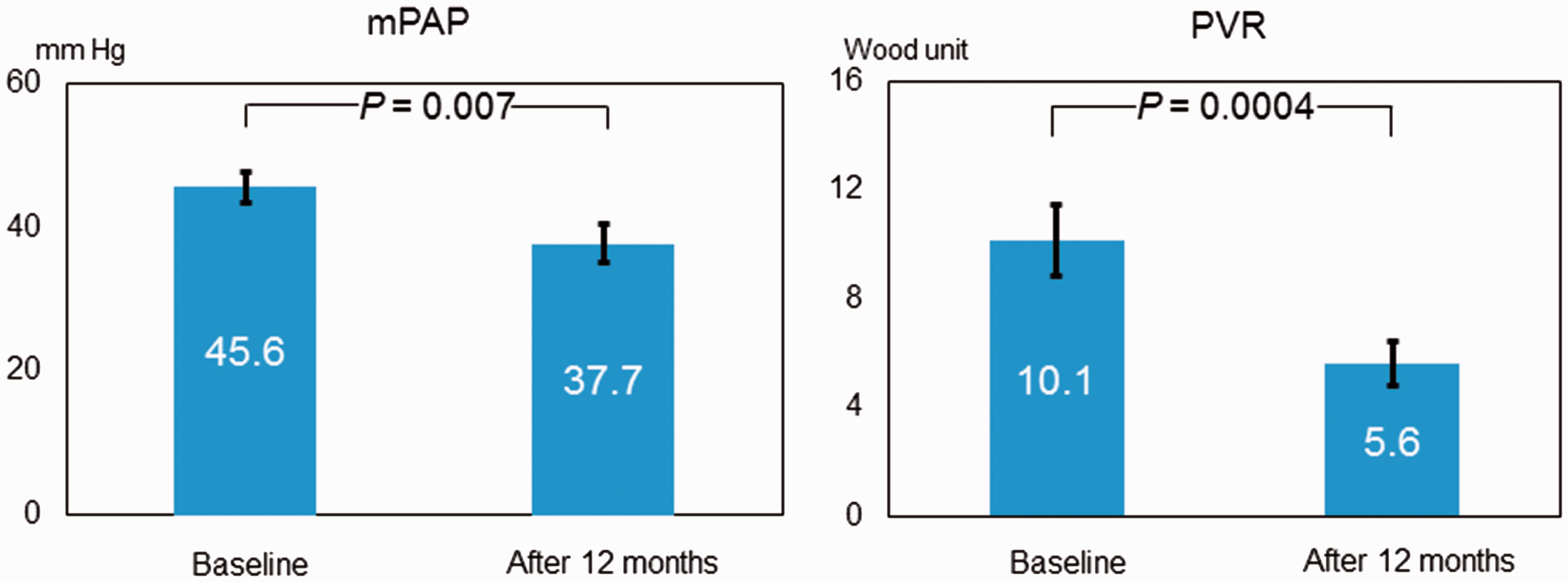
Discussion
In our patients newly diagnosed with PAH, both CP and VP progressively improved due to sequential combination therapy that was revised according to patients’ exercise capacity. We therefore believe that CPX assessment can provide useful information regarding the effects of therapeutic regimens in patients with PAH.
This study aimed to observe exercise capacity over time by monitoring the results of CPX in patients with PAH. Most investigations of PAH have focused on hemodynamic parameters or on cardiac function by using data from cardiac catheterization in resting patients. However, these assessments are impractical for monitoring therapeutic effect repeatedly. In fact, a low peak VO2 was an independent predictor of poor prognosis in patients with PAH.19,20 In the current study, however, we incorporated CPX-guided therapeutic decisions due to the noninvasive accessibility and prognostic importance of the available parameters.
At the start of the present study, beraprost had already been used in 37% of these participants. This drug is the first chemically stable and orally active prostacyclin analog for PAH,21,22 but its effects subside after half a year of use.23,24 Beraprost is approved in Japan and South Korea for the treatment of PAH, but worldwide, the evidence level for beraprost as a medication for PAH is decreased. Because hemodynamic parameters at baseline did not differ significantly between PAH patients who took beraprost and those who did not (data not shown), we excluded it for goal-oriented sequential combination therapy in the current study.
Although PAH-expert physicians ultimately determined the optimal pharmacological therapy for each patient in the current study, in principle, an ERA, such as bosentan or ambrisentan, was used as the first-line treatment; a PDE-5i, such as sildenafil or tadalafil, and other drugs then were added when the current therapy was not sufficiently effective. Treatment goals were set and therapeutic decisions were made according to the established prognostic criterion of a peak O2 > 15.0 mL/min/kg during CPX. During the 12-month observation period, only one patient required intravenous epoprostenol (after six months). In addition, except for two patients with systemic scleroderma-associated PAH who died due to progression of their collagen-tissue disease, all patients were treated according to the present protocol for 12 months. Ultimately, 23 of the remaining patients received combination therapy with ERA and PDE-5i; the proportion of patients treated with PDE-5i was 79% at six months and increased to 82% at 12 months. The five patients who received ERA only improved to WHO-FC I or II and remained clinically stable without cardiac events; PDE-5i were contraindicated in one of these patients because she took amiodarone for treatment of a non-sustained ventricular tachycardia. The average peak VO2 among the ERA-only patients increased from 12.5 mL/kg/min at baseline to 17.4 mL/kg/min after 12 months, and their mPAP decreased from 42.5 mmHg at baseline to 27.7 mmHg after 12 months. We believe that, in this subgroup of PAH patients, monotherapy was appropriate for at least 12 months, suggesting that our CPX-guided goal-based treatment strategy might avoid excess medication and cost but still provide appropriate intervention by enabling treatment to be tailored to the individual patient.
