
Abstract
Background:
Nonadherence jeopardizes treatment outcomes in the psychiatric care continuum. However, there was a paucity of data in the resource-limited life trajectories.
Objectives:
This study sought to uncover the psychotropic medications adherence behavior of older adults with severe mental disorders and its modeling predictors.
Design:
A hospital-based cross-sectional study was conducted in selected hospitals of the South Gondar Zone from March 1 to August 30, 2024.
Methods:
A multistage sampling technique followed by stratified and systematic random sampling methods was employed. Data were collected via interviewer-administered semistructured questionnaire and medical record review. A medication adherence rating scale, medication regimen complexity index instrument, Oslo social support scale, drug attitude inventory scale, and internal stigma monitoring index scale were utilized to assess adherence, treatment regimen complexity, social/family support, attitudes toward treatment, and internal stigma, respectively. Ordinal logistic regression deciphered key predictors using adjusted odds ratios (AORs) with a 95% confidence interval at p < 0.05.
Results:
The study sample comprised 423 patients with severe psychiatric disorder (mean (SD) age, 67.3 (±11.9) years; 56.03%, 237 male). Among the participants 255 (60.28%, (95% CI: 58.86–62.11)) had suboptimal adherence behavior. Age, education status, adherence counseling, attitude toward treatment, memory aids, internal stigma, insight, social support, illicit drug use, comorbidity, ADRs, patient-level medication regimen complexity index, and polypharmacy were the predictors identified in the final model.
Conclusion:
Despite multiple methodological limitations, this study suggests that suboptimal psychotropic medications adherence behavior was a critical challenge among older adults with severe mental disorders in geriatric mental healthcare in the Ethiopian hospital settings. We urge policymakers to devise evidence-based policies and strategies focusing on the identified predictors early on and intervene accordingly. Special attention should be given to individuals with low literacy levels, negative attitudes toward treatment, high internalized stigma, poor insight into their condition, substance use, comorbidities, adverse drug reactions, high levels of medication regimen complexity score, and those on polytherapy.
Plain language summary
Non-adherence affects treatment outcomes in the psychiatric care system. This study uncovers the psychotropic medication adherence behavior of older adults with severe mental disorders and its modelling predictors in a resource-strained hospital setting. Approximately two-thirds of older adults with major depressive disorder, schizophrenia, and bipolar disorders were nonadherent to their psychotropic medication therapy. Older age, illiteracy, poor adherence counseling, negative attitude towards treatment, lack of employing memory aids, high level of internal stigma, insight, poor social support, illicit drug use, comorbidity, adverse drug reactions, high level of medication regimen complexity, and polypharmacy were the potential predictors affecting psychotropic medications adherence behaviour.
Background
Mental disorder is a syndrome characterized by clinically significant disturbance in an individual’s cognition, emotion regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes underlying mental functioning, usually associated with significant distress or disability in social, occupational, or other important activities. 1 It is a growing crisis globally, ranking among the top 10 causes of morbidity. 2 According to the Global Burden of Disease 2021, major depressive disorder (MDD) and schizophrenia (SCZ) result in 56.33 (39.3–76.5) and 14.8 (10.9–19.1) million disability-adjusted life years (DALYs), respectively.3,4
Severe mental disorders are among the most common mental health conditions in older adults. Around 14% of older adults aged 60 years and over live with a mental disorder. About 4.8% of older adults are living with a serious mental illness. 5 These conditions account for 10.6% of the total DALYs among older adults. Noncommunicable diseases are prevalent in Ethiopia, with mental disorders being a significant contributor. Severe mental disorders (SMD), mainly SCZ, MDD, and bipolar disorder, were the most common types of mental illnesses in Ethiopia affecting older adults. The incidence rates of major depressive disorder, bipolar disorder, and schizophrenia were 4,650, 614, and 213 cases per 100,000 population, respectively. 6
Tailored psychotropic medications are vital for SMD therapy. However, psychotropic medication nonadherence is prevalent, detrimental, and incurs high costs, reaching $300 billion annually in the United States. However, there is no evidence on the cost of psychotropic medication nonadherence in resource-strained healthcare settings. Nonadherence ends with worse treatment outcomes. A retrospective cohort study revealed that nonadherence to psychotropic medications results in an eightfold increase in relapse rates among patients with SMD (pwSMD). 7 Patients with SMD have psychotropic medication \nonadherence rates ranging from 30% to 65% globally. 8 While no group is immune to nonadherence, older adults with SMDs are particularly vulnerable not only due to psychiatric decompensation, but also the cognitive, adaptive, and functional impairments associated with frailty. 9 Over 50% of older adults with SMD do not achieve remission with first-line psychotropic treatment. Despite the fact that poor treatment outcomes among older adults with SMD stemming from multiple determinants, medication nonadherence is among the key modifiable risk factors. 8 Recognizing the challenges, the WHO has identified SMDs among the nine chronic conditions prioritized for improvement in adherence to care. 10
Multiple factors affect psychotropic medication adherence behavior in older adults including patients’ affective temperaments,11–13 lack of social support, clinical conditions, health system-related issues, 14 socioeconomic barriers, stigma, and limited access to healthcare, attitudes toward medication, polypharmacy, 15 multimorbidity, adverse drug events, and lack of insight9,14 all of which have been identified as predictors of nonadherence. Despite growing research exploring factors influencing SMD medication adherence in Ethiopia,8,16,17 the potentially significant influence of medication regimen complexity (MRC) on adherence behavior has been overlooked.
