
Abstract
Combination therapy is commonly used to achieve better glycemic control, but Medication Regimen Complexity (MRC) can pose challenges for treatment adherence and outcomes. While some studies have explored the impact of MRC on patient outcomes, evidence remains inconclusive. Therefore, we aimed to explore the impact of MRC on diabetes management. This rapid review systematically identified studies on diabetes patients with complex medication regimens and their clinical and nonclinical outcomes. A comprehensive search was conducted across four databases (PubMed, Web of Science, Scopus, and Cochrane) from January 1967 to September 2023. Study quality was assessed using the Joanna Briggs Institute tool, while the overall evidence certainty was evaluated using the GRADE approach. Thirteen studies met the inclusion criteria, of which 11 focused on type 2 diabetes. The primary outcomes assessed were glycemic control and medication adherence. While findings on glycemic control conflicted among 12 studies, most indicated that higher MRC was associated with poor glycemic control. Four studies reported improved adherence with lower MRC. Additionally, high MRC was associated with greater medication burden and diabetes-related distress, though its impact on body weight remained inconclusive. Conversely, regimen simplification was linked to improved quality of life and increased treatment satisfaction. In conclusion, the findings suggest that MRC may contribute to various challenges in diabetes management. Simplifying regimens and standardizing outcome assessments are essential for optimizing treatment strategies in both practice and policy.
Plain language summary
People with diabetes often need to take multiple medications to help control their blood sugar levels. However, when treatment plans become too complex, it can be harder for patients to follow them properly, which may affect their health. Some research has looked at how complex medication routines impact diabetes management, but the results are not clear. In this study, we reviewed existing research to better understand how medication complexity affects people with diabetes. We searched four major medical databases for studies published between 1967 and 2023 and carefully assessed their quality. We found 13 relevant studies, most of which focused on type 2 diabetes. Our review showed mixed results. In most studies, more complex medication routines were linked to worse blood sugar control. Some studies also found that simpler medication routines helped patients take their medications as prescribed. Additionally, complex treatment plans were often associated with a higher medication burden and more stress related to diabetes. However, their effect on body weight was unclear. On the other hand, some studies have shown that simplifying treatment plans improves treatment satisfaction and quality of life. Overall, our findings suggest that complicated medication plans may make it harder for people to manage their diabetes effectively. To improve diabetes care, it is essential to simplify medication routines and ensure that future studies use consistent methods to measure patient outcomes
Keywords
Introduction
Diabetes continues to pose a significant challenge to individuals and healthcare systems worldwide. Recent reports showed that its prevalence is still increasing, with the expectation to rise from 537 to 643 million between 2021 and 2030, with most cases related to type 2 diabetes mellitus (T2DM). Moreover, in 2021, it was responsible for 6.7 million deaths and an increased health expenditure by 316% over the last 15 years.1,2 With this increased prevalence, variation of individual tolerance to medication, and the need to improve patients’ outcomes, convenience, and safety, different new antidiabetic medications have been approved in the market. However, most are used as an add-on medication. 3 Combination or add-on therapy remains standard practice among healthcare prescribers to achieve optimal glycemic control, especially in chronic progressive cases. Early use of this approach is also recommended in selected individuals at treatment initiation to extend the time to treatment failure.3 –5 However, according to the American Diabetes Association (ADA), different patient-specific factors affect the choice of medication in patients with T2DM, such as individualized glycemic and weight targets, medication side effects, cardiorenal protection, patient choice, and complexity of medication regimen. Therefore, the ADA recommends that medication regimens and medication-taking behavior should be regularly evaluated (every 3–6 months) and adjusted as needed to account for factors influencing treatment choice and patient outcomes, particularly in individuals with T2DM who often require amendments and add-on medications over time. This regular evaluation helps optimize medication use while reducing treatment discontinuation and cost. 4
Nowadays, healthcare providers face increasing challenges in selecting appropriate medications to improve patients’ health outcomes and prevent disease complications and hospitalization, challenges often linked to the complexity of diabetic medications.6 –8 Medication Regimen Complexity (MRC) refers to the number of medications in the regimen, dosing frequencies, dosage forms, and additional medication directions. 9 Previous studies identified different factors associated with MRC. For example, elderly patients often had a higher MRC than other age groups.10,11 Similarly, the presence of comorbid conditions, for example, congestive heart failure and chronic pulmonary disease, was associated with having MRC in many patients.11,12 Consequently, the ADA has recently recommended simplifying medication regimens in high-risk populations, for example, elderly patients with multiple comorbidities, to reduce the treatment burden and prevent diabetes complications such as hypoglycemia. 4 Some studies have explored the association between MRC and different patient characteristics5,11,13 –15; however, evidence regarding its impact on patient outcomes varies.
