
Abstract
Aortic stenosis (AS) leads to pulmonary hypertension (PH) and right ventricle (RV) failure. Our goal was to describe mortality related to postoperative complications in PH patients undergoing transcatheter aortic valve replacement (TAVR). Ninety-three TAVR patients were analyzed (controls, sPAP < 50 mmHg; cases, sPAP ≥ 50 mmHg). Significant findings in cases included increased mortality (365 days), post-TAVR atrioventricular block (AVB) and acute kidney injury (AKI), and increased mean length of stay (LOS). This novel study highlights complications of PH as independent risk factors for death and significant morbidity post TAVR. Optimization of preoperative volume status and RV afterload reduction, while addressing AVB and AKI, may play a vital role in reducing mortality and LOS.
Keywords
Introduction
Aortic stenosis (AS) has a known consequence of pulmonary hypertension (PH) and right ventricle (RV) failure. 1 Transcatheter aortic valve replacement (TAVR) has revolutionized treatment of AS by offering a less-invasive option compared to surgical aortic valve replacement (SAVR).2–4 Severity of AS is categorized as mild (Vmax 2–2.9 m/s or mean gradient < 20 mmgHg), moderate (Vmax 3–3.9 m/s or mean gradient 20–39 mmHg), or severe (Vmax ≥ 4.0 m/s or mean gradient ≥ 40 mmHg). 5 Patients who are candidates for AVR include both moderate and severe AS, as recent trials have shown the benefits of the Sapien S3 valve in the moderate AS population.6,7
The Placement of Aortic Transcatheter Valves (PARTNER) trial examined 358 patients with severe AS and compared balloon aortic valvuloplasty and TAVR.2,3 These results showed patients undergoing TAVR had lower mortality rates and improved New York Heart Association (NYHA) functional class. Another cohort of the PARTNER trial compared TAVR to SAVR and results demonstrated earlier symptom relief in the TAVR arm.8,9 Similarly, in the US CoreValve High Risk Study, 795 patients with severe AS were randomly assigned to TAVR and SAVR and results were significant for a reduced mortality rate in the TAVR arm. 10
Establishing definitive therapy for AS is imperative as it can result in left ventricular hypertrophy with consequent dysfunctional lusitropy, leading to pulmonary vascular remodeling and development of Group 2 PH per the World Health Organization (WHO) classification.11–14 The development of PH in this population is primarily the result of elevated left-sided cardiac filling pressures and associated vascular reactive changes. 15 Concurrent PH was seen in a study of 388 AS patients where right heart catheterization (RHC) showed evidence of mild–moderate PH, defined as systolic pulmonary artery pressure (sPAP) in the range of 31–50 mmHg, in 50% of patients and severe PH, defined as sPAP > 50 mmHg, in 15% of patients. 15 Reports have indicated a prevalence of PH in AS patients in the range of 29–50%.16,17 Another investigation showed that nearly 70% of AS patients who are TAVR candidates also had concomitant PH. 18
Prior investigations were able to substantiate that AS patients undergoing AVR had decreased long-term survival though the reasons behind this worsened prognosis were not defined.19,20 Group 2 PH associated with postoperative TAVR complications needs further delineation given increasing utilization of TAVR. The aim of our study is to correlate postoperative complications, including mortality, in AS patients undergoing TAVR according to severity of PH.
Methods
Study design
We conducted a retrospective, post-hoc analysis of 93 consecutive AS patients who underwent TAVR from 2011–2015 at Rush University Medical Center, Chicago, IL, USA. The study was approved by the Institutional Review Board of Rush University Medical Center and the requirement for informed consent was waived. Patients undergoing SAVR were excluded. Primary outcomes evaluated the prospect that PH would predict mortality and length of stay (LOS) rates. Secondary outcomes included evaluation of postoperative complications, including mortality, acute kidney injury (AKI), and new post-procedural atrioventricular block (AVB). AKI was defined by Kidney Disease: Improving Global Outcomes Clinical Practice Guidelines, where creatinine increased by ≥ 0.3 mg/dL within 48 h after surgery or a relative creatinine increase of ≥ 50% from the baseline within seven days after surgery. 21 AVB, in this population, included the development of unstable bradycardia requiring permanent pacemaker placement as well as all degrees of heart block. Patients with a history of pacemaker prior to TAVR were excluded from the AVB outcomes.
Data extraction
Clinical and laboratory data were collected for all patients at various time intervals including pre-procedure, peri-procedure, post-procedure, during the index hospitalization, and up to one year post procedure when available. Collected data included past medical history, laboratory tests, transthoracic echocardiograms (TTE) studies, RHC results, and clinical outcomes including postoperative complications. RHCs were completed at time of TAVR procedure by interventional cardiologists.
Statistical analysis
Baseline characteristics, results of RHC, peri-procedural characteristics, postoperative complications, and LOS between none/mild PH and moderate/severe PH were compared by one-way ANOVA and Fisher’s exact test. A P value of < 0.05 was considered statistically significant. Mortality rates up to 365 days were computed when data were available. Follow-up was noted up to 365 days since TAVR procedure. Additionally, for patients with available data, a linear regression model with LOS (in days) as dependent and pre-TAVR BNP as independent was performed. All data analysis was performed using SPSS statistical software.