Although treatment adherence is recognized as a key element in managing SMDs, there is limited data in Ethiopia on the extent of adherence and its predictors among older adults living with SMDs. This study aimed to fill this gap by examining adherence levels and their predictors. The findings may serve as a basis for developing evidence-based policies and strategies to intervene early in poor health trajectories and promote healthy aging through improved medication adherence and comprehensive geriatric mental healthcare.
Methodology
Study design
A multicenter cross-sectional study was conducted in the selected psychiatric departments of hospitals in South Gondar Zone.
Study area and period
This study was conducted in the outpatient psychiatry clinics of five hospitals (Debre Tabor Comprehensive Specialized Hospital, Gayint Primary Hospital, Estie Primary Hospital, Addis Zemen Primary Hospital and Ebinat Primary Hospital) across South Gondar Zone, representing a diversity of urban and rural settings from March to August 2024. This zone is an administrative zone in the Amhara Region, Ethiopia, containing 19 woredas with a population of approximately 2,578,906. It is found at a latitude and longitude of 11°50′18.6″N and 38°05′58.3″E in the northwest of Bahir Dar, the capital city of Amhara Regional State, at 103 km, and Addis Ababa, the capital city of Ethiopia, at 667 km. This zone was structured with ten governmental hospitals (one comprehensive specialized hospital and nine primary hospitals; Figure 1).

Study area map (prepared via ArcGIS V.10.4).
Study population
Older adult patients (⩾60 years old) diagnosed with severe mental disorders (SCZ, BD, or MDD) who were receiving treatment for more than 6 months from psychiatric departments in those selected hospitals.18,19
Inclusion criteria
Patients aged ⩾60 years and primarily diagnosed with severe mental disorders (SCZ, BD, or MDD) who were on psychotropic follow-up treatment for at least 6 months and gave their willingness to informed consent.
Exclusion criteria
Patients with severe cognitive impairment/comorbid dementia that prevents them from understanding the survey questions.
Sample size determination and sampling method
The sample size was determined using a formula for a single population proportion, with a 95% confidence level. The proportion of nonadherence to psychotropic treatment was assumed to be 55.2%, based on a study conducted in Felege Hiwot Referral Hospital. 8 A relative precision of 5% was taken into account. The computed size of sample was 384, based on equation (1).

To account for nonresponse, a 10% adjustment was made to the initial sample size of 384, resulting in a final sample size of 423 for this study.
A multistage sampling technique was used to select participants across the five hospitals. Initially, proportional allocation of samples to the total population of each hospital psychiatric ambulatory clinic was applied using the formula as follows:

ni = SMD sample size from center i, Ni = total population with SMD in center i identified from follow-up registration list, N = total population with SMD from all centers enlisted at follow-up registration books, n = total sample size of this study derived from equation (1). There were 803 patients with SMDs across the five participant hospitals (Figure 2).

Sampling procedure of study participants at outpatient psychiatric clinics in Northwest Ethiopia (N = 423).
DCSH: 349/803*423 = 184, Estie Primary Hospital: 109/803*423 = 57, Gayint Primary Hospital: 149/803*423 = 78, Addis Zemen Primary Hospital: 147/803*423 = 62, and Ebinat Primary Hospital: 79/803*423 = 42.
In the second stage, stratification was conducted within each hospital by grouping patients according to their primary diagnosis—namely, MDD, SCZ, and BD. Proportional allocation of samples to each stratum of each hospital psychiatric ambulatory clinic was conducted using the formula as follows:

si = sample size from strata i, Si = total population in each strata i identified from follow-up registration list, S = total population with SMD from each center, s = total participant sample size in each center derived from equation (2).
DCSH: SCZ: 71/349*184 = 37; MDD: 185/349*184 = 97; BD: 93/349*184 = 50, Estie Primary Hospital: SCZ: 23/109*57 = 12; MDD: 72/109*57 = 38; BD: 14/109*57 = 7, Gayint Primary Hospital: SCZ: 31/149*78 = 16; MDD: 94/149*78 = 49; BD: 24/149*78 = 13, Addis Zemen Primary Hospital: SCZ: 34/117*62 = 18; MDD: 62/117*62 = 33; BD: 21/117*62 = 11, and Ebinat Primary Hospital: SCZ: 29/79*42 = 15; MDD: 38/79*42 = 20; BD: 12/79*42 = 7.
Finally, within each diagnostic stratum, participants were selected using a systematic random sampling technique, where every kth (total population in each stratum/sample size from each stratum) individual was chosen from patient registration lists (Figure 2).
Respondents were screened for eligibility using the Clinical Global Impression-Severity (CGI-S) scale, which evaluates the severity of mental illness. 20 This scale has been utilized in Ethiopian patients with psychiatric disorders.19–22 Psychiatrists used the CGI-S scale in conjunction with their clinical judgment to identify suitable participants. Those who looked incomprehensible, confused, or disabled to enroll in the interview process were evaluated using the CGI-S scale. Patients scoring 1–3 were classified as mild, 4 as moderate, and 5–7 as markedly affected. We excluded those markedly affected ones who scored 6 and 7 specifically. If a respondent did not meet the criteria, the next eligible participant was selected.
