
Abstract
Background:
Coronavirus disease 2019 pandemic pointed out significant mental symptoms of frontline healthcare workers (HCWs).
Objective:
We aimed to estimate the prevalence and comorbidity of post-traumatic stress symptoms (PTSS), depression and anxiety symptoms in HCWs from Fangcang shelter hospitals during the pandemic.
Design:
Demographic information, post-traumatic stress disorder checklist for DSM-5 (PCL-5), Patient Health Questionnaire (PHQ-9) and Generalized Anxiety Disorder Questionnaire (GAD-7) were obtained online based on stratified random sampling design during April 2022, with 284 eligible responses.
Method:
Hierarchical regression analyses were applied to investigate independent variables associated with psychological status outcomes (PHQ-9, GAD-7 and PCL-5), and the network analyses were applied to explore the comorbidity using all items of PCL-5, PHQ-9 and GAD-7.
Results:
(1) 10.56%, 13.03% and 8.10% of HCWs reported PTSS, depression and anxiety symptoms. Fifty-three (18.66%) HCWs experienced at least one mental health disorder, among which 26.42–37.74% HCWs had comorbidity of two or three mental disorders; (2) several influence factors of mental health were identified, including medical professions, working hours, contacted patients (p < 0.05); (3) prominent bridge symptoms between PTSS and depression were sleep problems, suicide ideation, concentration difficulties and recklessness. Comorbidity between PTSS and anxiety was thought to mainly stem from negative affect, such as afraid, anxious, annoyed and worrying. Depressed mood and worry might be good targets during treatment of comorbidity of depression and anxiety.
Conclusion:
Our data suggest mild level of PTSS, depression and anxiety symptoms among HCWs during the pandemic and might give novel insights into assessment and intervention of comorbidity.
Introduction
Exposure to traumatic events can lead to an increased risk of developing various psychiatric disorders, such as post-traumatic stress disorder (PTSD), depression and Generalized Anxiety Disorder (GAD).1,2 Co-occurrence of PTSD, depression and GAD is common,3,4 and patients with multiple psychiatric disorders tend to have a poorer prognosis, experience greater difficulty coping with daily life and even exhibit higher rates of suicide.2,5 Previous literature has found that diagnostic treatment for the comorbidity of two psychiatric disorders may be more effective than treating each disorder individually,6–8 which emphasized the need for exploring therapeutic targets for comorbidity of psychiatric disorders.
Previously research has indicated that people inevitably endured significant psychological distress during the Coronavirus disease 2019 (COVID-19) pandemic.9–11 Notably, due to the growing number of patients for receiving treatment and restrictions for infection control,12–16 frontline healthcare workers (HCWs) were at high risk of getting infected and suffering from mental symptoms such as post-traumatic stress symptoms (PTSS), anxiety and depression symptoms.17–23 A survey on PTSS among HCWs in China indicated a prevalence rate of 10.7% in the early stage of the COVID-19 pandemic. 24 Furthermore, a 1-year longitudinal study demonstrated a substantial increase in the prevalence rate of PTSS among HCWs from 10.7% to 20.8%, suggesting a deterioration over time. 25 Additionally, a nationwide large-scale survey focused on the mental health of HCWs in China revealed high levels of anxiety symptoms (16.0%) and depressive symptoms (34.6%) during the acute phase of the COVID-19 pandemic. 26 Meanwhile, another cross-sectional study on HCWs in China showed that within 1 month after the outbreak of COVID-19, rates for reporting anxiety or depression symptoms were found to be 44.6% and 50.4%, respectively. 27
Though co-occurrence of PTSS, anxiety and depression symptoms among HCWs during the pandemic has been noted in a wide range of studies,21,26 there remains very limited knowledge concerning the core symptoms and major pathways of these psychiatric disorders in HCWs that greatly benefit targeted and problem-focused treatment for comorbidity. Network analysis is an appropriate tool to explore the underlying structure of comorbidity in psychiatric disorders.2,6,8 The centrality of a symptom, which refers to its degree of connection with other symptoms in the network structure, serves as a primary indicator in network analysis. 28 Bridge symptom is another noteworthy indicator, as comorbidity is considered to be the result of a relationship between symptoms that connect two disorders.3,29 The activation of bridge symptoms causes the onset of symptoms from syndrome clusters, whereas suppressing these bridge symptoms is expected to prevent the appearance of other symptoms.30,31 Therefore, network analysis can provide a deeper understanding of comorbidity among HCWs during pandemics.