Several multiple logistic regression models were performed on post-procedure AKI, post-procedure AVB, and mortality at 120 and 365 days as dependent variables and all the usable clinical variables collected in the study entered as candidate independent variables. For each dependent variable analyzed, candidate predictors were entered stepwise into the model whenever the estimated P value for their associated test F statistic was < 0.05. They were eliminated from the model when the F statistic was > 0.1. Candidate variables were entered in the order of smallest P value first. Odds ratios (OR) were generated and expressed with 95% confidence intervals (CI). A multiple linear regression was also performed on LOS in days against previously identified candidate predictors outliers with two ICU LOS removed (< 3% of the 93 cases) to minimize the impact of outliers on the regression.
Results
A total of 93 patients were included in the study. Patients were divided into two groups based on severity of PH, which was determined by sPAP recorded from RHC during the TAVR. The sPAP was averaged over three respiratory cycles and patient were anesthetized at the time of measurement. Controls were defined as none/mild PH with sPAP < 50 mmHg (n = 50) and cases were defined as moderate/severe PH with sPAP ≥ 50 mmHg (n = 43).19,22
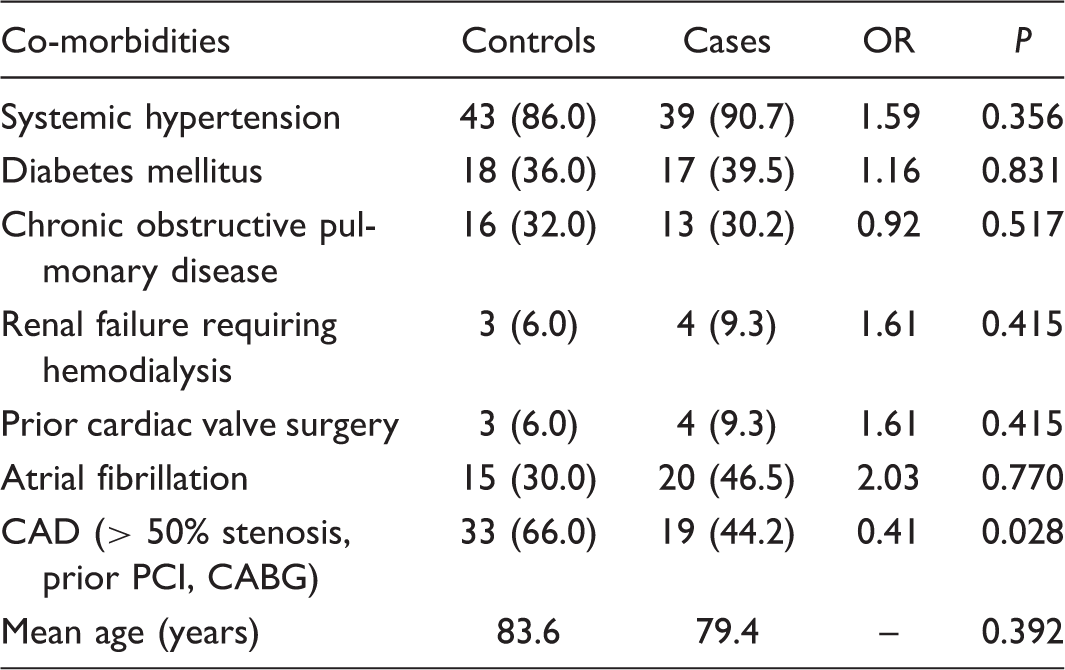
Baseline co-morbidities of controls and cases (n (%)).
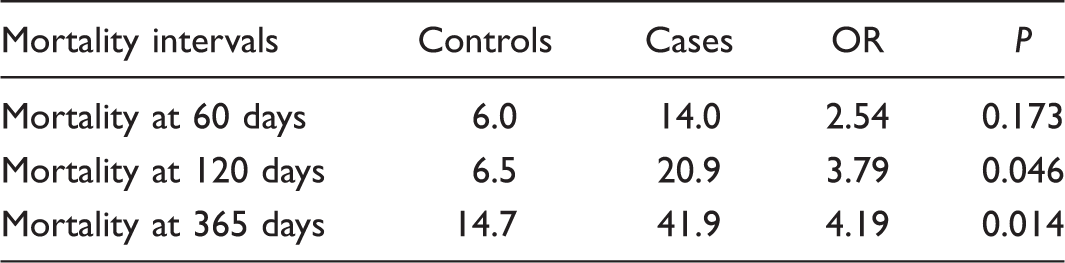
Mortality (%) between controls and cases.