Study variables
Dependent variable
Adherence status to psychotropic medication treatment was the principal dependent outcome variable. Based on the WHO definition, nonadherence/suboptimal adherence level refers to “a case in which a person’s behavior in taking medication does not correspond with agreed recommendations from health personnel” involving low and medium adherence statuses. 10
Independent variables
The independent variables consisted of sociodemographic and psychosocial factors such as age, gender, internal stigma, mental health literacy, religion, domicile, ethnicity, education status, marital status, monthly income, occupation, and social support. Clinical and treatment-related features, for instance, diagnosis, duration of illness, type of medication, beliefs/attitude toward treatment, experienced medication-related ADRs, history of complementary medicines use, comorbidities, medication regimen complexity, and polypharmacy were explanatory variables included in this study. Medication regimen complexity is a metric that quantifies the difficulties involved in a patient’s pharmacotherapy. It extends beyond a simple medication count to encompass challenging aspects of administration, such as varied dosage forms, dosing frequency, and additional administrative directives. It can be at the patient level including the overall medication regimen complexity index (MRCI), which involves psychotropic medications in addition to all other non-psychotropic prescriptions and OTC medications, or the psychotropic medication-specific MRCI, which refers to the MRCI calculated using only psychotropic medications. In psychiatry, polypharmacy has been defined as the use of two or more psychiatric medications in the same patient. 23
Finally, behavioral factors such as current substance/illicit drug use status, and health institution factors including availability of medications, distance, waiting time, health insurance coverage, integration of mental health services, therapeutic alliance, and adherence counseling service were among the potential predictor variables investigated in this study.
Data management
Data collection instruments and methods
To meet our objectives, both primary and secondary data were employed. A self-administered face-to-face interview technique with patients and a review of the medical records were employed in the data retrieval process. To capture sociodemographic data, as well as healthcare system, and psychosocial factors, a standardized and semistructured questionnaire was employed (Supplemental File 1). A medical record review checklist was used to gather clinical data such as diagnosis described according to the DSM 5TR, duration of illness, comorbidity, duration of treatment, and medication adverse drug reactions (Supplemental File 2).
We have employed the following validated instruments: the Medication Adherence Rating Scale (MARS-10): Despite several methods for measuring medication adherence are available, none are universally recognized as the most accurate or reliable. Therefore, we employed MARS-10, a comprehensive and standardized 10-item instrument designed to measure adherence, which is commonly used in the Ethiopian population.23–27 A cumulative MARS score of 7–10 suggests good adherence, 4–6 denotes moderate adherence, and 0–3 shows minimal adherence. 28 The scale’s internal consistency was found to be high in this investigation, with a Cronbach’s alpha coefficient of 0.84.
Medication regimen complexity index
A patient-level medication regimen complexity index (pMRCI) was evaluated using this tool. A validated 65-item instrument that comprehensively assesses medication complexity by incorporating factors such as total medication count, dosage forms, dosing frequency, and intricate administration directions, including escalating/deescalating dose, tablet splitting, timing, and food or liquid requirements.29,30 It was commonly utilized among patients with chronic psychiatric and somatic disease conditions in Ethiopia30–33 and abroad.34–36 In this study, the internal consistency of the scale was determined to be high, with a Cronbach’s alpha coefficient of 0.89. Psychotropic medicines were classified according to the Anatomical Therapeutic Chemical (ATC) classification of the World Health Organization. 37 A pMRCI is used to identify individuals who are likely to have trouble managing medication regimens and require interventions. It is a sum of weighted subscores for 3 mutually exclusive medication categories: Psychotropic medication-specific prescription medications regimen complexity, all other prescription non-psychotic medications regimen complexity, and over-the-counter (OTC) medications regimen complexity. The Microsoft Access V.1.0 (Microsoft Corporation; Redmond, Washington; USA) pharmaceutical regimen complexity electronic data capture tool was used to calculate MRCI. Based on these study findings, we classified treatment regimen difficulty levels as low, medium, and high based on pMRCI scores of <10, 10–20, and ⩾20, respectively.
Internalized stigma of mental illness scale (ISMI-29)
A 29-item well-validated instrument was employed to assess self-stigma. 38 Five subscales make up this measure: alienation, stereotype endorsement, discrimination experience, social withdrawal, and stigma resistance. The overall score was obtained by summing the individual scores of the five subscales. Internalized stigma was dichotomized as high for ISMI scores ⩾2.5 and low for scores <2.5. It has been validated and used in several studies in Ethiopia.21,39
The fourth tool was Oslo Social Support Scale (OSSS-3), which is a 3-item scale that assesses the level of an individual’s social support. 40 The instrument has been validated for use in the Ethiopian population with mental disorders.8,41,26,42,43 The scores were interpreted as follows: 3–8 (poor), 9–11 (moderate), and 12–14 (strong). 44
Medication attitude inventory (DAI) tool
A 10-item true/false scale designed to assess patients’ beliefs and attitudes toward treatment. A positive total score infers a positive attitude toward medication, whereas a negative total score infers a negative attitude. 45 This instrument has been employed in studies involving the Ethiopian population with mental disorders.8,46
Level of insight
Assessed based on a three-item questionnaire adopted from studies in Nigeria and Ethiopia.8,44 Scores range from 0 to 3, with 0 indicating no insight, 1–2 indicating partial insight, and 3 indicating full insight.26,44
The procedure of adapting the instrument began with independent translators translating the English version into Amharic and then back to English. The tool was back-translated into Amharic to verify semantic validity after we verified that it was consistent with the original English version. To further guarantee the tool’s applicability and understandability, the questionnaire was pretested on 5% of the sample pwSMD from Woreta Primary Hospital. Then, modifications were made accordingly.