In this study, we employed HCWs from Fangcang shelter hospitals, which were built by transforming the exhibition centres or stadiums and could accommodate the growing number of patients for receiving treatment in isolation. In these high-stress environments, HCWs were more likely to perceive an exposure risk, and thus were more likely to screen positive for depression, stress and PTSD.21,22,32,33 Our objectives were three-fold: (1) to evaluate the psychological status of HCWs in Fangcang shelter hospitals during Omicron pandemic using the Generalized Anxiety Disorder Questionnaire (GAD-7), Patient Health Questionnaire (PHQ-9) and PTSD Checklist for DSM-5 (PCL-5); (2) considering that previous researches revealed that nurses (versus doctors), women (versus men), younger and HCWs with lower education had relatively higher percentages of having psychiatry disorders,16,34,35 we also investigated potential factors influencing PTSS, depression and anxiety symptoms, such as medical profession, gender and age and (3) to explore underlying constructs of comorbidity between these mental disorders through network analysis. Firstly, we aimed to construct a comprehensive network encompassing all three disasters in order to reveal an integrated structure of interconnected symptoms. Secondly, the interplay between PTSS–depression, PTSS–anxiety and depression–anxiety were estimated while identifying specific bridge symptoms that could inform future trans-diagnostic treatments tailored towards HCWs during pandemics.
Methods
Study design and participants
This survey was conducted from 10 April to 20 April 2022 based on stratified random sampling design. We surveyed HCWs who worked in three Shanghai Fangcang shelter hospitals during the outbreak of Omicron. They volunteered to completed the closed survey on Web-based survey platform (https://www.wjx.cn/). All participants were asked to fill in the questionnaires anonymously, including demographic information (age, gender, education and medical profession), GAD-7, PHQ-9, PCL-5 as well as working hour and working intensity. All items in the questionnaire are mandatory to answer, and participants were able to review and modify their answers.
The sample size was calculated with α set as 0.05, β set as 0.20 and according to the previous studies that the prevalence of PTSS, depression and anxiety were 22.60%, 34.60% and 16.0%,16,36 respectively, a minimum of 277 participants were required for this study. All HCWs who were medical professionals in the designated hospitals and working during the Omicron outbreak were eligible for participation. Considering 80% response rate, 348 patients were planned to recruit by stratified random sampling method from 4 medical team in Fangcang shelter hospital in Shanghai, a table of random numbers is used to randomly select 87 HCWs from each medical teams. Participants were excluded if they were unwilling to accept the investigation (n = 61, response rate was 82.47%) or had a response time <60 s or >30 min for completing the questionnaire (n = 3). Finally, 284 participants completed the questionnaire and were included in this study (see Figure 1). Each participant was required to fill the questionnaire only once by checking their IP addresses, survey never displayed a second time once the user had filled it in.

Flowchart of the enrolment of participants from Fangcang shelter hospital during the Omicron outbreak in Shanghai.
Measures
PTSS
PCL-5 was applied to assess the PTSS of HCWs in Fangcang shelter hospitals. This scale consisted of 20 items and measured the PTSS severity by rating on a Likert scale from 0 (not at all) to 4 (extremely).37,38 Previous studies reported that 33 was valid cut-off point for identifying potential PTSD.36,39 The scale indicated excellent internal consistency in the present study (Cronbach’s α = 0.900).
Depression
PHQ-9 is a nine-item scale for assessing depression severity. Each item was scored on a 0–3 point scale from 0 (not at all) to 3 (almost every day). 40 Setting 10 as cut-off points was reported to have high clinical sensitivity and specificity in depression. 41 Internal consistency of PHQ-9 in our samples was excellent (Cronbach’s α = 0.924).
Anxiety
General anxiety disorder was measured by employing GAD-7. 42 Participants were asked to evaluate their anxiety symptoms by rating on 4-point scale, with score from 0 (not at all) to 3 (almost every day). 43 The study revealed that scores over 10 were shown to have moderate to severe anxiety symptoms. 44 Thus, the cut-off point of the current study was set as 10. The scale indicated excellent internal consistency in our dataset (Cronbach’s α = 0.96).