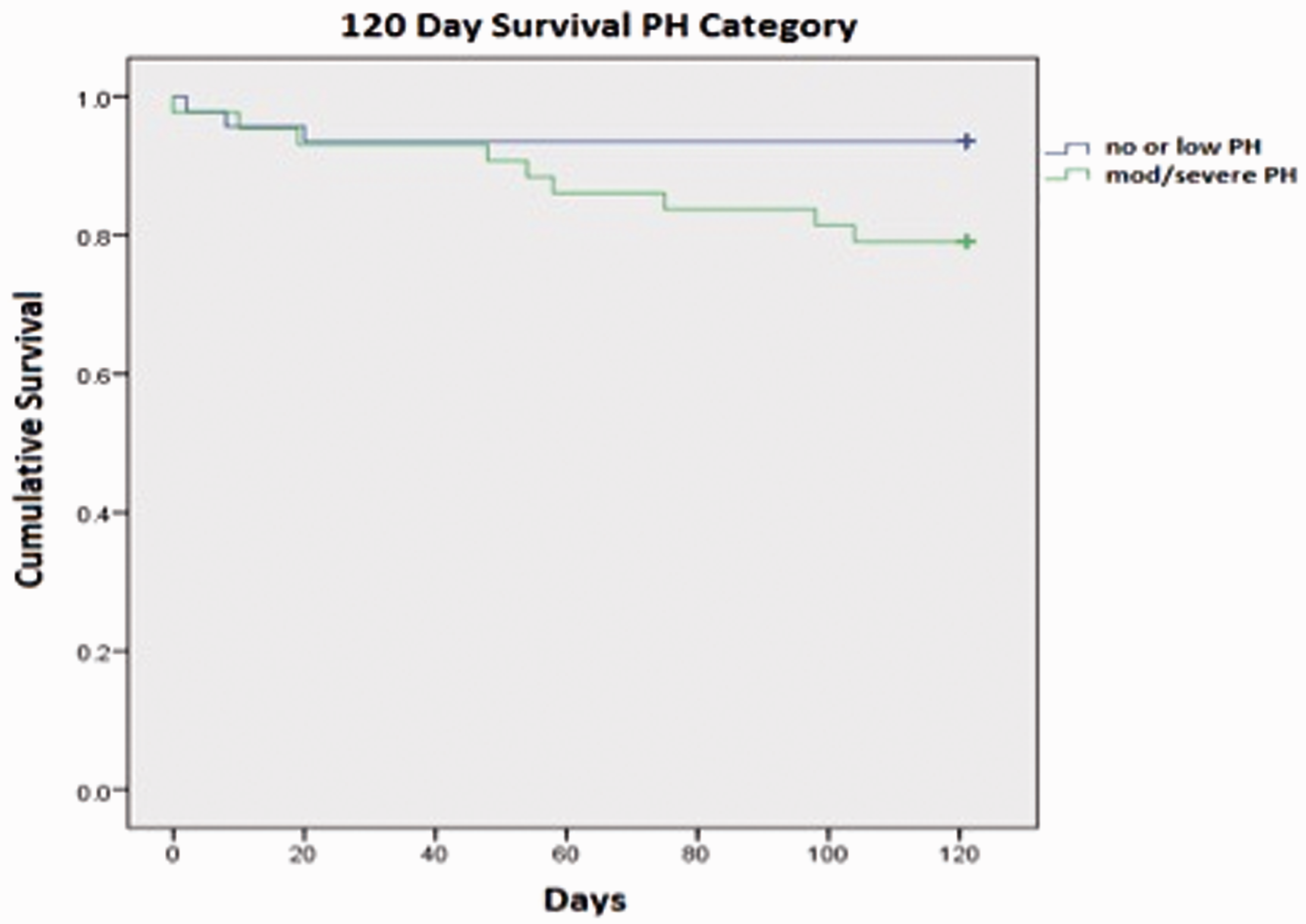
Kaplan–Meier curve for 120-day mortality. Moderate/Severe PH group with increased mortality at 120 days (P = 0.046).
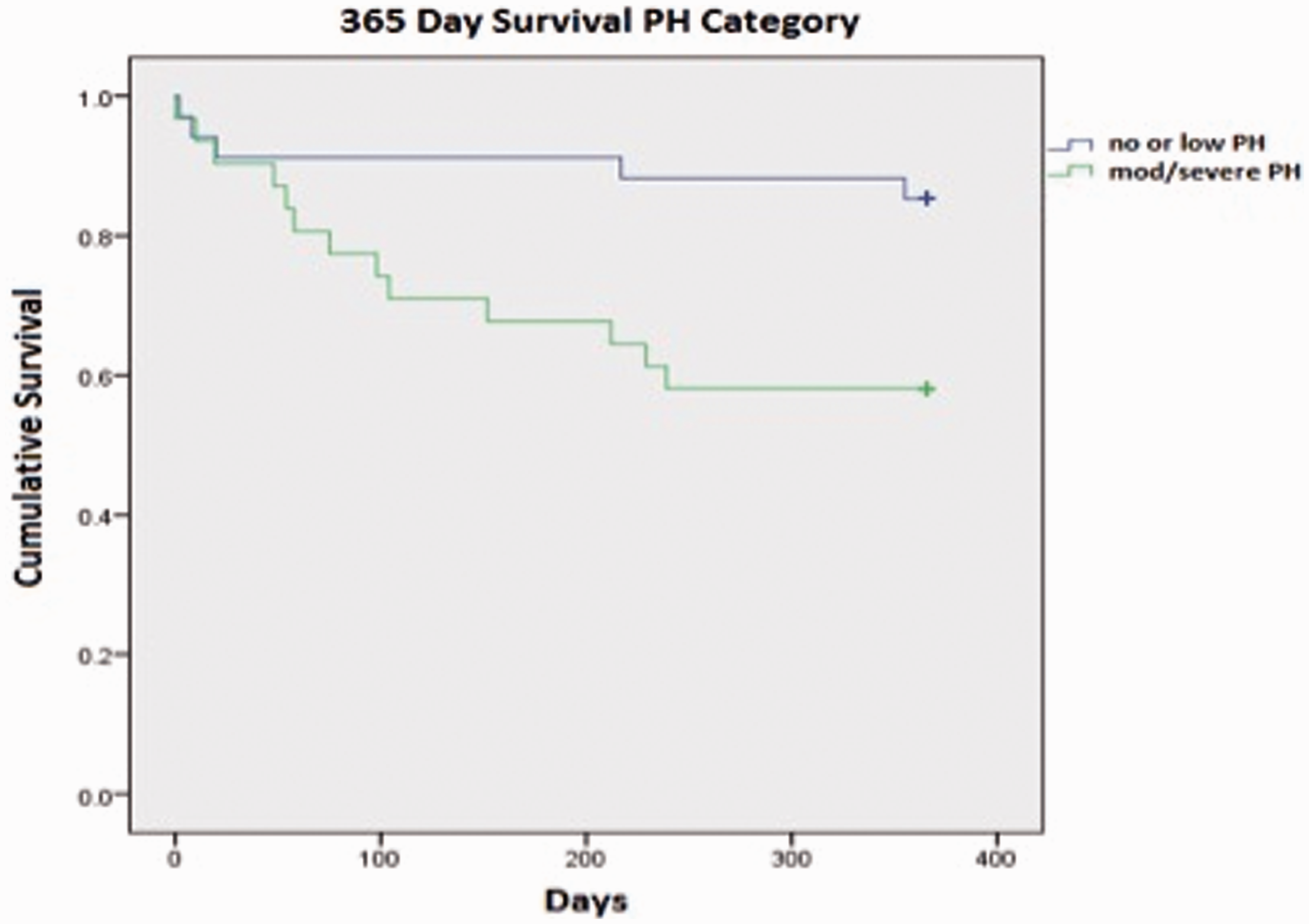
Kaplan–Meier curve for 360-day mortality. Moderate/Severe PH group