Data were collected by 10 health professionals experienced in psychiatric clinic care. Five were BSc psychiatrists and the rest were clinical pharmacists. One psychiatrist and one clinical pharmacist were assigned to each study site. They were trained for two consecutive days on contents of questionnaire, interview technique, and ethical issues. The training objective was to safeguard confidentiality, preserve data quality, and mitigate underreporting by study participants which also aimed to minimize interviewer bias and improve the reliability of the data. The primary and co-investigators closely monitored the data collection process. Every day, the gathered data were cross-checked for accuracy and consistency.
Statistical analysis
Data were entered into Epi-Info version 7 (Centers for Disease Control and Prevention; Atlanta, Georgia; USA) and transferred to STATA version 17 software (StataCorp LLC; College Station, Texas; USA) for analysis. The descriptive analysis was conducted in summarizing continuous variables with location measures (mean, minimum, and maximum) and dispersion measures (standard deviation and range), and categorical variables with frequencies and percentages. The covariates presented a non-Gaussian distribution. The association between psychotropic medication level of adherence and independent covariates was examined using ordinal logistic regression, given the ordinal nature of the medication adherence status (low, moderate, and high), while adjusting for potential confounders enabled us to correctly model these data. Each independent variable was fitted in the model separately and checked for the assumptions of ordinal logistic regression. We excluded those independent variables with empty cells or low frequencies from the cross-tabulation. Then, those that passed the model assumptions were fitted together to predict the outcome variables. The test of parallel lines was used to verify the assumptions of ordinal regression, which state that the effects of explanatory covariates are the same at every level of the outcome variable. Variables with p-values ⩽0.25 in the bivariable ordinal logistic analysis were included in the multivariable proportional odds model. Furthermore, upon performing an in-depth expert review, some factors might be included in the multivariate analysis even if their p-values were above the cutoff value in the bivariate analysis, based on existing knowledge and evidence. Model fitting information (p-value < 0.01), goodness of fit (Pearson p-value = 0.42 and Deviance p-value = 1.000), and test of parallel lines (p-value = 0.37) were values for the assumptions of the final model. The variance inflation factor (VIF) was used to diagnose the presence of multicollinearity among predictor variables. There is no collinearity among the independent variables in the model, as seen by the mean VIF of 2.61. Finally, the results were expressed using adjusted proportional odds ratio (AOR). Statistical significance was declared at p-value < 0.05 with 95% level of confidence. The findings of this study were reported in accordance with the STROBE statement. 47
Result
Sociodemographic characteristics of the study participants
A cohort of 423 participants was involved in the study with the mean (±SD) age of 67.3 (±11.9) (range: 60–87) years. More than half (56.03%, 237) of them were male. The majority of them were urban dwellers 244 (57.68%), Orthodox Christians 236 (55.80), illiterate 230 (54.37%), retired 193 (45.62%), and had a low monthly income 200 (47.28%). Among the participants, 255 (60.28%) have suboptimal adherence behavior (Table 1).
Sociodemographic characteristics of older adult patients with severe mental disorder at selected hospitals in the Amhara Region, Ethiopia, 2024 (N = 423).

Protestant, catholic.
Oromo, Guragie.
ETB, Ethiopian birr, SD, standard deviation.
Healthcare system and patient-/family-related characteristics
Most of the participants (74%, 313) had health insurance to cover their medical expenses. Among the study participants, nearly half (47.99%, 203) of them had a high rate of internal stigma. A little over half of the patients (50.83%, 215) had a negative attitude toward their psychotropic treatment. Less than half of participants had (n = 158, 37.35%) full insight about their illness. Nearly half of them (170, 40.19%) had a poor relationship with their healthcare providers. The majority of these patients, 313 (74%), have been covered with a community-based health insurance. Nearly half of pwSMD, 211 (49.88%), did not receive enough counseling on adherence strategies as part of their treatment (Table 2).
Health institution and patient-/family-related factors affecting adherence among elderly patients with severe mental disorder at selected hospitals in the Amhara Region, Ethiopia, 2024 (N = 423).

CBHI, Community-based health insurance.
