
Abstract
Introduction
The SARS-CoV-2 pandemic has had a considerable impact, causing millions of deaths worldwide, including many healthcare workers (HCWs). The pharmaceutical industry has been working diligently since the start of the pandemic to develop various vaccines to fight the spread of the virus and protect the population.
Objective
To study the seroprevalence of neutralizing anti-SARS-CoV-2 antibodies in vaccinated HCWs at the Mohamed VI University Hospital in Marrakech and to determine the parameters that can influence immune response.
Methods
A cross-sectional study of 138 HCWs was performed between October and December 2021 by measuring IgG antibodies directed against the spike antigen of SARS-CoV-2 using an Abbott Architect® SARS-CoV-2 IgG II assay.
Results
The mean age was 31.42 years, the sex ratio was 2.94 women to each man, and the overall prevalence was 97%. We found 39.5% of the participants had experienced COVID-19 infections pre-vaccination, which decreased to 26.8% after vaccination. Neutralizing antibody titers were dependent on the type of vaccine: they were higher with the Pfizer-BioNTech vaccine, the number of doses (p < .001), and post-vaccine COVID-19 form. The post-vaccine COVID-19 infection rates were lower with the Sinopharm vaccine.
Conclusion
Heterologous vaccination with non-mRNA and mRNA vaccines and the consideration of post-vaccination COVID-19 infection as a booster could help optimize vaccine results while reducing potential side effects.
Introduction
In December 2019, a severe pneumonia cluster caused by a novel coronavirus species, SARS-CoV-2, was identified in the city of Wuhan, China. 1 The World Health Organization (WHO) assigned the name COVID-19 to the disease caused by this strain in February 2020.
The impact of the SARS-CoV-2 pandemic has been considerable. It has been responsible for millions of deaths worldwide, including many among healthcare workers (HCWs), who are at a higher risk of infection than the general population due to their regular exposure to COVID-19-positive patients. 2
Since the beginning of the pandemic, laboratories have been working to find solutions for this disease. Many vaccines have been developed to generate an immune response against viral spike antigens and to develop spike-neutralizing antibodies.3–5 However, the immunity provided by vaccines varies between patients and decreases over time, lasting only several months. 5
In Morocco, the vaccination program against COVID-19 began on 28 January 2021, and three types of vaccines have been used (BBIBP-CorV from Sinopharm, Oxford/AstraZeneca ChAdOx1 nCoV-19, and Pfizer-BioNTech BNT162b2). The vaccines are administered in two doses 4 weeks apart, and a third booster dose is offered 6 months after the second dose.
The aim of our study was to determine the seroprevalence of SARS-CoV-2-neutralizing antibodies in vaccinated HCWs at Mohamed VI University Hospital in Marrakech and to determine their level of protection as well as parameters that can influence the immune response.
Methods
This cross-sectional seroprevalence study included HCWs at Mohamed VI University Hospital in Marrakech between 20 October and 20 December 2021. The inclusion criteria for enrollment in the study were the following: Complete vaccination according to the national vaccination program against COVID-19, absence of COVID-19 suggestive symptoms, and completion of an online survey. The exclusion criteria were the following: Incomplete vaccination according to the national vaccination program against COVID-19, presence of respiratory symptoms suggestive of COVID-19 during the preceding week, and an incomplete online survey.
>All stages of this study were performed in accordance with the fundamental principles of medical ethics, in conformity with the Declaration of Helsinki. Written informed consent was obtained from all of the patients.
The participants then underwent serological tests. Blood samples were collected in dry tubes and centrifuged at 3000 r/min for 5 min.
Quantitative serology testing (Abbott Architect® SARS-CoV-2 IgG II Assay) was performed according to the manufacturer’s protocol, on the Abbott Architect® i1000SR using chemiluminescent microparticle immunoassay technology targeting IgG antibodies directed against the spike antigen, and samples were considered positive for antibody titers higher than 50.0 AU/mL.
Statistical analysis
Categorical variables were expressed as absolute and relative frequencies (%), and quantitative variables were expressed as medians and means. Various statistical tests were used to analyze the relationships between the different groups. The tests used were χ2, Student’s t, Fisher’s exact, and Spearman’s tests.