Working hour and working intensity
Working hour was measured with a single item, ‘What is your average working hour now’, the item was rated on ‘less than 4 h’, ‘4–6 h’, ‘more than 6 h’ and change of working intensity was measured with ‘How was your working intensity since entering the Fangcang shelter hospital’, the item was rated on ‘as usual’, ‘increased’, ‘decreased’ and ‘a lot’.
Data analysis
Hierarchical regression analyses were applied to investigate independent variables associated with psychological status outcomes (PHQ-9, GAD-7 and PCL-5). Specifically, three hierarchical regression analyses were conducted for PHQ-9, GAD-7 and PCL-5 scores, respectively, which were added as the dependent variables. Previous study on HCWs revealed that females, younger, HCWs with lower education background and doctor (versus nurse) might have higher risk of developing PTSS. 16 Thus, these demographics were added as independent variables into Model 1. Moreover, in Model 2, we focus on the independent impact of working hour and working intensity on mental health of HCWs (see Table 2).
Furthermore, network analysis of PTSS, depression and anxiety were performed by employing the bootnet package in R Studio. 45 The network was modelled with the 20 items of PCL-5, the nine items of PHQ-9 and the seven items of GAD-7. Every symptom was treated as a node of the network structure. The graphical Gaussian model was applied for calculating pairwise association between nodes, and the coefficients partial correlation between nodes were called edges. The edge weight ranges from −1 to 1, the negative and positive of the values present the directions of correlations.28,31 Additionally, we aimed to identify bridge symptoms in the network of PTSS–depression and PTSS–anxiety, depression–anxiety. The bridge strength is the sum of edge weight of all interconnection edges across two disorders.5,29 In each network, we reported standardized z score of the bridge strength (above 80th percentile) and edge weight between nodes (above 0.1).8,29 The Fruchterman and Reingold 46 algorithm was used to layout the network with a gamma hyperparameter of 0.30; the stronger the edge weight, the closer the nodes were placed.
To test the stability of the edge weights and the centrality indices, a case-dropping bootstrap with 1000 samples was applied to plot their 95% confidence intervals and to calculate the correlation stability coefficient (CS-coefficient). The lowest accepted value of the coefficient is 0.25, and above 0.5 is preferable. 15 The CS-coefficient denotes the maximum number of cases that can be dropped to preserve a correlation of at least 0.70 between centrality indices based on the original network and those computed with less cases. 47
