
Abstract
Background
Breathlessness is the most common symptom reported by patients with pulmonary arterial hypertension (PAH). The Modified Borg Dyspnea Scale (MBS) is routinely obtained during the six-minute walk test in the assessment of PAH patients, but it is not known whether the MBS predicts clinical outcomes such as hospitalizations in PAH.
Methods
We performed a retrospective study of World Health Organization (WHO) Group 1 PAH patients followed at our center. The dates of the first three MBS and hospitalizations that occurred within three months of a documented MBS were collected. Marginal Cox hazard regression modeling was used to assess for a relationship between MBS and all-cause as well as PAH-related hospitalization.
Results
A total of 50 patients were included; most (92%) were functional class III/IV, 44% and 65% were treatment-naïve prior to their first MBS and hospitalization, respectively. The first recorded MBS was inversely correlated with the first recorded six-minute walk distance (6MWD) (r = –0.41, P < 0.01) but did not track with WHO functional class (r = 0.07, P = 0.63). MBS did not predict all-cause (hazard ratio [HR], 0.91; 95% confidence interval [CI], 0.76–1.08; P = 0.28) or PAH-related hospitalization (HR, 1.04; 95% CI, 0.89–1.23; P = 0.61), though there was a strong relationship between 6MWD and PAH-related hospitalization (P = 0.01). These findings persisted after multivariable adjustment.
Conclusions
Breathlessness as assessed by MBS does not predict all-cause or PAH-related hospitalization. Robust and validated patient-reported outcomes are needed in pulmonary vascular disease.
Keywords
Introduction
Pulmonary arterial hypertension (PAH) is a progressive disease of the pulmonary vasculature associated with significant morbidity, functional limitation, and a limited life expectancy. 1 The decision to initiate or escalate treatment in PAH is multifaceted but World Health Organization (WHO) functional class, which is predominantly determined by the severity of patient-reported dyspnea with activity, 2 is a major factor in risk assessment.2,3 Breathlessness is the most commonly reported symptom in PAH and as it can be perceived, interpreted, and rated by the patient, it is by definition a patient-reported outcome (PRO).4,5 PROs provide important information about health status and disease management not adequately captured by traditional endpoints. While several tools to assess health-related quality of life (HRQoL) have shown promise in PAH, these have not been well-validated or lack pragmatism.6,7
The pathophysiologic mechanisms underlying dyspnea in PAH are not well understood, but in a given patient may represent diminished right-sided cardiac output, abnormal oxygen uptake, ventilatory inefficiency during exercise, or cardiovascular deconditioning.8–10 Signals from the central nervous system and receptors in the right atrium, pulmonary vasculature, lung parenchyma, and chest wall may also contribute to the sensation of shortness of breath. The degree of dyspnea during exercise may therefore reflect a comprehensive “read-out” of multisystem interactions in PAH.
The Modified Borg Dyspnea Scale (MBS) is a 0 to 10 rated numerical score used to measure dyspnea as reported by the patient during submaximal exercise and is routinely administered during six-minute walk testing (6MWT), one of the most common and frequently used measures to assess disease severity in PAH. The MBS is reproducible within a single testing period and tracks with objective indices of exercise intensity in healthy controls and thus has been extrapolated for use in chronic lung disease.11,12 The MBS may provide a minimally cumbersome method of predicting clinical deterioration in PAH, especially since the 6MWT is used widely in PAH care. The MBS was shown to be a univariate predictor of mortality in PAH patients in a single study, 13 but additional evidence tying the MBS to clinical events in pulmonary vascular disease is lacking. We sought to examine the relationship between MBS and hospitalization in patients with WHO Group 1 PAH. Hospitalization for PAH is a potentially clinically meaningful outcome and was the primary driver of composite endpoints in recently completed randomized clinical trials of medical therapies for PAH.14–16 We hypothesized that higher MBS would be associated with an increased rate of all-cause as well as PAH-related hospitalization.
Methods
Study sample
We performed a retrospective study of patients with WHO Group 1 PAH identified from the Rhode Island Hospital Pulmonary Hypertension Center Registry during 1999–2014. We included participants with a diagnosis of PAH confirmed by right heart catheterization and meeting traditional diagnostic criteria 2 who were followed for at least six months and had at least one MBS recorded within the first six months after diagnosis. We excluded participants aged < 18 years. This study was approved by the Institutional Review Board of Rhode Island Hospital (IRB Registration #023914). Written consent was deemed not necessary for this retrospective review.