with increased mortality at 365 days (P = 0.014).
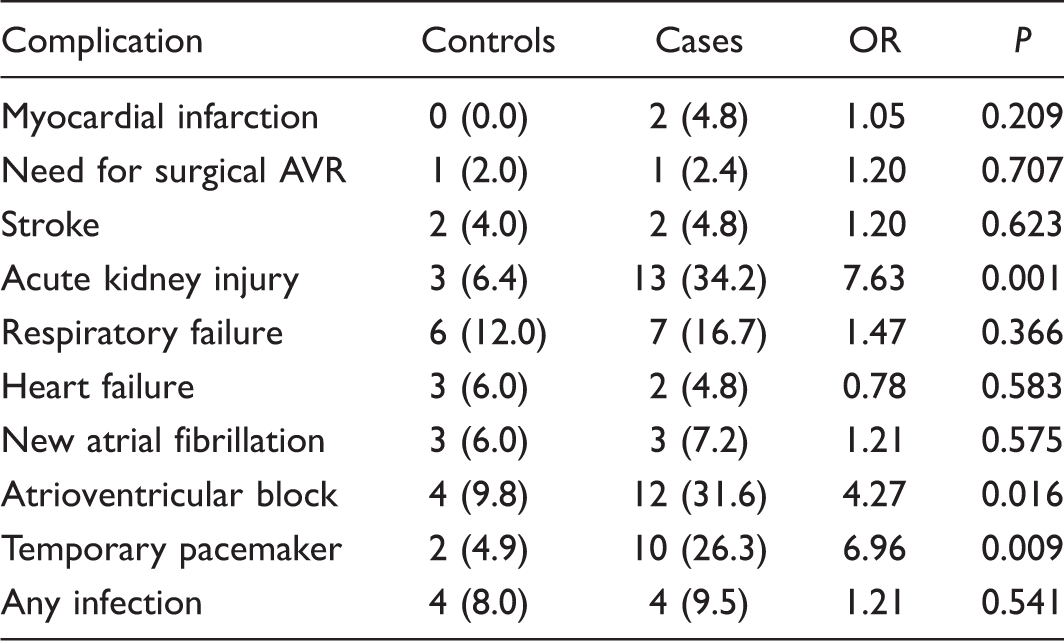
Post-procedural complications between controls and cases (n (%)).
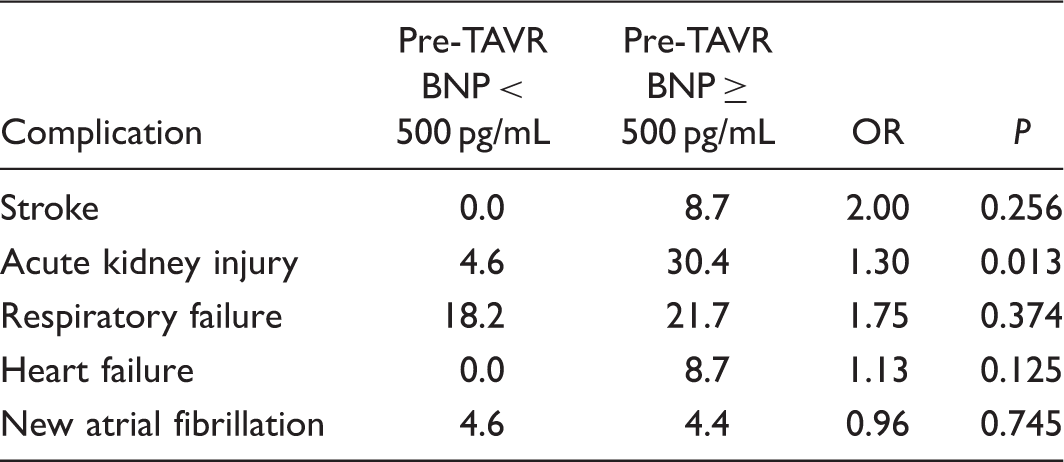
Pre-TAVR BNP levels associated with post-TAVR complications (%).