See Supplemental Material for all R code for four network analyses in the present study. The reporting of this study conforms to the checklist for reporting results of internet E-Surveys (CHERRIES) statement. 48
Results
Description of sample
The entire sample comprised 284 HCWs from Fangcang shelter hospitals, the mean age was 33 years old (SD = 7.01). A large proportion of the HCWs were women (72.54%, n = 206). About two-thirds were nurses (69.37%, n = 197), and 26.41% of participants were doctors (n = 75); 181 (63.73%) of HCWs had university degrees, and 33 (11.62%) of them had master’s degrees and 38 (13.38%) of them had higher education backgrounds (Table 1).
Demographic and disease-related characteristics of the HCWs.
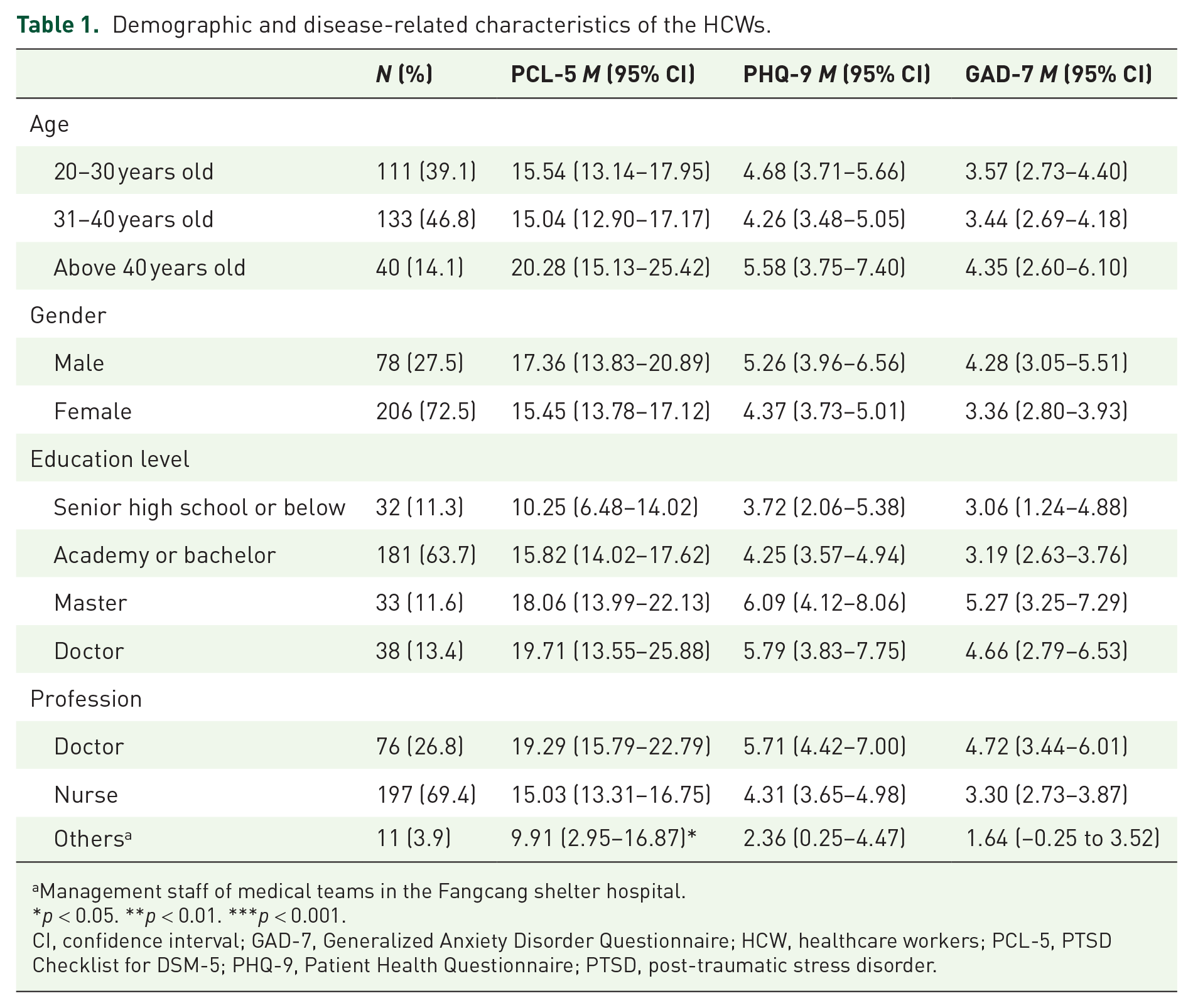
Management staff of medical teams in the Fangcang shelter hospital.
*p < 0.05. **p < 0.01. ***p < 0.001.
CI, confidence interval; GAD-7, Generalized Anxiety Disorder Questionnaire; HCW, healthcare workers; PCL-5, PTSD Checklist for DSM-5; PHQ-9, Patient Health Questionnaire; PTSD, post-traumatic stress disorder.
Anxiety, depression and post-traumatic stress symptoms
According to the recommended cut-off points of corresponding scales, 10.56% (n = 30), 13.03% (n = 37) and 8.10% (n = 23) of participants reported PTSS, depression and anxiety symptoms. Besides, 53 (18.66%) HCWs who reported experiencing at least one of these mental health disorders, among which a quarter of them (24.53%, n = 13) had PTSS–depression–anxiety combined symptoms, and 30.19% (n = 16), 26.42% (n = 14), 37.74% (n = 20) reported experiencing PTSS–depression, PTSS–anxiety, depression–anxiety combined symptoms. Spearman’s correlation analyses revealed that the scores of PTSS was positively correlated to the anxiety and depression (r = 0.73, p < 0.001; r = 0.78, p < 0.001), and the scores of anxiety symptoms was positively correlated to depression symptoms in these samples (r = 0.80, p < 0.001).
The influence factors of psychological status
We used the hierarchical regression analysis to estimate the independent influence factors for mental health status of HCWs. The results are shown in Table 2. Doctors have more severe PTSS, depression and anxiety symptoms than nurses (p < 0.05), and HCWs who contacted with patients were more likely to develop depression, anxiety and PTSD symptoms (p < 0.01). In Model 2, work hour was significantly positively correlated with PTSS (β = 3.25, p < 0.01), depression (β = 2.97, p < 0.01) and anxiety (β = 3.20, p < 0.01). The work intensity was significantly positively correlated with PTSS (β = 2.53, p < 0.05).