Modified Borg Dyspnea Scale and clinical variables
All 6MWT performed at our institution prior to 2002 were performed according to published studies.17,18 Thereafter, 6MWT were conducted as per the 2002 American Thoracic Society standards. 19 The MBS recorded at walk test conclusion was collected along with dates of administration. The first MBS performed at our institution was defined as the first test. Up to four serial scores were recorded; the fourth walk date was used for right censoring purposes. Additional clinical data, including demographics, PAH sub-type as designated by the PAH clinician, functional class, serial six-minute walk distance (6MWD), and PAH therapies, were extracted from the registry database.
Hospitalization
Dates and details of hospital admissions were collected from the medical record. A hospitalization event was classified as PAH-related if the admission was due to disease progression (e.g., worsening exercise tolerance, dyspnea, syncope), right heart failure, or initiation or transition of prostacyclin analogue therapies. Hospitalizations related to complications of parenteral prostacyclin analogue administration (e.g., subcutaneous injection site pain or soft-tissue infection, Hickman catheter fracture or infection) but not progression of disease requiring addition of or change in prostacyclin analogue were categorized as all-cause hospitalizations. An additional analysis was performed in which hospitalizations related to complications of parenteral prostacyclin analogue therapy were excluded entirely from all-cause hospitalizations. Dates of MBS were paired with the corresponding sequential hospitalization date if this occurred within a three-month period (the recommended interval for repeating 6MWT in PAH). 3 A sensitivity analysis was performed which included MBS collected within one month of hospitalization.
Statistical analysis