Clinical and treatment-related characteristics of study participants
The predominant participants’ main diagnosis was MDD; 56.03%, followed by SCZ; 23.17%, at last BD 20.80%. In this study, psychotropic medication nonadherence was highly prevalent in patients with SCZ, 67.35%; BD, 59.09%; and MDD, 57.81%. Regarding chronic comorbid diseases, 67.61% (n = 286) of the samples had at least one chronic comorbidity, of them (n = 194) 67.83% had ⩾3 comorbidities. The most common comorbidities were cardio-renal (26.24%), endocrine and metabolic (12.5%), and hematological disorders (9.69%). A significant number of participants were using psychoactive substances (n = 165, 39.01%). Regarding the administered medications profile, nearly half of them, 208 (49.17%), had been treated with antipsychotics and 77.30% of patients were polymedicated (n = 327). The mean number of drugs per patient, including OTC drugs, was 3.67 ± 0.28 (range of 0–7). The mean pMRCI was 37.49 ± 3.11 with a higher mean section of additional instructions (Table 3). More than two-thirds of participants had high to medium treatment regimen complexity. The mean level of psychotropic MRCI was 28.31 ± 3.47. Nonprescription medications also had a significant role (15.47%) for pMRCI (OTC MRCI, 5.80 ± 4.12). More than two-thirds of participants (64.54%) experience ADRs. Adverse drug reaction profile includes extrapyramidal side effects 23.44% (64), sedation and confusion 18.68% (51), anticholinergic effects 17.58% (48), weight gain 17.22% (47), gastrointestinal effects 11.36% (31), agranulocytosis 4.76% (13), cardiovascular effects 3.30% (9), dizziness 2.56% (7), and endocrine effects 1.1% (3).
Clinical characteristic-related factors affecting adherence among patients with severe mental disorder at selected hospitals in the Amhara Region, Ethiopia, 2024 (N = 423).

Combined use of two or more psychoactive substances.
Minerals, dermatologic drugs, and ophthalmic medications.
BD, Bipolar disorder; CAM, complementary and alternative medicine; EMD, Endocrine and metabolic disorders; MDD, major depressive disorder; MSISD, Musculoskeletal and integumentary system disorders; OTC, over-the-counter medication; pMRCI, patient-level medication regimen complexity index; SCZ, schizophrenia; SD, standard deviation; SMD, severe mental disorders.
Factors associated with low adherence to psychotropic medication
Sociodemographic and healthcare system-related predictor covariates
In this bivariate ordinal logistic regression analysis, a total of 22 explanatory variables were examined to determine their association with the outcome of interest. In this unadjusted analysis, gender, age, education status, current substance use history, social support, high internal stigma, poor attitude to drugs for mental health, stigma, poor adherence to counseling, not using reminders to mitigate forgetfulness, pMRCI were moderately associated with low adherence behavior.
Age above 75 years old (AOR (95% CI): 1.98 (1.21–3.08)), poor adherence counseling (AOR (95% CI): 2.48 2.84 (1.09–6.85)), attitudinal issues toward treatment (AOR (95% CI): 1.85 (1.01–3.26)), not using reminders to mitigate forgetfulness (AOR (95% CI): 1.96 (1.02–2.19)), and no family support (AOR (95% CI): 4.05 (1.32–8.10)) were significant predictors of low psychotropic medication adherence level in the final model. Individuals who perceive a high level of internal stigma associated with their SMD are nearly three times more likely to have failed to adhere to their medication compared to those who perceive no stigma (AOR (95% CI): 2.85 (1.09–5.39)). Furthermore, a lack of insight into one’s condition significantly impedes adherence, with individuals lacking insight being twice as likely to be poorly adherent compared to those with good insight (AOR (95% CI): 2.11 (1.30–3.10)). In addition, a current history of substance use presents a substantial barrier to medication adherence, with individuals reporting substance use being two and a half times more likely to be nonadherent compared to those without such a history (AOR (95%CI): 2.50 (1.04–4.67)) (Table 4).
Association between sociodemographic and healthcare system-related covariates and low level of medication adherence in patients with severe psychiatric disorder (n = 423).

Reference.
Single; divorced; widowed.
AOR, adjusted odds ratio; CBHI, Community-based health insurance; COR, Crude odds ratio; ETB, Ethiopian birr; SMD, Severe mental disorder.