Regression analysis with the PCL-5, GAD-7 and PHQ-9 as the outcome variable.
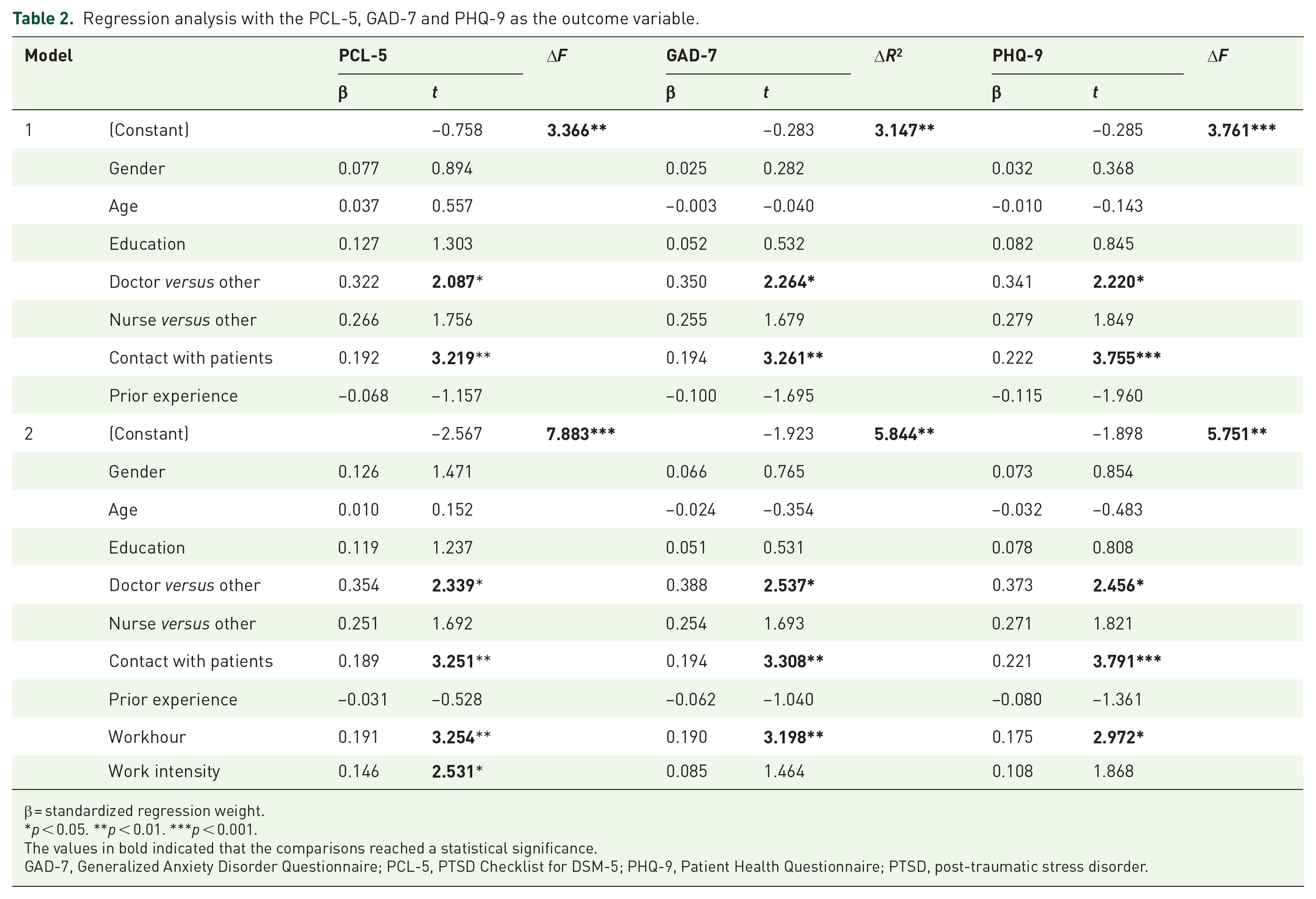
β = standardized regression weight.
p < 0.05. **p < 0.01. ***p < 0.001.
The values in bold indicated that the comparisons reached a statistical significance.
GAD-7, Generalized Anxiety Disorder Questionnaire; PCL-5, PTSD Checklist for DSM-5; PHQ-9, Patient Health Questionnaire; PTSD, post-traumatic stress disorder.