Descriptive statistics were reported as medians and quartiles and categorical data were expressed as counts and percentages. Differences between those with and without one or more PAH-related hospitalization were assessed using Wilcoxon or Fisher’s exact tests (when applicable). Pearson’s correlation was used to evaluate the relationship between MBS and markers of disease severity (functional class and 6MWD). Differences in the first recorded MBS among PAH sub-groups were assessed using a generalized mixed model assuming a binomial distribution with the GLIMMIX procedure. Marginal repeated hazard regression analysis was used to model the relationship between MBS and all-cause and PAH-related hospitalizations adjusted for age and body mass index using the PHREG procedure. Significance was established at the 0.05 level and all interval estimates were calculated for 95% confidence.
Results
Characteristics of the study sample.
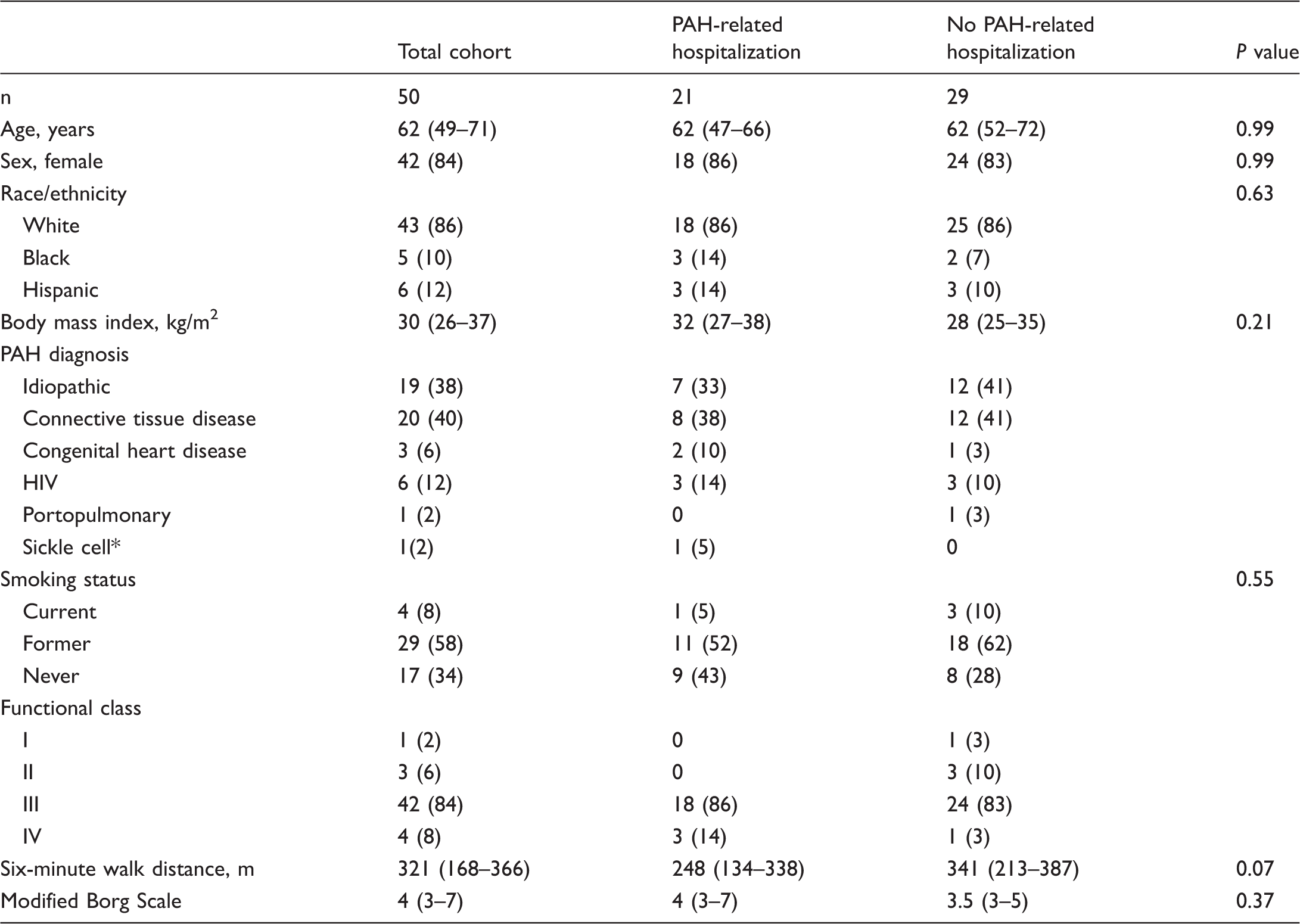
Reported as n (%) or median (interquartile range).
Hemodynamically defined as PAH. P values not calculated when cells contained zero.
HIV, human immunodeficiency virus; PAH, pulmonary arterial hypertension.
The first recorded MBS was inversely correlated with the first recorded 6MWD (r = –0.41, P < 0.01) but did not track with WHO functional class (r = 0.07, P = 0.63). There was a negative correlation between functional class and the first recorded 6MWD (r = –0.43, P < 0.01). No differences were found between PAH subgroups and MBS (P = 0.15). As such, participants with all PAH diagnoses were analyzed as one cohort.
Relationship between Modified Borg Scale and hospitalizations.
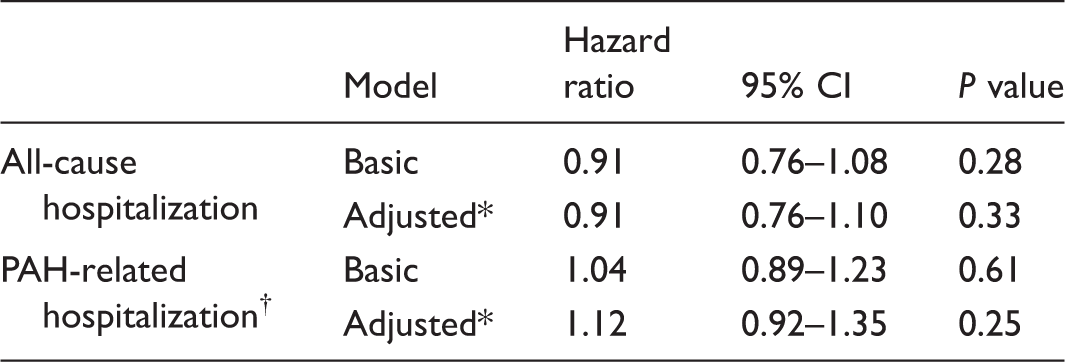
Age and body mass index.
Progression of cardiopulmonary symptoms, right heart failure, and/or change in pulmonary arterial hypertension therapy.
CI, confidence interval.