Aim of the study
This rapid review aims to explore the impact of MRC on diabetes management. The objectives include identifying, describing, and critically appraising studies evaluating the impact of MRC on health outcomes for patients with diabetes.
Methods
Search strategy
This rapid review followed the systematic approach described in the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) to improve this review’s clarity, validity, and suitability. 16 Given the need for timely evidence synthesis, the rapid review approach was employed to gather and analyze relevant literature while maintaining methodological rigor efficiently. A rapid review is a streamlined form of a systematic review that utilizes accelerated methods, such as restricting search databases, limiting inclusion criteria, and simplifying data extraction, to produce findings within a shorter timeframe. This approach was deemed appropriate to provide timely insights while ensuring a systematic and transparent review process. Four databases (PubMed, Web of Science, Scopus, and Cochrane Database of Systematic Reviews) were searched between January 1, 1967 and September 8, 2023 for studies in English. Hand-searching of the reference lists of eligible studies was also conducted. The research team discussed the search strategy and keywords (provided in Supplemental File 1). The keywords used were categorized into two groups: (1) those related to the objective of the study, which are “medication,” “medication regimen,” “drug,” “Simplification,” “complexity,” “Complex,” “Complicate” and (2) keywords related to the study population; “diabetes.” The Boolean operator “OR” combined similar and related keywords, for example, complex, complexity. These were then combined using AND with keywords related to the study population (patients with diabetes). The search was restricted to papers published in English. Studies were initially screened for inclusion by title and abstract, followed by full-text review. Gray literature was discussed with the research team for inclusion. Three collaborative researchers conducted the literature search, study selection, and data extraction. To ensure the validity and consistency of data synthesis, the principal investigator resolved discrepancies and reviewed the data extraction.