Network analysis
Network stability
The strength stability with case-dropping subset bootstrap 95% confidence intervals was good in the complete network (CS = 0.60), PTSS–depression network (CS = 0.60) and PTSS–anxiety network (CS = 0.67), increasing confidence in drawing conclusions from these cross-sectional networks. But, the strength stability of depression–anxiety network was below 0.5 (CS = 0.36); thus, the results of this network should be interpreted with caution as it is not highly stable 28 (see Supplemental Figures S1–S4).
The complete network
As illustrated in Figure 2, overall, the complete networks indicated that connections between symptoms within each disorder were stronger [see Figure 3(a)]. In terms of centrality index, the strength of each node was shown as standardized z scores [see Figure 2(b)], P7 (Avoiding reminders) had the highest strength, normalized strength (NS) = 1.92, followed by A2 (Not being able to stop or control worrying), NS = 1.46, P18 (Jumpy), NS = 1.33, A6 (Becoming easily annoyed or irritable), NS = 1.21 and P14 (Trouble experiencing positive feelings), NS = 1.01, in descending sequence. See Supplemental Table S1 for values of all nodes.

Network structure of PTSS, depression and anxiety (a), and the centrality index of the network structure (b). The items of PTSS, depression and anxiety were labelled in black, grey and white, respectively. Thickness of connection lines represented the edge weight. The positive and negative connections were marked by solid lines and dashed lines, respectively.

Network analyses between PTSD and depression (a), PTSD and anxiety (c), depression and anxiety (e). The network structure was on the left, the bridge strength was on the right. The items of PTSS, depression and anxiety were labelled in black, grey and white, respectively. Thickness of connection lines represented the edge weight. The positive and negative connections were marked by solid lines and dashed lines, respectively. See Figure 2 for the full name of each node.
PTSS–depression network
Bridge strength of each node was showed in Figure 3(b). The nodes with relatively high bridge strength in descending order were: P20 (Sleep problems), normalized bridge strength (NBS) = 2.12; slightly below which were: D3 (Sleep problems), NBS = 2.06; D9 (Suicide ideation), NBS = 1.84; P19 (Concentration difficulties), NBS = 1.56; P16 (Recklessness), NBS = 1.34 and D1 (Anhedonia), NBS = 0.99. As shown in Figure 3(a), the strongest relative bridge connections in sequence were: P20 (Sleep problems) and D3 (Sleep problems), edge weight = 0.44; P16 (Recklessness) and D9 (Suicide ideation), edge weight = 0.28; P19 (Concentration difficulties) and D4 (Low energy), edge weight = 0.13; P19 (Concentration difficulties) and D7 (Trouble concentrating), edge weight = 0.11; P19 (Concentration difficulties) and D1 (Anhedonia), edge weight = 0.10. See Supplemental Material for values of all NBS (Supplemental Table S5) and edge weight between nodes (Supplemental Table S2).
PTSS–anxiety network
Figure 3(d) showed the bridge strength of each node. The nodes with relatively high bridge strength in descending order were: A7 (Feeling afraid as if something awful might happen), NBS = 2.36; A1 (Feeling nervous, anxious or on edge), NBS = 1.86; A6 (Becoming easily annoyed or irritable), NBS = 1.43; A2 (Not being able to stop or control worrying), NBS = 1.38; P18 (Jumpy), NBS = 1.30 and P17 (Hypervigilant), NBS = 1.15. As shown in Figure 3(c), the strongest relative bridge connections in sequence were: P17 (Hypervigilant) and A7 (Feeling afraid as if something awful might happen), edge weight = 0.10; P18 (Jumpy) and A7 (Feeling afraid as if something awful might happen), edge weight = 0.09; P17 (Hypervigilant) and A2 (Not being able to stop or control worrying), edge weight = 0.08; P14 (Trouble experiencing positive feelings) and A7 (Feeling afraid as if something awful might happen), edge weight = 0.07; P13 (Feeling detached) and A3 (Worrying too much about different things), edge weight = 0.06. See Supplemental Material for values of all NBS (Supplemental Table S5) and edge weight between nodes (Supplemental Table S3).