Hoeper et al. 14 previously proposed goal-oriented treatment of PAH patients according to results of CPX or 6MWD. In that study, the treatment goals to stratify therapeutic decisions were set according to established prognostic criteria: 6MWD, 380 m; peak VO2, >10.4 mL/min/kg; and peak SBP during exercise, >120 mmHg. This approach yielded one-, two-, and three-year survival rates of 93%, 83%, and 80%, respectively. 14 These results compared favorably with a historical control group of PAH patients treated before 2002 (i.e. before bosentan and sildenafil became available).25,26 However, because of progress in therapeutic options for PAH, these earlier treatment goals might now be suboptimal. In a meta-analysis of 6WMD in patients with PAH, improvement in 6MWD did not reflect benefit in clinical outcomes. 17 Furthermore, the 6MWD measure depends not only on cardiopulmonary fitness but also on other factors, including sex, body weight, and height. 27 In addition, to improve prognosis according to the current European Society of Cardiology and European Respiratory Society guideline, which describes parameters established for assessing PAH severity, stability, and prognosis for PAH, 11 we increased the cutoff value for peak VO2 to > 15 mL/min/kg. Therefore, we particularly targeted peak VO2 as a therapy goal and assessed CPX parameters repeatedly under sequential combination therapy.
Among the parameters available through CPX testing, we particularly focused on changes in CP and VP in the present study. CP (i.e. the product of peak VO2 and arterial pressure) is a powerful prognostic marker in chronic heart failure. 22 In addition, VP was independently predictive of cardiac events compared with the prognostic value of standard CPX indices (i.e. peak VO2 and the VE/VCO2 slope); furthermore, according to multivariate analysis, combining CP and VP provided even better prognosis discrimination. 23 Whereas CP is an index that combines central and peripheral components of cardiac stroke work, VP provides a measure that combines systemic hemodynamics with CO2 production efficiency. Both CP and VP provide important information regarding disease severity and prognosis.28–30 In the present study, only VP was significantly improved after six months of PAH-targeted combined therapy compared with three months. This index might be more sensitive to therapeutic effects than other CPX prognostic parameters in PAH. To our knowledge, no other data are available regarding changes in CP and VP over time in PAH patients receiving sequential combination therapy. In the present study, both CP and VP—like other prognostic CPX parameters—gradually improved due to sequential combination therapy for at least six months. Future work is needed to determine the prognostic utility of CP and VP in patients with PAH.
In the present study, exercise capacity after 12 months was similar to or somewhat poorer (albeit non-significantly) than that at six months. The reason for this result is unclear, but we speculated that not all patients performed the recommended cardiac rehabilitation, no further drugs were added between these time periods, and natural disease progression occurred. One important finding of this study was that, to achieve the predefined treatment goals, combination treatment eventually became necessary in more than 80% of the patients, indicating that monotherapy lacks sufficient efficacy in many patients with PAH. This finding was expected, because none of the currently available treatments are curative, and PAH eventually progresses in many patients despite active therapy. The strategy we followed was based on many factors, including the interval at which to monitor potential side effects of each medication, physician experience, practicability, and economic considerations. However, further studies are needed to define the variables most useful for clinical decision-making and the treatment principles that provide the best long-term results.
Our study has several limitations. First, it was performed in a small number of patients and had a short follow-up period. However, our study population comprised patients newly diagnosed with PAH, and we believe that this characteristic enhances our study’s value. Second, we did not assess any peripheral factors, even though these factors influence exercise capacity. Third, as we suggested above, not all patients complied with cardiac rehabilitation; if all patients had, perhaps exercise capacity might have shown greater improvement.
In conclusion, in our patients with newly diagnosed PAH, sequential combination therapy significantly improved exercise capacity, particularly VP and CP. Sequential combination therapy, therefore, may be a useful treatment option in patients with PAH. In addition, CPX assessment potentially can provide useful information regarding treatment efficacy in PAH.
Footnotes
Acknowledgments
Akihiro Hirashiki used to belong to a department endowed by Actelion Pharmaceuticals Japan, Ltd. Both Takahisa Kondo and Shiro Adachi belong to a department endowed by Actelion Pharmaceuticals Japan, Ltd. We express our sincere appreciation to all the patients, collaborating physicians, and other medical staff for their important contributions to the present study.
Conflict of interest
The author(s) declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.