Inclusion and exclusion criteria
Inclusion and exclusion criteria (Table 1) were informed by elements of the PICOS framework (Population, Intervention, Comparator, Outcomes, and Study design), and adapted to the focus of this review.
Studies’ inclusion and exclusion criteria.
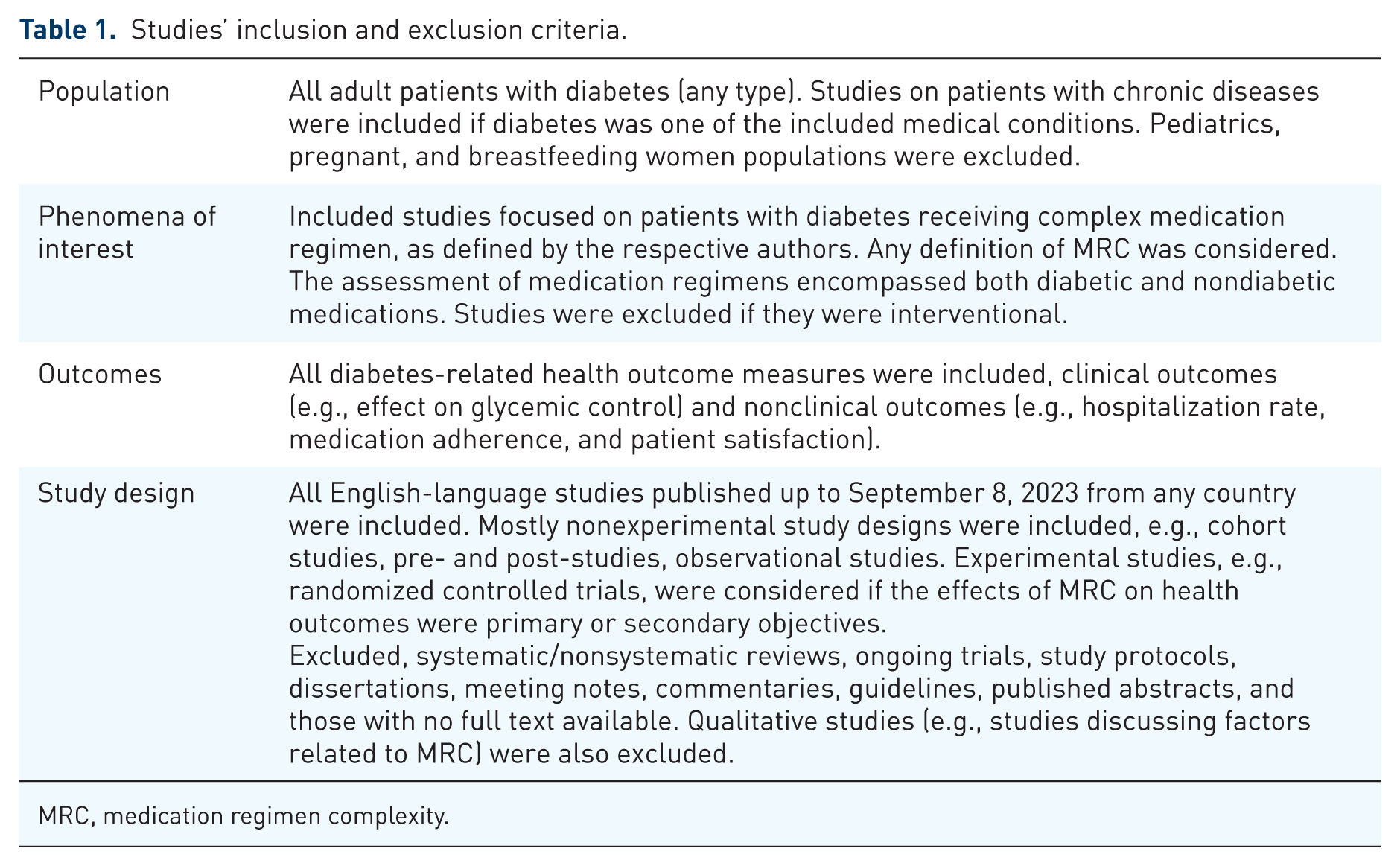
MRC, medication regimen complexity.
Data extraction and analysis
In this review, the impact of MRC on diabetes management was assessed based on reported associations, trends, or measured outcomes in the included studies. Since interventional studies were excluded, the analysis primarily relied on available randomized controlled trials (RCTs) and observational studies. Cross-sectional and cohort studies provided insights into associations rather than causal relationships, while longitudinal studies offered further context regarding trends over time. The interpretation of findings considered study design limitations, particularly regarding causality.
For quality assessment, the Joanna Briggs Institute tool was used to appraise the included studies critically, evaluate the methodological quality of the studies, and examine potential bias in the studies’ designs, conduct, and analysis. 17 All included papers in this rapid review were subjected to rigorous appraisal by two critical appraisers. The certainty of overall evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach, which provides a transparent and structured method for evaluating research findings, particularly in clinical decision-making and guideline development. The assessment of the certainty of evidence goes beyond critical appraisal to consider the overall quality and reliability of evidence presented. By evaluating the evidence, it would be possible to determine whether it is strong, weak, or a combination of both. GRADE classifies evidence into four levels, also referred to as certainty or quality of evidence: very low, low, moderate, and high. 18
Results
The electronic search identified 13 eligible studies. Figure 1 gives an overview of the screening process using the PRISMA flowchart. The included studies examined the impact of MRC on various outcomes, including glycemic control and medication adherence, and other key aspects of diabetes management.