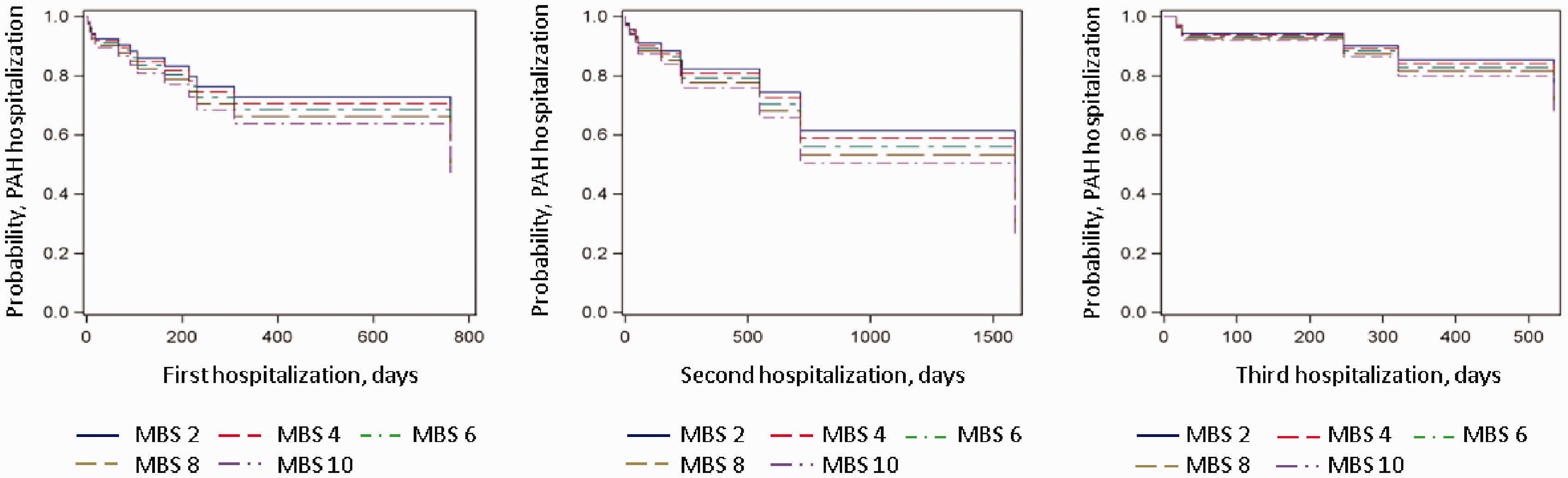
Marginal repeat hazards modeling for PAH-related hospitalization by MBS. X axis is the time to PAH-related hospitalization in days; Y axis is the likelihood of event. The legend corresponds to range of MBS representing each line.
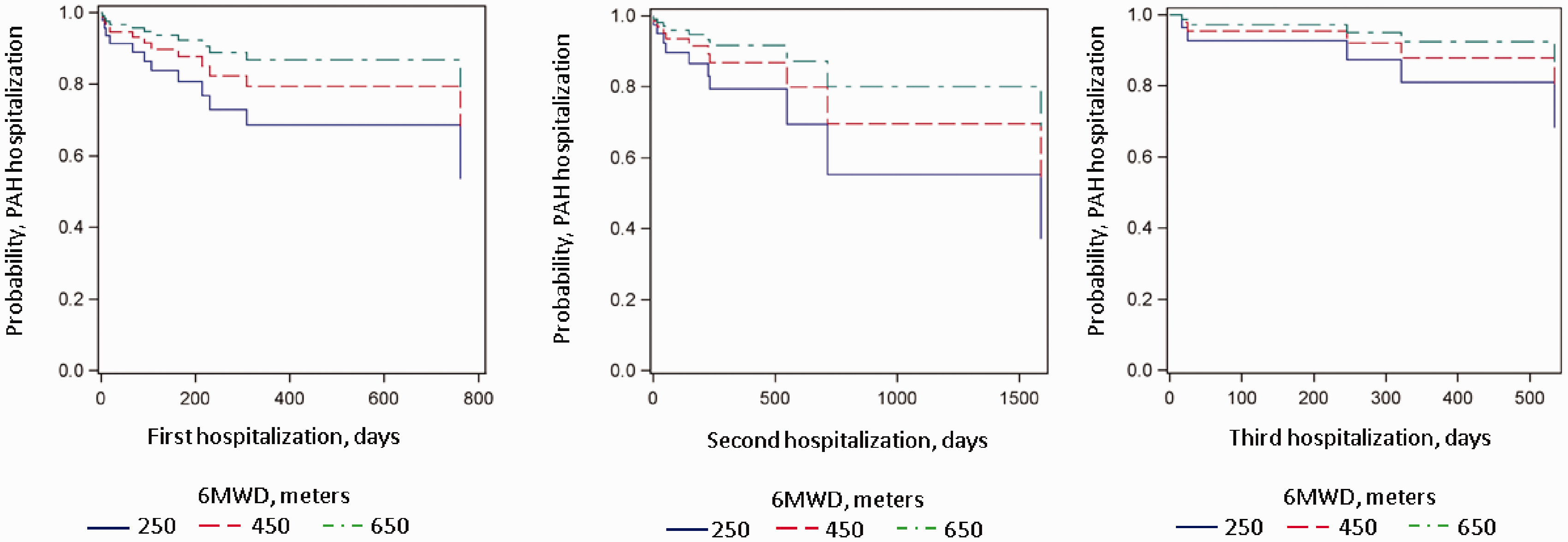
Marginal repeat hazards modeling for PAH-related hospitalization by 6MWD. X axis is the time to PAH-related hospitalization in days; Y axis is the likelihood of event. The legend corresponds to range of 6MWD representing each line.