Clinical and treatment-related determinant covariates
In the multivariate ordinal logistic regression analysis, factors with a p-value ⩽ 0.25 in the bivariate analysis were considered eligible and included. In addition, complementary medicine use was incorporated into the multivariate analysis despite its p-value exceeding the cutoff, as previous studies identified it as a significant determinant factor of nonadherence to psychotropic medications.48,49
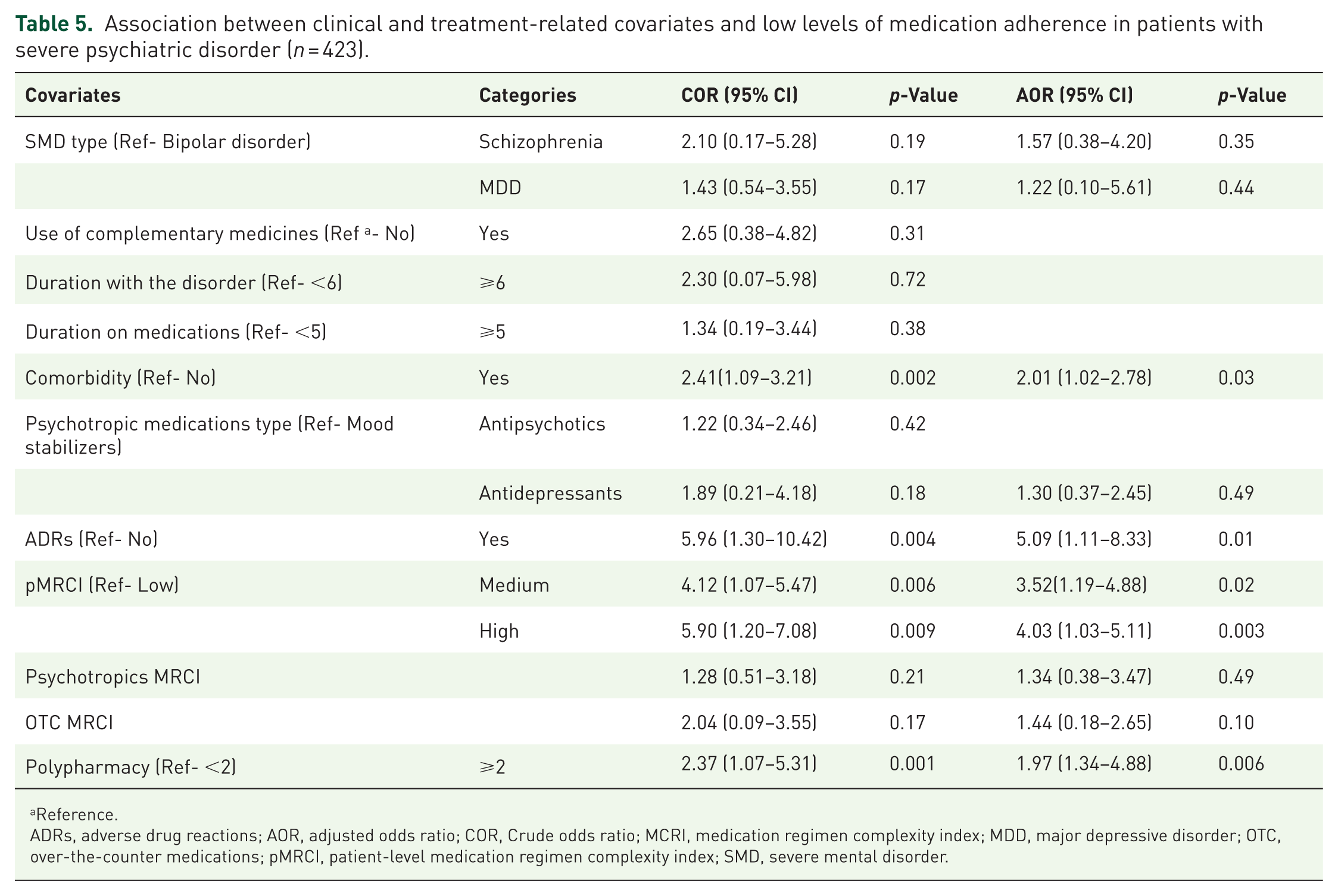
Medication adherence is significantly influenced by several key clinical and treatment-related covariates. Specifically, individuals with comorbidities are twice as likely to have failed to adhere to treatment as compared to those without chronic comorbidities (AOR (95% CI): 2.01 (1.02–2.7)). Experiencing adverse drug reactions (ADRs) increases the odds of low adherence level by fivefold (AOR (95% CI): 5.09 (1.11–8.33)). Furthermore, patients with medium (AOR (95% CI): 3.52(1.19–4.88)) and high (AOR (95% CI): 4.03 (1.03–5.11)) pMRCI levels exhibit higher odds of low levels of adherence. Finally, polypharmacy also doubled the likelihood of a low level of adherence behavior (AOR (95% CI): 1.97 (1.34–4.88)) (Table 5).
Association between clinical and treatment-related covariates and low levels of medication adherence in patients with severe psychiatric disorder (n = 423).
Reference.
ADRs, adverse drug reactions; AOR, adjusted odds ratio; COR, Crude odds ratio; MCRI, medication regimen complexity index; MDD, major depressive disorder; OTC, over-the-counter medications; pMRCI, patient-level medication regimen complexity index; SMD, severe mental disorder.
Discussion
Nonadherence to psychotropic medications is detrimental in the psychiatric care continuum. However, little research has examined medication adherence levels and their predictors in clinic samples of older people receiving psychotropic medication. Thus, this study aimed to evaluate medication adherence level and influencing factors in older adults receiving psychotropic medication.
The overall prevalence of psychotropic medication nonadherence was found to be 60.28% (95% CI: 58.86–62.11). This study outcome was fairly in line with previous studies conducted among pwSMD in Felege Hiwot Hospital (55.2%) 8 and in Debre Markos Hospital (50.9%). 16 Furthermore, it was also in agreement with studies conducted in Nigeria among pwSMD (55.7%). 44 However, this rate of nonadherence was above the study report in Norway (38.4%) 50 involving psychiatric patients with cross-diagnosis from the affective-to-psychotic spectrum with an age range of 18–86 employing the Brief Adherence Rating Scale. This discrepancy might be due to differences in the study population and adherence assessment scale.