Among multivariable analyses performed for prediction of AKI after TAVR, moderate/severe PH was found to be the strongest predictor with an OR of 9.5 (95% CI, 2.0–44.8). Additional variables that were found to be predictors of AKI after TAVR included chronic kidney disease (OR = 6.6; 95% CI, 1.4–30.6) and female sex (OR = 6.2; 95% CI, 1.3–30.6).
Among multivariable analyses preformed for prediction of AVB after TAVR, moderate/severe PH was found to be the strongest predictor with an OR of 20.6 (95% CI, 3.4–126.1). Additional variables that were found to be predictors of post-procedure AVB included use of Sapien THV (OR = 6.8; 95% CI, 1.063–43.6) and significant CAD (OR = 7.1; 95% CI, 1.4–37.0), whereas chronic AF was a found to be a negative predictor (OR = 0.12; 95% CI, 0.02–0.8).
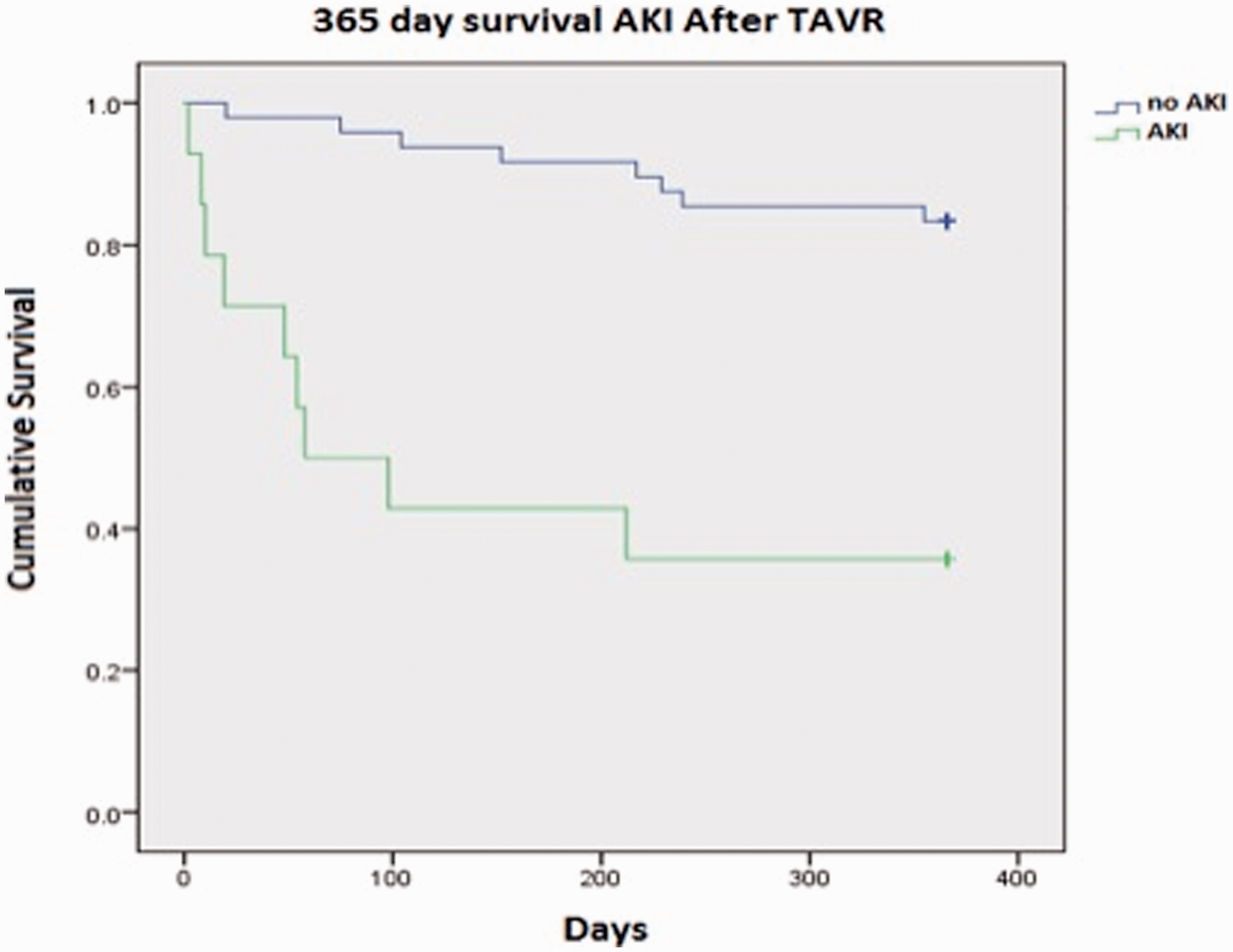
Multivariable analyses were performed for mortality at 120 and 365 days. AKI post-procedure was the only significant predictor (OR = 33.3; 95% CI, 6.0–183.8) for mortality at 120 days (Fig. 3). Post-procedure AVB was the strongest predictor for mortality at 365 days (OR = 10.4; 95% CI, 1.4–79.6). Post-procedure AKI was also a significant predictor of mortality at 365 days (OR, 6.5; 95% CI, 1.4–30.7; Fig. 4).