Discussion
We have shown that routine MBS collection at the end of the 6MWT does not predict all-cause or PAH-related hospitalization in PAH patients from a single center. This is despite a modest inverse correlation between MBS and 6MWD and a strong relationship between longer 6MWD and decreased rates of PAH-related hospitalization. The lack of association between the MBS (mean and maximum values) and a morbidity measure suggests it is an inadequate PRO in pulmonary vascular disease.
A straightforward and validated tool that would allow for patient-characterized shortness of breath is appealing in PAH, since such a measure could represent the sum total of complex cardiopulmonary, nervous system, and musculoskeletal interactions. The MBS is reproducible and tracks with objective indices of exercise intensity such as heart rate, minute ventilation, oxygen consumption, and workload in patients with chronic obstructive pulmonary disease (COPD) and advanced lung disease.12,20 Developed to capture both the rate of perceived exertion and the intensity of the sensation of breathlessness during exercise as a one-dimensional scale, 18 the MBS would be a pragmatic tool in PAH since it is easy to measure, inexpensive, and can be repeated on successive clinical encounters to assess response to treatment, especially since the 6MWD is so widely incorporated into routine PAH care. 2
Patient-reported dyspnea independently predicts mortality in both pulmonary and non-pulmonary diseases.21,22 In COPD patients, subjective dyspnea is superior to pulmonary function tests in predicting clinical outcomes including survival. 23 Dyspnea has also been linked to hospitalizations in COPD, and importantly, quantified dyspnea has a greater impact on HRQoL than objective spirometric measurements.24,25 The MBS has been linked to survival in pulmonary fibrosis and when administered to asthmatic patients after bronchodilator treatment predicts hospitalization or relapse more so than forced expiratory volume in 1 second.23,26,27 While functional class designation has been repeatedly linked to outcomes in PAH and was inversely correlated with 6MWD in our study, only a single study in PAH has demonstrated a relationship between Borg score, which also captures breathlessness, and survival, and this relationship dissipated after multivariable adjustment. 13 Khair et al. recently reported the minimal clinically important difference (MID) for MBS (approximately 1 unit) anchored against 6MWD in a PAH cohort. 28 We also demonstrated a significant inverse correlation between MBS and 6MWD in our study, but the relationship between MBS and clinical events in PAH has not been established.