Nonadherence to psychotropic treatment was very common in individuals with MDD, SCZ, and BD at a rate of 57.81%, 67.35%, and 59.09%, respectively, in the current study. In concordance with this study, a meta-analysis by Semahegn and his colleagues reported that psychotropic medication nonadherence among patients with SCZ, MDD, and BD was 56%, 50%, and 44%, respectively. 14 These findings also corroborate a study conducted in Norway by Jónsdóttir H. and his colleagues, who reported a nonadherence rate of 41.6% and 33.7% in patients with SCZ and BD, 51 respectively. Besides this, a previous meta-analysis study conducted on nonadherence in MDD reported a 42%, 52 which is closer to our findings. Likewise, a study conducted in northern Ethiopia observed nonadherence rates of 46.9% in MDD patients and 31% SCZ, 53 which also supports our results. Furthermore, a study in comprehensive specialized hospitals in northwest Ethiopia reported a higher nonadherence rate of 51.2% among patients with SCZ, 25 which is also in line with the present study. Despite previous research consistently demonstrating significant nonadherence across these conditions, the current findings are slightly higher. This may be due to the study’s focus on older adults, a population inherently more vulnerable to treatment nonadherence.
Treatment adherence to psychotropic medications is influenced by a variety of factors. In this study, being in the older age group (>75 years old) doubled the risk of a low adherence level. A propensity match score study among pwSMD in China by Dou et al revealed that older age was associated with poor adherence, which corroborates the current study’s finding. 54 Furthermore, previous studies in Mekele, Tigray, on SCZ patients were also in line with this study. 46 In contrast to this study, older age was found to be a significant protective factor against nonadherence in other studies. 55 In addition, a registry-based study in Spain on depressive patients revealed that nonadherence to antidepressants decreases with aging. 56 This discrepancy might be due to differences in the study population, adherence measurement tools, and study design, which included all adults and employed a clinical trial design among pwSMD. Another sociodemographic factor associated with low adherence behavior in this study was illiteracy. This study was in agreement with other studies.46,53 Unintentional medication nonadherence, often attributable to forgetfulness, is a recognized challenge in psychiatric care. Our findings, which highlight the difficulty of remembering medication doses as a key adherence barrier, align with the results from earlier quantitative and qualitative study reports,48,57 reinforcing the potential effectiveness of reminder interventions to mitigate this concern.
Therapeutic regimen complexity was significantly higher in geriatric patients with psychiatric morbidity. 58 In this study, pMRCI was high, 37.49 ± 3.11. This study’s outcome surpassed previous studies on elderly psychiatric patients, which reported average MRCI scores of 17.62 and 19.36. 35 Furthermore, in comparison to a study by Barnett et al, with a mean total MRCI of 14.6, the current study’s pMRCI was superior. This recorded discrepancy might be due to differences in study population, as the current study included only elderly patients with SMD likely to be frail. 59 In addition, moderate to higher pMRCI levels were determinants of psychotropic medication nonadherence in a study on patients with multimorbidity 31 in Ethiopia, consistent with the current study. However, in contrast to the current study, Dean J. and his colleagues, studying children receiving psychotropic medication, reported that MRCI score did not reach a threshold level of significance to be associated with adherence status. 48 This discrepancy might be due to the participants’ age group difference. In the current study polypharmacy was associated with poor treatment adherence in line with previous studies.25,60 By contrast, a population-based registry study in Spain revealed that being polymedicated is a protective factor against nonadherence. 56 This inconsistency between studies might be due to differences in study settings, where in developed countries, polymedicated elderly patients may be admitted to nursing homes with frequent supervision.
Older adults experience psychosocial challenges such as isolation and limited social support, which may interfere with treatment. 61 As revealed in our model, older adults with poor social support were four times more likely to fail to adhere to psychotropic treatment compared to those with a good social support. This study outcome coincides with studies at Felege Hiwot Hospital and Debre Markos Hospital.8,16 Despite the population difference, a study in Australia revealed that a lack of close involvement of family in medication routines results in a higher rate of nonadherence in psychiatric treatment. 48
In the current study, patients with a poor level of insight were poorly adherent to psychopharmacology. Patients with positive insight believe that they require treatment for recovery. Many studies have revealed that patients with poor/no insight into their treatment are associated with nonadherence in pwSMD.8,17,62,63 This might be due to cultural beliefs attributing mental illness to supernatural causes, which can hinder recognition of the condition as a medical disorder and reduce acceptance of psychiatric treatment.
The patient’s attitude toward medication is a proxy for their decision‑making process and is crucial in determining adherence to psychopharmacology, as elderly patients had significantly more negative attitude compared to adults. 61 Patients with SMD who have a negative attitude toward treatment were two times more likely to have failed to adhere to treatment as compared to those who have a positive attitude toward treatment. This finding fairly coincides with the results of previous studies.14,16,17,46,60 Patients with a negative attitude to treatment believe that the chronic drug treatment brings a loss of autonomy and fear of addiction. Healthcare providers should counsel patients to consider treatment as an opportunity to recover their health status and improve their quality of life. Similarly, healthcare providers should adequately explore the patient’s beliefs and attitudes about treatment and provide the appropriate evidence on psychopharmacology.