Kaplan–Meier curve for 120-day mortality and AKI. Post-TAVR AKI correlating with increased mortality at 120 days (OR = 33.3). Kaplan–Meier curve for 365-day mortality and AKI. Post-TAVR AKI correlating with increased mortality at 365 days (OR = 6.5).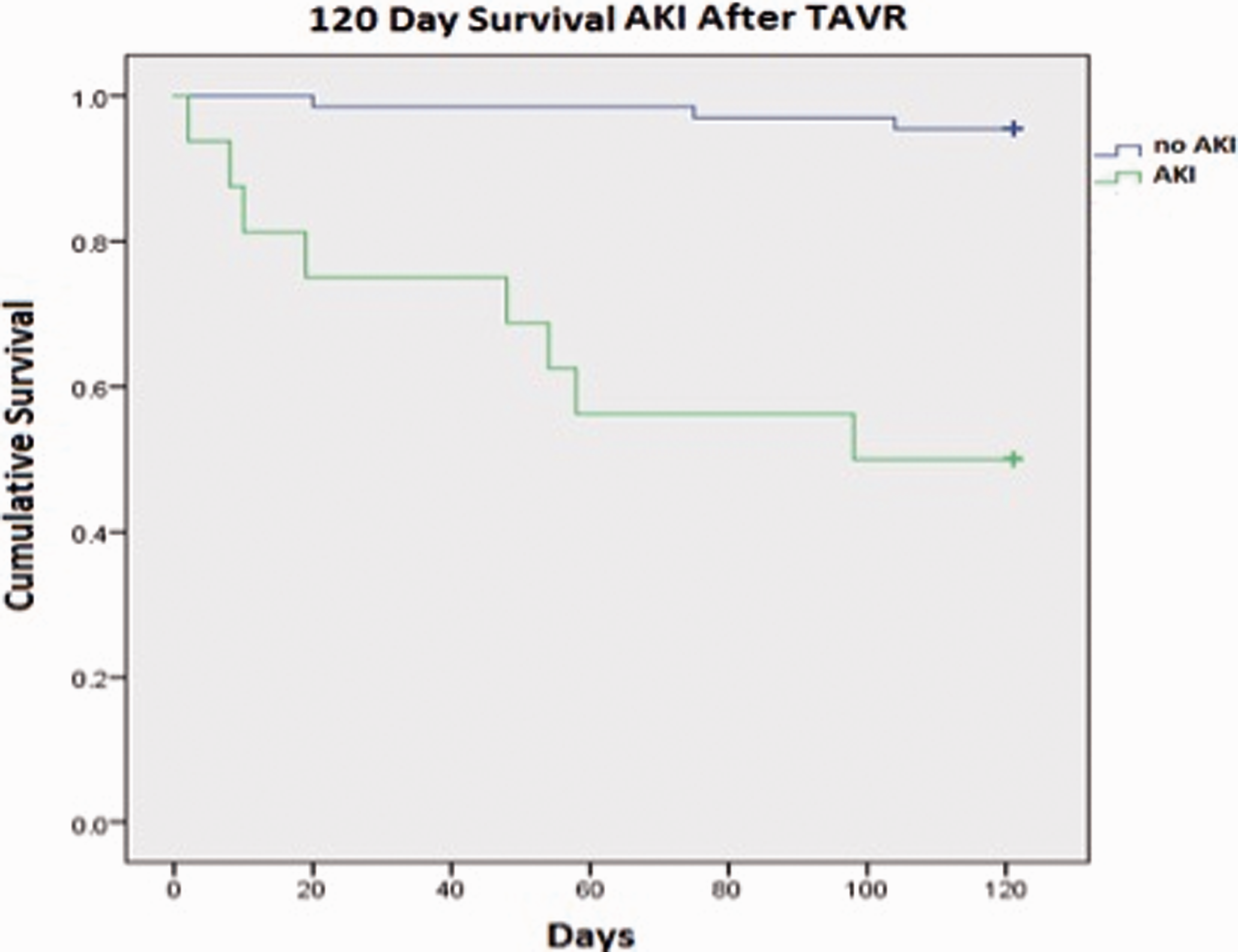
Multiple linear regression analysis showed LOS was associated with pre-TAVR BNP, moderate/severe PH, CAD, and post-procedure respiratory failure. The multiple R-value for the regression was 0.56 while R2 was 0.31, indicating that the multiple linear regression accounts for approximately 31% of the variance in LOS.