Statistical analysis was performed using IBM® SPSS Statistics V25, and p‐values < .05 were considered statistically significant.
Results
Main characteristics of participants: the main age group was between 30 and 45 years old, the majority was blood type O+, and the most frequent associated pathology was asthma.

COVID-19 in vaccinated HCW: the number of cases of infection has decreased with vaccination, but the clinical forms do not seem to be modified.

Neutralizing anti-SARS-CoV-2 median titer and post-vaccine COVID-19 infection in the different vaccine groups: antibody titers are higher in patients vaccinated with Pfizer-BioNTech and in those who received the third dose.
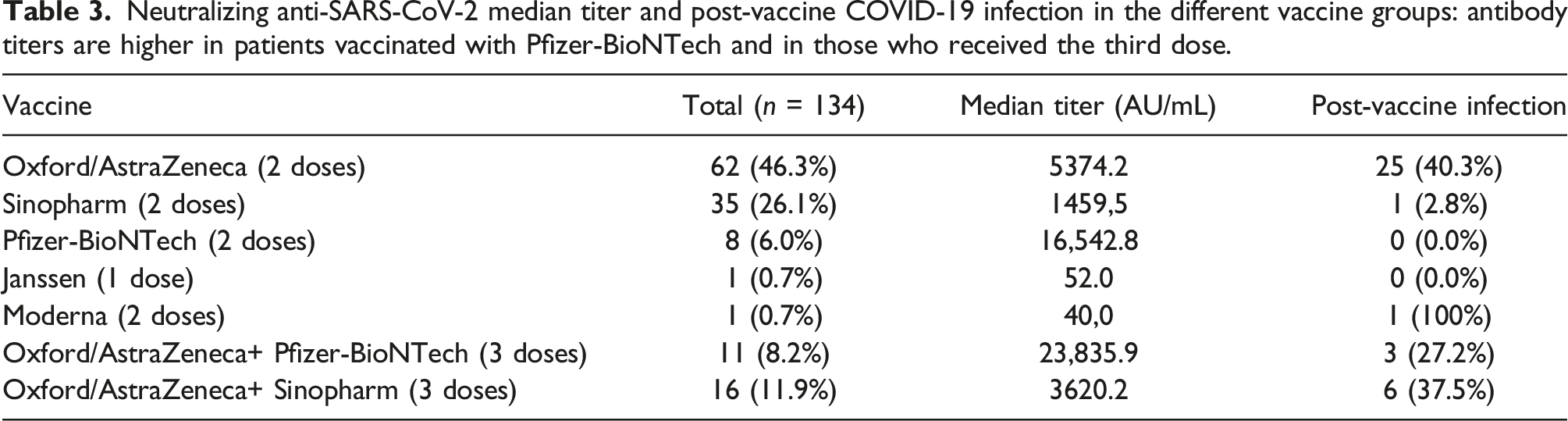
In 26.1% of cases, the participants had a post-vaccine COVID-19 infection. There was no significant difference between the percentage of pre- and post-vaccine clinical forms (p = .572). The median delay between the second dose administration of the vaccine and the post-vaccine infection was 3.9 months. Post-vaccination COVID-19 episodes were more frequent in the group vaccinated with two doses of Oxford/AstraZeneca (p < .0001) (Table 3).
The quantitative determination of the neutralizing anti-SARS-CoV-2 antibodies was positive in 97% of the cases, and the median antibody titer was 6543 AU/mL. The antibody titer was statistically correlated with vaccine type (p = .004) and the number of doses (p < .001); meanwhile, it was lower with Sinopharm than with other vaccines (Figure 1). Neutralizing antibody titers were higher in HCWs post-COVID infection (Table 4). In fact, the titers were proportional to the severity of the post-vaccination infection (Figure 2). Neutralizing anti‐SARS‐CoV‐2 anti-spike antibody titers in the different vaccine groups: the highest antibody titers were found in HCW vaccinated with Pfizer-BioNTech and the lowest in those vaccinated with Sinopharm. Median antibodies titer in HCW with history of COVID-19: neutralizing antibody titers are higher in HCW with post-vaccination COVID-19 infection. Neutralizing anti‐SARS‐CoV‐2 anti-spike antibody titers in post-vaccine infection group: the antibody titer is proportional to the severity of the post-vaccination COVID-19 episode.