In this study, pwSMD having a higher internalized stigma have failed to adhere to psychotropic medication, which coincides with previous studies.17,26,42 Individuals with a high level of negative stereotypes and prejudices about their own condition failed to stay motivate and adhere to treatment. Furthermore, a high level of internal stigma was a predictor of treatment discontinuation among depressed older patients, consistent with this study. 64 Current substance use was cited as a predictor of nonadherence in this study. This finding was in agreement with previous studies conducted on pwSMD.16,17,25,46,60,63
In this study, chronic disease comorbidity was a predictor of nonadherence. This result is in concordance with previous studies.60,65 Furthermore, the current study result corroborates existing literature reports in the population with BD. 66
Older adults are more sensitive to the psychotropic medications’ ADRs, such as dizziness, motor disorders, and orthostatic hypotension, leading to a fear of falling and experiencing trauma. 67 They are apprehensive regarding these adverse effects, and such apprehensions influence their adherence. This study reported that individuals who experience ADRs were five times more likely to fail to adhere to their treatment as compared to those who do not. This is in concordance with previous studies.16,25,26,46,60 In addition, a case-control study in Malaysia on elderly psychiatric patients revealed that ADRs were associated with treatment discontinuation, 49 which corroborates the current finding.
Adherence issues are intricate and multifaceted. Predictor-focused and tailored adherence therapy interventions are able to improve adherence for optimum treatment outcome.68,69 Thus, in this study, 87.06% of patients with suboptimal adherence received interventions accordingly.
Limitations
This study had multiple limitations. Due to the subjective measure of adherence, social desirability, or self-presentational bias, and recall bias may have affected this study; hence adherence level may have been overestimated. The study had a cross-sectional design, where adherence was measured at a single time point, despite it being a dynamic process that changes over time. Considering that the study was conducted in a hospital setting in pwSMD morbidity using limited samples, the findings cannot be generalized to other clinical areas. This study also did not consider other factors that may influence adherence, including the healthcare provider features, potentially inappropriateness of medications, role of pharmacists in psychiatric care, caregivers’ characteristics such as age, education status, and status of psychotherapy services.
Conclusion
Altogether, suboptimal adherence behavior to psychotropic medication was prevalent among elderly patients with severe mental disorders in the Ethiopian hospital settings. This is the first study to identify medication regimen complexity as a determinant of psychotropic treatment adherence. Despite several limitations, this study attempts to identify the potential target areas wherein a suitable intervention could be made to improve adherence in psychopharmacology.
As a result, we recommend enhancing patient adherence to psychotropic medications by strengthening adherence counseling, simplifying medication regimens and polypharmacy through comprehensive medication reviews and deprescribing, and mitigating ADRs through medication reconciliation and regular monitoring. Additionally, addressing patient misconceptions with scientific explanations and promoting mental health literacy are crucial. Furthermore, rigorous studies are required to assess these outcomes while accounting for critical confounding variables, most notably regimen appropriateness evaluated via established explicit criteria such as Beers and STOPP/START, to provide a more holistic understanding of the drivers of nonadherence.
Supplemental Material
sj-docx-1-tpp-10.1177_20451253251387413 – Supplemental material for Psychotropic medications adherence status and its determinants among older adults with severe affective and psychotic disorders: a multicenter cross-sectional study
Supplemental material, sj-docx-1-tpp-10.1177_20451253251387413 for Psychotropic medications adherence status and its determinants among older adults with severe affective and psychotic disorders: a multicenter cross-sectional study by Woretaw Sisay Zewdu, Tigabu Eskeziya Zerihun, Desalegn Addis Mussie, Abel Temeche Kassaw, Taklo Simeneh Yazie and Tilaye Arega Moges in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-docx-2-tpp-10.1177_20451253251387413 – Supplemental material for Psychotropic medications adherence status and its determinants among older adults with severe affective and psychotic disorders: a multicenter cross-sectional study
Supplemental material, sj-docx-2-tpp-10.1177_20451253251387413 for Psychotropic medications adherence status and its determinants among older adults with severe affective and psychotic disorders: a multicenter cross-sectional study by Woretaw Sisay Zewdu, Tigabu Eskeziya Zerihun, Desalegn Addis Mussie, Abel Temeche Kassaw, Taklo Simeneh Yazie and Tilaye Arega Moges in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-docx-3-tpp-10.1177_20451253251387413 – Supplemental material for Psychotropic medications adherence status and its determinants among older adults with severe affective and psychotic disorders: a multicenter cross-sectional study
Supplemental material, sj-docx-3-tpp-10.1177_20451253251387413 for Psychotropic medications adherence status and its determinants among older adults with severe affective and psychotic disorders: a multicenter cross-sectional study by Woretaw Sisay Zewdu, Tigabu Eskeziya Zerihun, Desalegn Addis Mussie, Abel Temeche Kassaw, Taklo Simeneh Yazie and Tilaye Arega Moges in Therapeutic Advances in Psychopharmacology
Footnotes
Acknowledgements
First, our special thanks go to the sample participants and data collectors. I would like to express our greatest gratitude to Debre Tabor University College of Health Science, Department of Pharmacy, and the administrators of the participant hospitals and psychiatric clinics for providing the chance to conduct this study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.