Discussion
BNP and pulmonary hypertension
The correlation between BNP and AF in PH was investigated in our study. A higher incidence of preoperative AF was identified in patients with AS with moderate/severe PH undergoing TAVR versus none/mild PH, as shown in previous studies.
23
The increased prevalence of AF in this population is presumably a result of post-capillary PH causing left atrial stretch. Right ventricular dilatation, along with atrial stretch, may play a role in triggering this arrhythmia (Fig. 5). A trend towards increased pre-TAVR AF in moderate/severe PH can be attributed to increased atrial stretch due to passive congestion from AS, which is reflected by higher mean BNP levels in the moderate/severe PH group (pre-TAVR BNP 726.9 pg/mL controls versus pre-TAVR BNP 1869.5 pg/mL cases; P = 0.135).24,26
Pre-TAVR TTE. Pre-TAVR TTE with increased RV dimensions. Patient at risk for elevated BNP, AF, AKI, AVB, increased LOS, and mortality.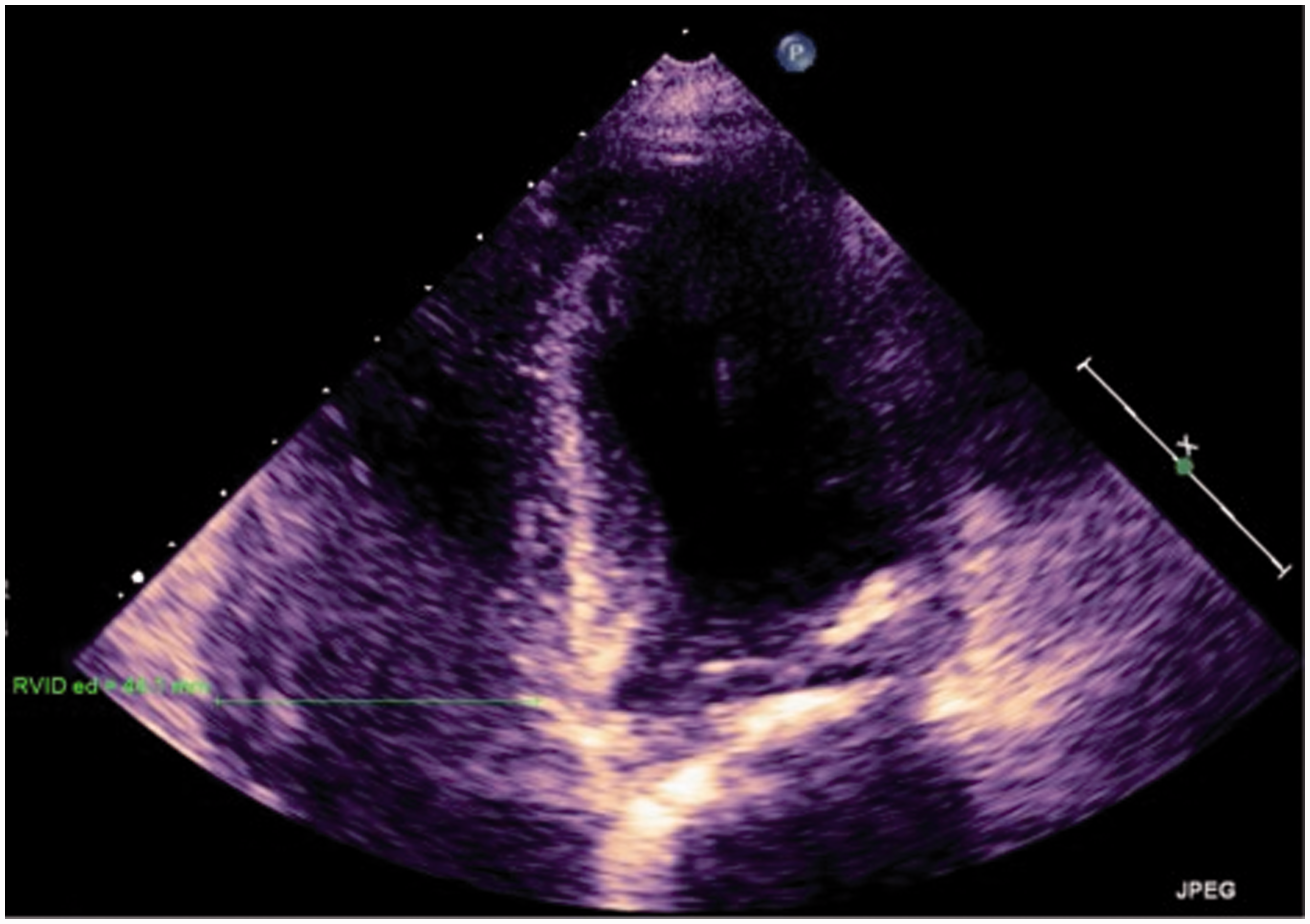
Mortality, cardiac remodeling, and LOS
Our study shows significant higher mortality rates correlating with PH severity at 120 (20.9%) and 365 days (41.9%) post TAVR, consistent with larger cohorts showing 30-day (14.5%), 365-day (30.8%), and two-year (48.4%) mortality.19,21 The FRANCE-2 registry also showed an increase in 365-day mortality (20.8%) in moderate and severe PH patients. 25 Our study, however, uses RHC to define severity of PH rather than TTE, which may be more accurate as a measure of pulmonary vascular resistance (PVR) in this population.