Discussion
In this study, samples were collected from 134 participants to estimate the seroprevalence of neutralizing anti-SARS-CoV-2 antibodies in HCWs at Mohamed VI University Hospital of Marrakech.
Regarding the serology testing kit, the Abbott Architect® SARS-CoV-2 IgG II Assay kit presents a strong correlation with virus neutralization tests. In fact, this assay presents one of the highest sensitivities and specificities for automated quantitative immunoassays. 6
Our study has shown that 39.5% of the HCWs had tested positive for COVID-19 before vaccination, and the COVID-19 rates among the HCWs varied from 34.7% to 68.2%. 7 We have shown that the risk of COVID-19 infection is higher among HCWs and that this is related to patient contact. 8 Indeed, our results showed no significant difference between the pre- and post-vaccine clinical forms (p = .572). However, the COVID-19 rate decreased to 26.8% after vaccination, which is in line with results reported in the literature. Various studies have shown evidence to support the major effects of vaccination on reducing the rate of infection and shortening the duration of illness and viral clearance, which reduces the number of infections and days of sick leave.9,10 This therefore implies vaccination has a positive impact on the healthcare system.
Although the sample size is not representative, the results show that the neutralizing antibody titers in our series were dependent on the type of vaccine; the highest titers were observed with the Pfizer-BioNTech vaccine and the lowest with the Sinopharm vaccine. Studies agree that mRNA vaccines demonstrate a superior ability to induce humoral response by producing more anti-spike antibodies.11,12 In addition, the Pfizer-BioNTech vaccine has demonstrated superior quantitative efficiency when compared to the Sinopharm vaccine. 13
The antibody titers were also correlated with the number of doses (p < .001). They were higher in HCWs who received a booster dose and 2.36 times higher in those with post-vaccine COVID-19 episodes that occurred on average 3.9 months after the second dose. In fact, the humoral immunity efficiency progressively decreased after vaccination to reach only 34–80% after 6 months. This highlights the importance of a booster dose to increase antibody titers and improve the humoral defense by restoring vaccine efficacy.14,15 Subjects convalescing from COVID-19 developed a protective humoral response for up to 9 months,16,17 which may be comparable to the booster dose effect.
In this study, although the production of neutralizing antibodies was lower in HCWs vaccinated with the Sinopharm vaccine, post-vaccine COVID-19 infection was observed in only one subject. This may be due to the effectiveness of the cellular immunity provided by the vaccination. Indeed, while the humoral response declines over time, the T-cell response persists longer, offering more durable protection. 18
Heterologous administration of non-mRNA and mRNA vaccines has demonstrated superior efficacy in developing both humoral and cellular immunity and this study has proved their complementarity.12,19,20 In our study, HCWs who had received three heterologous doses (two Oxford/AstraZeneca doses + one Pfizer-BioNTech dose) showed 6.5 times higher neutralizing antibody titers than those with three homologous doses (two Oxford/AstraZeneca doses + one Sinopharm dose).
The main limitations of this study were related to the absence of RT-PCR for the detection of possible COVID-19 infections, the low representation of some types of vaccines, and the small sample size. Furthermore, this study included only HCWs who agreed to share their data. However, the sample size was representative of different categories of HCW from various departments.
Conclusion
As vaccination remains a powerful tool against the COVID-19 pandemic, the immune response to vaccines depends on multiple factors. The use of heterologous vaccination combining non-mRNA and mRNA vaccines and the consideration of post-vaccination COVID-19 infection as an immune booster could help to optimize vaccine results while reducing any potential side effects. The results in this study can be used as the basis for large-scale studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The requirement for ethics approval to conduct this study was waived by the institutional review board. The study included only volunteer participants who agreed to share their data in this study.
Informed consent
Written informed consent was obtained from all subjects before the study.