Depression–anxiety network
The nodes with relatively high bridge strength in descending order were: A6 (Becoming easily annoyed or irritable), NBS = 2.61; D2 (Depressed), NBS = 1.05, A1 (Feeling nervous, anxious or on edge), NBS = 1.02 [see Figure 3(f)]. As shown in Figure 3(e), the strongest relative bridge connections in sequence were: D2 (Depressed) and A2 (Not being able to stop or control worrying), edge weight = 0.13; D8 (Psychomotor problems) and A6 (Becoming easily annoyed or irritable), edge weight = 0.13; D3 (Sleep problems) and A1 (Feeling nervous, anxious or on edge), edge weight = 0.13; D4 (Low energy) and A1 (Feeling nervous, anxious or on edge), edge weight = 0.10; D2 (Depressed) and A1 (Feeling nervous, anxious or on edge), edge weight = 0.10. See Supplemental Material for values of all NBS (Supplemental Table S5) and edge weight between nodes (Supplemental Table S4).
Discussion
The rapid transmission of the Omicron variant in March 2022, Shanghai, China posed a significant threat to frontline HCWs. Though physical care of HCWs was greatly improved by accepting vaccination, which played a major role in staff and patient safety, workforce capacity and patient uptake,49–51 our data suggested that the acute tremendous stress during the Omicron pandemic might lead to rapid changes in psychological status among HCWs in Fangcang hospitals. We further explored comorbidity by analysing the interconnectedness of symptoms using a network analysis approach. With network analysis, we identified potential central symptoms of three disasters. Furthermore, we conducted separate network analyses for PTSS–depression, PTSS–anxiety and depression–anxiety to identify bridge symptoms and potential pathways connecting these symptoms to others.
Firstly, this study examined the short-term impact of this pandemic on HCWs’ mental health in Fangcang shelter hospitals, 10.56%, 8.10% and 13.03% of HCWs reported PTSS, depression and anxiety symptoms, respectively. The prevalence rate of PTSS in our current sample was closely aligns with rates reported in previously studies focusing on the HCWs during the 3–5 months following COVID-19 outbreaks (7–10%).24,26 In comparison to a previous survey conducted during the initial stage of the COVID-19 pandemic in China, the prevalence of depression and anxiety symptoms among HCWs in our present sample was relatively low. Additionally, 53 HCWs reported experiencing at least one mental health disorder, with 26.4–37.7% of them having two or three comorbidities of mental disorders. These findings supported existing research indicating that individuals who suffered from PTSS are at a higher risk for developing depressive disorder and anxiety.2,6–8 Meanwhile, regression analyses revealed a positive correlation between HCWs’ working hours and their PTSS, depression and anxiety symptoms. Our findings emphasized that the potential threat to HCWs’ mental health caused by overwork and insufficient sleep still needed to be intervened,52,53 such as digital cognitive behaviour therapy, which was most evidence-based treatment to overcome insomnia and could be practiced online.54–56
Furthermore, we conducted network analyses to investigate the comorbidity of PTSS, depression and anxiety symptoms among HCWs during the Omicron pandemic. Initially, through a comprehensive network analysis encompassing all PTSS, depression and anxiety items, ‘Avoiding reminders’ within PTSS and ‘Not being able to stop or control worrying’ within anxiety symptoms were highlighted as central symptoms. Consistent with previous research findings, the symptom of ‘Not being able to stop or control worrying’ in anxiety was identified as a potentially core symptom. 57 The presence of these symptoms might play a central role in triggering other psychological symptoms, indicating their potential as specific indicators of comorbidity among HCWs during the pandemic.
Secondly, network analyses were employed to identify bridge symptoms interactions between PTSS and depressive items, PTSS and anxiety items, as well as anxiety and depressive items. In the PTSS–depression network, the prominent bridge symptoms included ‘sleep problems’ (a shared symptom of two diseases), ‘suicide ideation’ of depression and ‘concentration difficulties’, ‘recklessness’ of PTSS Cluster-E (hyper-arousal). Previous network analysis studies also identified sleep problems and concentration issues as bridge symptoms within the PTSS–depression network.6,58,59 These results highlighted the interconnectedness between depression symptoms and Criterion E of PTSD among HCWs. Notably, the ‘suicide ideation’ was the highest node, and the strongest connection was observed between ‘suicide ideation’ from depression and the ‘recklessness’ from PTSS. These findings suggested that the presence of severe PTSS among HCWs might potentially trigger suicidal behaviours, and targeting the symptom of ‘recklessness’ could be effective in identifying individuals at risk for suicide.