Cardiac remodeling can contribute to the increased mortality in the moderate/severe PH group as well. In severe AS, geometric remodeling of the left ventricle is a known complication. However, with concomitant PH, increased PVR with subsequent remodeling of the RV may further contribute to excess mortality. In addition to cardiac remodeling, post-TAVR complications of PH (AKI and AVB) contribute to worsened mortality at 120 and 365 days.
Along with increasing complications in the post-TAVR period and the subsequent increased rates of mortality, cases also had a longer LOS compared with controls. Pre-TAVR elevated BNP (in all TAVR patients) is an independent predictor of morbidity correlating to increased LOS as well. This suggests maintaining preoperative euvolemia and addressing elevated RV diastolic parameters may help improve outcomes and decrease LOS in these patients.
Atrioventricular block
The development of new AVB (post-TAVR) is a novel finding in AS patients with moderate/severe PH, not reported in previous studies. AVB is a known complication in TAVR patients, especially those with specific co-morbidities including prior cardiac conduction abnormalities, heart failure, hypertension, and DM.27–29 AVB is thought to be due to the proximity of the coronary orifice and conduction system to the aortic valve annulus, which may be impinged upon by the prosthesis.27,28 While long-standing PH can lead to pre-existing dysfunction of the right-sided conduction system, a significant history of right bundle branch block was not noted in our cohort of patients. If this were to exist, further disruption of the left-sided conduction system by the underlying aortic valve disease process and the new prosthetic valve, could result in complete heart block and the need for permanent pacing; however, this would only be present in severe cases of PH and not in mild or moderate cases. The presence of AVB in our moderate/severe PH cases was also associated with an increased incidence of pacemaker placement. Our study also suggests that prosthetic valve type contributes to the incidence of new AVB post procedure, as the Sapien THV was shown to be an independent predictor of heart block in the cohort.
Acute kidney injury
Post-TAVR AKI was another significant complication seen in the moderate/severe PH group. AKI in TAVR patients has been shown to have a strong correlation with postoperative mortality. Prior investigations highlight preoperative renal impairment, transapical versus transfemoral TAVR approach, and need for circulatory support as the major contributing risk factors for post-procedural AKI. 30 In our study, the presence of moderate/severe PH at the time of TAVR was significantly associated with the development of post-TAVR AKI. Pre-procedural volume status with elevated BNP correlated directly with post-TAVR AKI, suggesting that maintaining preoperative euvolemia and potentially addressing increased PVR may modify AKI outcomes.
Studies have shown that PH patients with subsequent RV failure have a stimulated renin-angiotensin-aldosterone system (RAAS) axis. 31 Additionally, electrolyte abnormalities, including hyponatremia, are associated with poorer outcomes in PH patients. 31 The presumed physiology leading to AKI is a result of arterial underfilling due to poor cardiac output, which triggers RAAS and thereby increases sodium and water retention. Additionally, RV failure serves to increase renal venous pressure and hence, decrease the kidney’s glomerular filtration rate, which increases sodium and water retention. These mechanisms define the cardiorenal syndrome that develops in patients with PH and RV failure. This subset of patients has a tenuous fluid status from low cardiac output that ultimately leads to kidney perfusion injury. Identifying patients at risk for AKI is essential as our study showed a significant correlation between AKI and post-TAVR mortality at 120 and 365 days.
Limitations
This study was a post-hoc analysis and therefore is subject to the generalized limitations of retrospective analyses, including the potential role of unknown confounders. In regards to our cohort of patients, we did not distinguish between PH secondary to AS versus other etiologies of PH although other causes for PH were evaluated and excluded. Our sample size was limited due to recent initiation of the TAVR program at our institution; this limitation in patient cohort lends to the possibility of Type 2 errors in our statistical analysis.
We chose to define severity of PH in two separate subsets based on sPAP from RHC at time of TAVR. Because we were not able to calculate PVR or transpulmonary gradient from the RHC at time of TAVR (due to lack of recording cardiac output and pulmonary artery occlusion pressure), we chose to delineate severity of PH based solely on sPAP recorded at RHC. The absence of these hemodynamic measurements, including cardiac output, served to obscure the observations from our study. This severity scoring has been validated in two prior studies by Melby et al. and Yong et al.15,19,33
AKI was presumed to be a result of poor cardiac output from group 2 PH; however, we are only able to establish an association and not causality of a cardiorenal process due to lack of cardiac output measurements.
Conclusions
Our study shows that complications from PH are independent predictors of poor outcomes post TAVR. This retrospective analysis highlights the importance of preoperative optimization in AS patients with concomitant PH. Such optimization could potentially include addressing fluid balance and prophylactic pacemaker implantation in high-risk patients. Additionally, a multivariable analysis that can determine whether sPAP > 50 mmHg is a strong independent predictor of post-procedural AKI and AVB would also serve as a complement to our investigation.
Further prospective studies with pulmonary vasodilators, pre-procedural volume optimization, and prophylactic pacemakers are warranted to decrease postoperative TAVR complications and improve mortality in this PH subset. Increased short-term and long-term mortality, together with AKI and AVB, highlights how pre-existing PH may complicate outcomes in this frail population.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.