PRISMA flowchart of the rapid review results.
Quality of the included studies
The studies generally met high standards for clarity in sample inclusion, valid and reliable measurement of exposure and outcomes, and appropriate statistical analysis. However, some studies lacked clear identification and handling of confounding factors, which may impact the internal validity of their findings.5,19 Despite this, the overall quality of the studies was adequate, with most employing a sound approach to evaluating the impact of MRC on glycemic control and other outcomes in diabetes management.
General characteristics of the included studies
The 13 quantitative studies identified from the literature search had different study populations, durations, designs, and settings. They were classified into themes based on the outcomes. Details of the studies are provided in Supplemental File 2. In general, 11 studies enrolled patients with T2DM. The commonly used method was the prospective cross-sectional design (n = 5), followed by retrospective cohort (n = 3) and RCTs (n = 3), retrospective cross-sectional design (n = 1), and prospective cohort (n = 1). Researchers commonly used primary care and hospital-based settings to collect data (n = 5, in each setting), as both reflect real-world, routine healthcare practice and provide access to diverse patient populations and their medical records.
Characteristics of exposure (MRC)
The operational definition of MRC varied across the studies. The Medication Regimen Complexity Index (MRCI) developed by George et al. 9 was commonly used.5,6,19 –25 Five studies evaluated the MRC outcomes at the disease-specific level, that is, assessing only antidiabetics.5,24,26 –28 While most studies evaluated MRC outcomes at both disease-specific and patient levels,6,20 –23,25 only one study assessed MRC outcomes at the patient level by considering all medications—antidiabetics, other prescribed medications, and over-the-counter (OTC) medications. 29 Each of the previous methods provides distinct insight and has advantages and limitations. For example, while evaluating MRC at the disease-specific level is straightforward and focuses on a particular health condition, it does not account for the potential interactions with OTC medications or those prescribed for other comorbidities. The patient-level evaluation, or the use of both approaches (the disease-specific and patient-level), also presented certain limitations. For example, they are more complex to analyze, especially in patients with comorbidities, require time and effort, and necessitate full access to patients’ records, including OTC medications, which may not be typically reported in their records. Thus, a risk of attrition bias (i.e., having missing or incomplete patient data) might exist with these types of evaluations.
Evidence synthesis
For the types of outcomes, the commonly assessed MRC outcomes were glycemic control and medication adherence. Other less-evaluated outcomes included medication burden (i.e., number of medications used), quality of life (QoL), weight reduction, diabetes-related distress, and treatment satisfaction.
Effects of MRC on glycemic control
Studies evaluating the glycemic control outcome (n = 12) had conflicting findings concerning its association with MRC. Collectively, the studies suggest that higher MRC is often associated with poorer glycemic control. Table 2 provides an overview of the overall effect of MRC on glycemic control.
Findings of the effect of MRC on patients’ glycemic profile.

AOR, adjusted odds ratio; CI, confidence interval; GRADE, Grading of Recommendations Assessment, Development, and Evaluation; MRC, Medication Regimen Complexity; MRCI, Medication Regimen Complexity Index; NS, not significant; RCT, randomized controlled trials; SD, standard deviation.
Most studies found that high MRC was associated with poor glycemic control. This indicates that patients with more complex regimens tend to have higher HbA1c levels, suggesting worse glycemic control. However, the studies applied different operational definitions for MRC. Four studies evaluated the MRC outcomes at the disease-specific level, that is, assessing only diabetes medications.5,26 –28 Others assessed the MRC outcomes at the patient level. At the overall patient level, the significance of the results varied depending on the method used to evaluate MRC. For example, two studies found significant changes in glycemic control with complex regimens.21,29 Another two studies reported a significant association only with the high MRCI scores.6,20 However, three studies did not report any change in HbA1c when using a complex regimen.20,26 –28 Notably, three studies indirectly evaluated the impact of MRC on glycemic outcomes by examining the effects of various regimen simplification strategies on different clinical outcomes.26 –28 However, it is important to consider several factors that may influence the results, including the method of delivery (e.g., type of medication, in-person visits, or phone follow-ups), the provider administering the intervention (e.g., nurse vs pharmacist), and the duration of exposure to the intervention. Additionally, the timeframe used to detect changes in the glycemic profile varied across studies. For example, HbA1c level was measured between 3 and 6 months in five studies.19,21,25,28,29 Other authors indicated using the most recent HbA1c or fasting blood glucose measures, but the exact timeframe was not reported.5,6,20,23 These characteristics pose a high risk of bias, which justifies reducing the certainty of the evidence by two levels, from high to low.