Over ten HRQoL tools have been studied in PAH. 29 The Cambridge Pulmonary Hypertension Outcome Review (CAMPHOR), which includes breathlessness as a scale, is the most established but multi-dimensional and proprietary in nature.6,30–32 The Short Form-36 (validated in other chronic conditions) correlates with 6MWD and functional class and tracks with PAH therapy; however, the MID with PAH-therapy is large, particularly in the domain of physical activity limitation, suggesting it may be too blunt an instrument for the disease state.32,33 Other metrics (e.g., the Minnesota Living with Heart Failure Questionnaire and emPHasis-10) have either been adapted or designed to be PAH-specific and appear promising but require further validation and are not currently routinely in use, as is the MBS.7,13,34
In our cohort, the median MBS was 3 (IQR, 2.5–5.0) and the maximum was 4.8 (IQR, 3.6–7.0) despite the majority of patients being of advanced functional class before their first hospitalization. This suggests that the MBS in the context of 6MWT may lack the sensitivity needed to adequately discriminate patients’ sense of dyspnea across their disease trajectories, complex treatment regimens (which may impact HRQoL), or may represent a regression to the mean phenomena as patients are subjected to repeated tests (although there was also no relationship between maximum MBS and hospitalizations). Given that the reported MID is small, it is possible that slow incremental changes over time are not perceptible on any given test, leading to a lack of granularity. 28 The change in MBS before and after 6MWT may have added value, but this is not routinely collected at our institution. Interestingly, 6MWD did have an inverse relationship with PAH-related hospitalizations, lending face validity to the assessment of the clinical encounter and its relationship to events, since both 6MWT and MBS are performed concurrently.
Hospitalization as an outcome is an important determinant of survival, cost, HRQoL for the patient and burden on the caretaker in PAH.35,36 Though hospitalization has not been a primary outcome for PAH clinical trials, it has been recognized as a key component of a composite endpoint in several studies.37–39 Despite provider- and geography-specific thresholds for hospitalization, hospital admission is one of the few accepted objective measures of clinical worsening in pulmonary vascular disease.40,41 We found no relationship between hospitalizations (both all-cause and PAH-related) and MBS suggesting MBS may not be a relevant measure of breathlessness or a robust predictor of clinical events in patients with PAH. These results are somewhat surprising considering that increased dyspnea is a common complaint in patients admitted for worsening PAH and given that functional class, a somewhat subjective dyspnea metric, is a powerful predictor of outcome in PAH.42–44 Our study suggests that the degree of dyspnea at the end of 6MWT is not a predictor of later decompensation.
The study was limited by its retrospective nature, small sample size, and single-center design. While we controlled for variation in time between MBS assessment and hospitalization with mixed modeling, residual confounding could exist due to the introduction of PAH therapy or cardiopulmonary conditioning programs, for example. While there was no relationship between maximum MBS and hospitalization, with repeat testing there may be a learning phenomenon and a dilution of an underlying relationship between mean scores and outcomes; low mean MBS in our cohort may also represent suboptimal effort or modification of exertion by patients so as not to elicit breathlessness during 6MWT. We do not have detailed data about the exact timing of the initiation of PAH therapy and a given MBS and the interval between therapeutic changes or additions and MBS was not strictly protocolized. Still, our study sample included only patients with MBS performed three months prior to a hospitalization, the recommended interval for serial reassessments in PAH3 (and one month in a smaller group, with identical results), in order to increase sensitivity and the likelihood that a change in MBS would signal a clinical decline with subsequent hospitalization. While the majority of patients were treatment-naïve at the time that MBS was recorded prior to their first hospitalization, MBS was also a poor predictor of a second or third hospitalization when nearly all patients were on therapy at the time MBS was measured. Although MBS were similar in PAH subtypes in our cohort, subgroup sample sizes were small and this may not be generalizable to the PAH population-at-large (e.g., for all connective tissue disease versus idiopathic patients).
In this retrospective single-center study, we found no association between patient-reported dyspnea as measured by the MBS at the end of 6MWT and all-cause or PAH-related hospitalization. Despite the lack of an association between MBS and hospitalization, the 6MWD recorded at the same time as the MBS tracked inversely with hospitalization rates. These findings suggest that dyspnea as measured by MBS is an insensitive predictor of disease severity in PAH and that other PROs are needed to assess the risk of disease progression in PAH.
Footnotes
Acknowledgements
The authors thank the staff and participants of the Rhode Island Hospital Pulmonary Hypertension Center. This work has previously been presented in abstract form (A7384) at the 2016 American Thoracic Society International Conference, San Francisco, California, May 18, 2016.
Conflict of interest
CEV has received past consulting fees from Bayer, United Therapeutics, and Actelion, as well as grants to her institution from Actelion. JRK serves on the steering committees for Bayer and serves as a site investigator for clinical studies sponsored by Actelion, Bayer, Pulmonary Hypertension Association, NIH, and United Therapeutics. DB has received a grant funded in part by Actelion.
Funding
This work was supported by the National Institutes of Health P20GM103652.