In terms of the PTSS–anxiety network, all four prominent bridge symptoms were anxiety-related: ‘Feeling afraid as if something awful might happen’, ‘Feeling nervous, anxious or on edge’, ‘Becoming easily annoyed or irritable’, ‘Not being able to stop or control worrying’. These findings provide support for previous research indicating that the co-occurrence of anxiety and PTSS may stem from negative emotions such as fear, anxiety, irritability and worry.2,60 Furthermore, several strong connections were observed: ‘Feeling afraid’ and ‘Hypervigilant’, ‘Feeling afraid’ and ‘Jumpy’, ‘Not being able to stop or control worrying’ and ‘Hypervigilant’. It is plausible that HCWs repeated exposure to traumatic events like witnessing patients’ suffering or death could amplify feelings of fear and worry, leading to heightened interconnections between these anxiety symptoms and the hyperarousal cluster (Criterion E) of PTSS.61,62 Therefore, combining the network analysis results of PTSS–depression and PTSS–anxiety, our data suggested that Criterion E of PTSS should figure high on the list of priorities for assessment and intervention comorbidity of psychiatric disorders in HCWs.
The results of depression–anxiety network should be interpreted with caution due to the instability of the coefficient of strength. The bridge symptoms of ‘Becoming easily annoyed or irritable’ in anxiety, and ‘Depressed’ in depression was highlighted, which was also found to be the highest nodes in bridge strength in early studies. 8 These symptoms might serve as effective targets during treatment for comorbidity of depression and anxiety. Another concern in this network was that depressed mood and worry also most strongly connected symptoms across these two disorders. Consistent with common conceptualizations of anxiety and depression, these two symptoms were considered core symptoms of these disorders,60,63 suggesting that the persistent worry of HCWs had some activating effect on depressed feeling, which might be good target in interventions.
There are several limitations to consider, including lack of generalizability to other healthcare workers (HCWs), the absence of measurement for COVID-19 burnout and the use of cross-sectional data which prevents causal inference.59,64 Future research could employ larger-scale follow-up data to compare samples with comorbidity and subthreshold comorbidity to examine possible differences in network structures and explore causal relations.
Conclusion
In conclusion, this study provided a snapshot of the psychological status of HCWs in Fangcang shelter hospital under acute overwhelming stress during the Omicron pandemic. Our findings suggest that 10.56% HCWs might suffer from PTSD, whereas 8.10% and 13.03% might experience symptoms of anxiety and depression, respectively. Furthermore, this study is the first to explore comorbidity of psychiatric disorders in HCWs from Fangcang shelter hospitals by a symptom-level analysis and might give novel insights into assessment and intervention of comorbidity of psychological disorders in HCWs, suggesting that Criterion E of PTSS should be a top priority for assessing and treating comorbidity of psychiatric disorders in HCWs.
Supplemental Material
sj-docx-1-tpp-10.1177_20451253241243292 – Supplemental material for Network analysis of the comorbidity between post-traumatic stress, depression and anxiety symptoms among frontline healthcare workers during the COVID-19 pandemic
Supplemental material, sj-docx-1-tpp-10.1177_20451253241243292 for Network analysis of the comorbidity between post-traumatic stress, depression and anxiety symptoms among frontline healthcare workers during the COVID-19 pandemic by Hui Ouyang, Lili Wu, Wenjie Yan, Keyi Si, Hongli Lv, Jingye Zhan, Jing Wang, Yanpu Jia, Zhilei Shang, Wenfang Chen and Weizhi Liu in Therapeutic Advances in Psychopharmacology
Supplemental Material
sj-docx-2-tpp-10.1177_20451253241243292 – Supplemental material for Network analysis of the comorbidity between post-traumatic stress, depression and anxiety symptoms among frontline healthcare workers during the COVID-19 pandemic
Supplemental material, sj-docx-2-tpp-10.1177_20451253241243292 for Network analysis of the comorbidity between post-traumatic stress, depression and anxiety symptoms among frontline healthcare workers during the COVID-19 pandemic by Hui Ouyang, Lili Wu, Wenjie Yan, Keyi Si, Hongli Lv, Jingye Zhan, Jing Wang, Yanpu Jia, Zhilei Shang, Wenfang Chen and Weizhi Liu in Therapeutic Advances in Psychopharmacology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.