Effects of MRC on medication adherence
Four studies assessed the level of medication adherence in patients with diabetes and complex regimens.20,23,24,28 Regardless of the strengths and limitations of each type of assessment, studies had similar findings. Table 3 overviews the overall association between MRC and medication adherence.
Findings of the effect of MRC on patient medication adherence.

AOR, adjusted odds ratio; BI, basal insulin; BBI, basal-bolus insulin; CI, confidence interval; GLP1RA, glucagon-like peptide-1 receptor agonist; GRADE, Grading of Recommendations Assessment, Development, and Evaluation; IQR, interquartile range; MMAS, Morisky Medication Adherence Scale; MRC, Medication Regimen Complexity; MRCI, Medication Regimen Complexity Index; RCT, randomized controlled trials; SD, standard deviation.
The studies found a significant association between medication adherence and MRC, that is, the lower the MRC the patients had, the better adherence rates were reported. However, the methods used to measure medication adherence varied. Four studies used in-person or live assessments where investigators asked patients to complete validated questionnaires, such as the Morisky Medication Adherence Scale.20,23,24 In contrast, one study assessed patients’ medication adherence through chart and record reviews, calculating the proportion of days covered over a fixed time interval. 28
Effects of MRC on other health outcomes
Few studies assessed the effect of complex medication regimens on health outcomes including medication burdens, diabetes-related distress, and influence on body weight.5,22,23 The studies found that medication burdens and diabetes-related distress were associated with high MRC and resulted in lower chances of achieving control levels of HbA1c.5,22,23 Conflicting results were observed regarding the effects of MRC on body weight. Some studies have reported significant weight reduction in patients who received and adhered to their simple diabetes medication regimen.27,28 On the other hand, others did not observe any reduction compared to study cohorts with complex regimens. 26 Yet, two studies assessed the impact of MRC on treatment satisfaction and found positive effects on satisfaction after simplifying the medication regimens in patients with diabetes.27,28 Two studies highlighted the positive impact of regimen simplification on QoL in patients with T2DM. Ando et al. 26 found that QoL scores significantly improved in both treatment groups over 24 weeks, despite no significant difference between them (p = 0.05). Patel et al. 28 reported a significant QoL improvement in patients who received combination therapy with a glucagon-like peptide-1 receptor agonist (GLP1RA) plus basal insulin (BI) over 6 months, emphasizing the benefits of a less complex regimen. These findings suggest that simplifying medication regimens can enhance patient well-being and treatment satisfaction. However, previous measures (e.g., QoL, weight reduction) were either secondary outcomes in studies that lacked sufficient power to detect differences between groups or had uncertain long-term sustainability. Therefore, additional research is needed to determine the strength of the association between these outcomes and MRC in patients with diabetes.
Discussion
Managing T2DM requires a combination of lifestyle modifications and pharmacological interventions to maintain glycemic control. Multiple factors can influence the outcome of patients’ glycemic control, making it challenging to achieve optimal control. The findings of this review highlighted a potential cycle between MRC, glycemic status, and medication adherence (Figure 2). This interplay between MRC, poor glycemic control, and nonadherence in patients with diabetes is a multifaceted issue with significant implications for long-term health outcomes. 30

The cycle of MRC, medication adherence, and glycemic control.
While complex regimens aim to improve glycemic control, a growing body of evidence suggests that the complexity itself can pose significant barriers to medication adherence. Regimens requiring multiple doses, diverse medication types, and regular adjustments can overwhelm patients, leading to missed doses or incorrect medication use. A significant clinical paradox is highlighted in this review, indicating that simplifying the regimen may not always result in improved glycemic control, despite being linked to increased adherence.31,32 Some research has shown that simplified regimens produced results similar to those of more complex ones. 32 In contrast, more complicated regimens might be needed for intensive glycemic management (as recommended by ADA guidelines, which support the early use of combination therapy in some patients) to achieve optimal outcomes. 4 This conflict underscores the need to balance between treatment intensity with regimen complexity. The goal is not to simplify regimens indiscriminately, but to tailor therapy to patient-specific factors such as comorbidities, risk of nonadherence, and clinical response. In some cases, simplification using fixed-dose combinations or extended-release formulations may help reconcile these opposing priorities by maintaining glycemic efficacy while reducing complexity.32,33 Future studies should identify patient subgroups, such as older adults or those with multiple comorbidities, who are most likely to benefit from regimen simplification. Developing predictive tools or personalized complexity thresholds based on clinical, behavioral, or demographic characteristics may help tailor treatment intensity more effectively. In addition, prospective cohort studies and RCTs are still needed to evaluate the clinical and patient-centered outcomes of simplification strategies.
The relationship between MRC and glycemic control in patients with diabetes is complex and sometimes contradictory. Several factors may explain these inconsistencies across studies. First, glycemic control is a time-dependent outcome influenced by different factors, including diet, physical activity, disease progression, and medication adherence. It is also limited by the presence of some medical conditions that affect its accuracy, such as renal failure, hemolytic anemia, or iron and folate deficiencies, which can lead to falsely low or high levels.11,34,35 Comorbidities often necessitate additional therapies, which can increase regimen complexity and complicate diabetes management. 36 Second, differences in study design, particularly the timing of outcome measurement, could contribute to divergent results. For example, two studies measuring HbA1c after more than 1 year reported a negative impact of higher MRC.26,27 A potential explanation for this negative impact could be attributed to having chronic cases of diabetes where patients become less adherent to their medications over time, yet receive more medication to control the progression of their diabetes, which consequently worsens their glycemic control. Previous studies have supported this theory, finding that patients with acute illnesses have higher adherence rates to their medication compared to those with chronic diseases, especially in the long-term use of medication (i.e., after the first 6 months of medication initiation).37,38 Third, heterogeneity in how MRC is defined or operationalized, such as focusing only on dosing complexity versus including monitoring and drug interactions, may also lead to variation in observed outcomes. 39 Lastly, factors such as the type of healthcare provider administering the intervention and the duration of treatment may also contribute to variations in glycemic control across the studies. These differences highlight the need for standardized measures of MRC and comprehensive assessments that consider patient-specific, clinical, and methodological factors.
While this review highlighted the association between higher MRC scores and poor glycemic control, it did not adequately account for confounders such as medication adherence. Only a few studies assessed changes in glycemic outcomes and medication adherence concerning MRC. In those studies, the impact of regimen complexity on clinical outcomes remained inconclusive due to the absence of direct clinical outcome evaluations. This review noted that nonadherence was more common among patients with high MRCI scores.20,36 However, MRCI scores do not capture all the elements that affect adherence and glycemic control. Notably, studies measuring adherence focused on dosing-related domains, such as once-daily dosing, fixed-dose combinations, or single tablet regimens. These domains may not necessarily impact glycemic control in the same way, suggesting that different aspects of complexity may affect these outcomes differently.
Recommendation for practice (treatment intensification between benefits and challenges)
The new evidence and recommendations emphasized the need for intense medication regimens for patients with diabetes, especially those not meeting their treatment goals. 4 Such an approach would positively impact healthcare utilization and patients. A one-decade study conducted in the United States reported an association between healthcare service utilization and MRC. 40 There was a significant annual increase in the number and duration of primary care visits (longer than 20 min) for patients with diabetes using more than five prescribed medications. The increased number of visits was associated with oral use of antidiabetic medication, while patients using insulin regimens had a significantly decreased number of primary care visits. 40 Such findings highlight the need for regimen intensification and simplification to reduce the global pressure on physicians and the healthcare systems, which would impact achieving evidence-based diabetes care goals. Moreover, regimen simplification through extended-release formulations or newer drugs has directly benefited patients with diabetes by improving their symptoms, disease status, and outcomes, mainly medication adherence, QoL, treatment satisfaction, and costs. 33 These positive outcomes may be attributed to improved ease of use, reduced burden, and better perceived treatment control. Healthcare providers and researchers have also developed and implemented other interventions considering physician and patient behavior to improve prescription and medication intensification in uncontrolled diabetes.25,29,41 Improvement interventions were believed to consider reflective and impulsive behavior change approaches. 41 In addition, a collaboration between experts in general practice and diabetes found that organization-focused interventions were more effective than medication regimen modification or patient-centered interventions with direct patient engagement. 41 For example, professional-level strategies such as clinical decision support systems, collaborative team-based models (e.g., Diabetes Intense Medical Management program), and comprehensive medication review in the context of the best practice guidelines were believed to improve outcomes in patients with uncontrolled diabetes.25,29,41 Service developers and policymakers should understand key behaviors that necessitate appropriate treatment intensification before designing any intervention, and consequently, identify the key mechanisms to implement these interventions. According to the behavior change wheel theory, organization-focused interventions should be supported by different mechanisms to change the desired behavior (in this case, appropriate prescribing and regimen intensification); these are healthcare providers’ education and training, enablement, environmental restructuring, and incentivization.41,42
This rapid review provides a timely approach to evidence synthesis, but it has some limitations. A narrowed search strategy and simplified appraisal methods may introduce publication bias and reduce methodological rigor. Additionally, reliance on narrative synthesis rather than meta-analysis can limit comparability and generalizability. Furthermore, while our review examines the relationship between MRC and diabetes management, most included studies were observational, which limits our ability to infer causality. Cross-sectional studies, in particular, provide only a snapshot in time, identifying associations rather than definitive impact. Despite these limitations, this rapid review remains valuable for informing time-sensitive clinical and policy decisions.
Conclusion
This review underscores the importance of addressing concerns about MRC in diabetes management, as it is associated with various health outcomes that may impact treatment effectiveness. Higher MRC was generally associated with poorer glycemic control and medication adherence, greater treatment burden, and increased diabetes-related distress. Due to methodological heterogeneity across studies, including variations in populations, settings, study designs, and outcome measures, further research is needed to clarify how regimen complexity influences glycemic control. Nonetheless, our findings emphasize the need for healthcare providers to consider regimen simplification strategies where possible to enhance adherence and improve other patient outcomes. Incorporating simplification into clinical decision-making may also support more patient-centered care by reducing treatment burden and aligning therapy with individual patient needs and preferences. Future research should focus on standardizing outcome assessments and identifying subgroups most likely to benefit, thereby improving the understanding of the actual impact of MRC and informing strategies for optimizing diabetes treatment in both practice and policy.
Supplemental Material
sj-pdf-1-tae-10.1177_20420188251372294 – Supplemental material for The role of medication regimen complexity in diabetes management: a rapid review
Supplemental material, sj-pdf-1-tae-10.1177_20420188251372294 for The role of medication regimen complexity in diabetes management: a rapid review by Sarah M. Khayyat and Ruba S. Azfr Ali in Therapeutic Advances in Endocrinology and Metabolism
Supplemental Material
sj-pdf-2-tae-10.1177_20420188251372294 – Supplemental material for The role of medication regimen complexity in diabetes management: a rapid review
Supplemental material, sj-pdf-2-tae-10.1177_20420188251372294 for The role of medication regimen complexity in diabetes management: a rapid review by Sarah M. Khayyat and Ruba S. Azfr Ali in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.